


Poliana Santin Portela1; Felipe José da Cruz Oliveira2; Daniel Fabiano Ferreira3
Xanthelasma is a frequent complaint in dermatology, especially among women. Clinically, the condition has the appearance of flat or slightly raised yellowish plaques in the eyelid region. There are several procedures described for treating this condition. Blepharoplasty is the most commonly used technique to correct extensive xanthelasmas, particularly in patients with excess skin.
Keywords: XANTHOMATOSIS; BLEPHAROPLASTY; SURGICAL PROCEDURES, ELECTIVE.
Xanthelasma (from the Greek xanthos = yellow and elasma = metal plate) is a frequent complaint in dermatologic practices, especially among women. It is the most common type of plane xanthoma, and can indicate possible abnormalities in serum lipoprotein levels (occurring in approximately 50% of cases). There is deposition of xanthomatous cells in the superficial dermis, associated with inflammation and fibrosis.1 Clinically, it has the appearance of yellowish plaques, flat or slightly elevated, in the eyelid region.
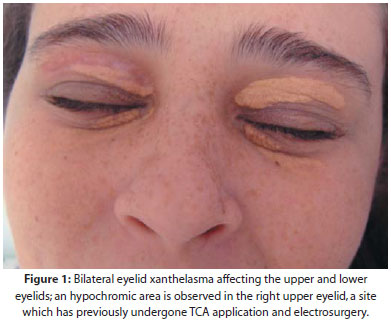
A 36-year-old female patient experiencing bilateral xanthelasma for three years (Figure 1). Previously treated with punctual electrocoagulation and application of 70% trichloroacetic acid (TCA), developing into residual hypochromia, she underwent surgical removal of the lesions through the blepharoplasty technique, with local anesthesia and removal of skin only, leaving the subcutaneous tissue untouched. Primary closure was carried out without the need to rotate the flap or implement grafts (Figures 2, 3, and 4). The procedure was performed without complications.
Several therapeutic options have been described for the treatment of xanthelasma. It is a difficult to manage condition because each method may be associated with undesirable side effects, such as hyper-or hypochromia, recurrence, persistence, and hypetrophic scarring. The most frequently used modalities are the chemical cauterization, fractional electrocoagulation, laser therapy, cryosurgery, and surgical excision.1, 3 – 8
Blepharoplasty – the generic term used to describe the surgical intervention carried out to remove excess skin of the upper and/or inferior eyelids – is the most commonly used technique to correct extensive xanthelasmas, particularly in patients with excess skin.3 The vast majority of procedures are carried out for aesthetic reasons – in order to reverse the effects caused by the aging of the skin 9 –nonetheless the technique has been employed to correct skin lesions located on the eyelids. The closure can be primary or, in the most exuberant cases, through flaps and grafts.
A rigorous assessment as to the amount of excess skin, texture, and laxity must be made from the outset, in order to achieve the correct surgical marking. The presence of scars, nevi and palpebral bags must also be taken into account.10 The surgical markings must not surpass the orbital region.
In the present surgical procedure, the marking was carried out narrowly and with with precision, bilaterally around the xanthomatous lesions. Anesthesia (2% lidocaine with vasoconstrictor) was applied locally, with the incision being carried out with the removal of the skin only, without the subcutaneous tissue and fat pads. After conducting local hemostasis, 6-0 nylon monofilament thread was used to carry out the primary running suture, with the stitches being removed five days after the procedure. As the patient presented only a small amount of excess skin, it was possible to carry out the procedure without the need for rotation flaps or grafting. There was no functional compromise, only residual hypochromia, which did not prevent the patient classification of the procedure as yielding excellent results. There was a high level of patient satisfaction, with reports of improvement in self-esteem and social inclusion.
1. Rohrich RJ, Janis JE, Pownell PH. Xanthelasma palpebrarum: a review and current management principles. Plast Reconstr Surg 2002; 110(5): 1310-14.
2. Bergman R. The pathogenesis and clinical significance of xanthelasma palpebrarum. J Am Acad Dermatol. 1994; 30(2 pt 1):236-42.
3. Then SY, Malhotra R. Superiorly hinged blepharoplasty flap for reconstruction of medial upper eyelid defects following excision of xanthelasma palpebrum. Clin Exp Ophthalmol. 2008;36(5):410-14.
4. Pereira FJ, Cruz AAV, Guimarães Neto HP, Ludvig CC. Blefaroplastia associada a enxertia de pele autóloga para xantelasmas extensos: relato de caso. Arq Bras Oftalmol. 2008;71(4):592-4.
5. Cannon PS, Ajit R, Leatherbarrow B. Efficacy of trichloroacetic acid (95%) in the management of xanthelasma palpebrarum. Clin Exp Dermatol. 2010;35(8):845-8.
6. Dincer D, Koc E, Erbil AH, Kose O. Effectiveness of low-voltage radiofrequency in the treatment of xanthelasma palpebrarum: a pilot study of 15 cases. Dermatol Surg. 2010;36(12):1973-8.
7. Park EJ, Youn SH, Cho EB, Lee GS, Hann SK, Kim KH, Kim KJ. Xanthelasma palpebrarum treatment with a 1,450-nm-diode laser. Dermatol Surg. 2011;37(6):791-6
8. Dewan SP, Kaur A, Gupta RK. Effectiveness of cryosurgery in xanthelasma palpebrarum. Indian J Dermatol Venereol Leprol 1995;61(1):4-7.
9. Pereira JE. Blefaroplastia e procedimentos auxiliares. In: Gadelha AR, Costa IMC. Cirurgia dermatológica em consultório. 2a ed. São Paulo, Rio de Janeiro, Belo Horizonte: Editora Atheneu, 2009. p. 821-42.
10. Fagien S. Blefaroplastia superior: aumento de volume pela abordagem cutânea: rebaixamento do sulco palpebral superior. In: Fagien S. Cirurgia Oculoplástica ESTÉTICA de Putterman. 4a ed. Rio de Janeiro: DiLivros, 2009. p. 85-101.
This study was carried out at the Dermatology Service of the Hospital Naval Marcílio Dias (HNMD), Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}