


Tainá Scalfoni Fracaroli1; Lislaine Bomm2; João Luz Sodré2; Mário Chaves3; Marcela Benez4; Solange Cardoso Maciel Costa Silva5
Pyogenic granuloma is a common vascular proliferation that can be found on skin and mucous membranes. Its clinical presentation is that of a nodular, friable and erythematous lesion, with fast growth history. The nail bed pyogenic granuloma is generally related to onychocryptosis and trauma, being very painful in that site. There are several treatment options, including surgical excision, cryotherapy, electrocautery, curettage, lasers, application of trichloroacetic acid, imiquimod and microembolization. The present study reports a case of bilateral pyogenic granuloma in the halluces with exuberant growth, leading to the occlusion of the nail plate. The surgical excision of the lesion was performed with good cosmetic results.
Keywords: PYOGENIC GRANULOMA, SURGERY, TRICHLOROACETC ACID, CRYOTHERAPY.
Pyogenic granuloma or lobular capillary hemangioma is a benign vascular proliferation that occurs mainly in body sites exposed to frequent traumas, such as hands, arms, feet and face. From the clinical perspective, it is a nodular, or vegetating, friable lesion, varying in color from red to blackish-blue. It can be sessile or pedunculated and has a history of rapid growth. In general it bleeds with minimal trauma and tends to recur.1,2
Its etiology is still unknown, with factors such as trauma, viral infections, chronic ulcers and female sex hormones having been implicated. It may be also found in patients who are using isotretinoin, capecitabine or indinavir, due to the stimulus for angiogenesis.2,3
The diferencical diagnosis occurs mainly with Kaposi's sarcoma, amelanotic melanoma, metastatic carcinoma, inflamed seborrheic keratosis and eccrine poroma.4
The diagnosis is essentially clinical, with histopathological examination being useful to rule out other dermatoses. The main structure observed in the pyogenic granuloma is a lobular circumscribed aggregate of capillary proliferation within an edematous stroma, infiltrated by numerous neutrophils, with an often-eroded epidermis.1,3
There are several treatment options, including surgical excision, cryotherapy, electrocautery, curettage, lasers, application of trichloroacetic acid, imiquimod and microembolization.4-7
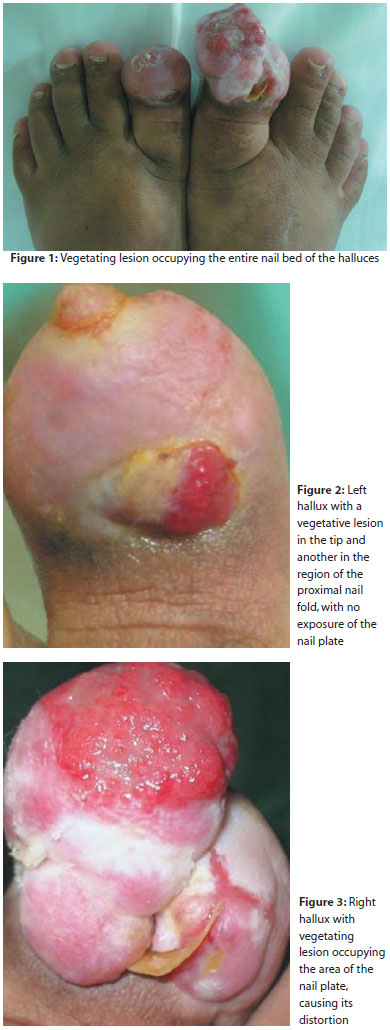
A 27-year-old female patient described the emergence of a vegetating lesion in the halluces 15 years before, followinga local trauma. The patient had already undergone topical treatment with partial improvement and surgical excision of the lesion, nonetheless it recurred a year before. There was occlusion of nai plates with the growth of the lesion. The lesion's histology was consistent with that of pyogenic granuloma.
The dermatological examination revealed a vegetative, erythematous, friable lesion of approximately 5x3cm in the right hallux, with distortion of the nail plate. In the left hallux were was observed small vegetative lesions on its tip and proximally in the nail fold, with complete epithelialization of the hallux and a complete lack of visualization of the nail plate (Figures 1 to 3). Radiographs and bone scintigraphy of the halluces were carried out, excluding the presence of osteomyelitis. A decision was made to carry out the surgical exeresis of the lesions, leading to good cosmetic results.
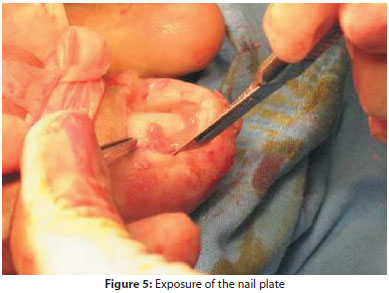
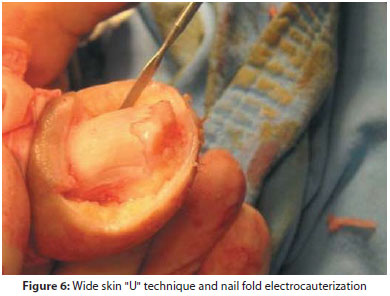
In the present case, the surgical excision was the best treatment option due to the size of the lesions and the fact that both halluces were affected. The asepsis and antisepsis were carried out. Nerve block anesthesiawith 2% lidocaine without vasoconstrictor and a tourniquet were applied to the hallux. The skin was incised with a number 15 scalpel blade in order to remove the vegetative lesion (Figure 4), which covered the left hallux entirely. After the removal of the lesion's tissue, the presence of the nail plate, which was beneaththe vegetative tissue, could be observed. The excision of the skin in the lateral nail folds was carried out in a wide "U" shape, in order to remove the hypertrophied hyponychium.8 The electrocauterization of the nail fold (Figures 5 and 6) and subsequent suture with 3.0 mononylon threads were carried out (Figure 7). The same procedure was then performed in the opposite hallux. The occlusive dressing was carried out with the patient being instructed to rest for 48 hours and cephalexin orally was used for seven days.
The post-operative follow up was conducted on a weekly basis, and the stitches removed 15 days after the procedure. The patient presented a good surgical outcome with no complications post-operatively. It was possible to observe the good cosmetic results (Figure 8) 30 days after the procedure. However, there was an increase of the right hallux's distal hyponychium, which was corrected with the application of 50% trichloroacetic acid and topical steroids. The patient is receiving outpatient treatment, with no recurrence of the lesion to the moment.
Some pyogenic granulomas subside spontaneously, however most require treatment. The nail pyogenic granuloma is usually the result of onychocryptosis or local trauma.3 It is a painful condition that prevents patients from carrying out daily activities. Pain and inflammation result from the penetration of the nail plate in the subcutaneous tissue. Surgical excision is a good therapeutic option because it offers low recurrence, heals the condition in one session and allows that the material be sent for histological examination. 2,4,8 In the present case, the pyogenic granuloma was so exuberant that the authors suspected that there had been destruction of the nail plate. With the surgical removal of the lesion, it was possible to visualize the nail, which had its growth hampered by the excess of overlying tissue. The surgical technique employed consisted of removing the vegetating lesion, associated with the wide "U" shaped technique, which features the elliptical removal of the skin of the distal lateral nail fold, with the posterior suture of the borders.8,9
Among the therapies available for treating pyogenic granuloma, the choice of the best treatment will depend on the specific case and on the experience of the physician in charge of the case.
1. Piraccini BM, BellavistaS, Misciali C, Tosti A, de Berker D, Richert B. Periungual and subungual pyogenic granuloma. Br J Dermatol. 2010; 163(5): 941-53.
2. Piraccini BM, Iorizzo M. Drug reactions affecting the nail unit: diagnosis and management. Dermatol Clin. 2007;25(2):215-21.
3. Lee J, Sinno H, Tahiri Y, Gilardino MS. Treatment options for cutaneous pyogenic granulomas: A review. J Plastic Reconstr Aesthet Surg. 2011;64(9):1216-20
4. Giblin AV, Clover AJ, Athanassopoulos A, Budny PG. Pyogenic granuloma – the quest for optimum treatment: audit of treatment of 408 cases. J Plastic Reconstr Aesthet Surg. 2007; 60(9):1030-5.
5. Goldenberg G, Krowchuk DP, Jorizzo JL. Successful treatment of a therapyresistant pyogenic granuloma with topical imiquimod 5% cream. J Dermatol Treat. 2008; 17(2): 121-3.
6. Bourguignon R, Paquet P, Pierard-Franchimont C, Pierard GE. Treatment of pyogenic granulomas with Nd- YAG laser. J Dermatol Treat. 2006; 17(4): 247–9.
7. Mirshams M, Daneshpazhooh M, Mirshekari A, Taheri A, Mansoori P, Hekmat S. Cryotherapy in the treatment of pyogenic granuloma. J Eur Acad Dermatol Venereol. 2006; 20(7): 788–90.
8. Rosa IP. Hipercurvatura transversa da lâmina ungueal ("pincer nail") e lâmina ungueal que não cresce, tratamento cirúrgico: remoção de "u" largo de pele, osteocorreção do leito e cicatrização por segunda intenção. Tese (Doutorado em Ciências). São Paulo: Escola Paulista de Medicina –Universidade Federal de São Paulo; 2005. 156 p.
9. Silva, SCMC. Cirugia Dermatológica teoria e prática. Dilivros. 2008.p. 362-4.
This study was carried out at the Department of Dermatology, Hospital Universitário Pedro Ernesto (UERJ) – Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}