


Natalia Cymrot Cymbalista1; Renato Garcia2; Samir Jacob Bechara3
Introduction: The aging process in the infraorbital region involves a loss of volume, gravitational and skin changes.
Objective: To describe the etiopathogenic classification and treatment of dark circles caused by lower eyelid contour changes.
Methods: A new technique of hyaluronic acid filling, using a blunt cannula through a unique orifice is presented.
Results: Reformulating the dark circles classification is useful for making the best therapeutic options. The technique's advantages are its safety and good aesthetic results.
Conclusion: Filling with hyaluronic acid using this new technique has proven safer than other pre-existing techniques.
Keywords: EYELIDS; REJUVENATION; HYALURONIC ACID/ADMINISTRATION & DOSAGE.
The aging process in the area around the eyes involves a loss of volume and skin changes that cause aesthetic problems. The literature proposes the following etiopathogenic classification of infraorbital dark circles:
1. Hyperpigmentation of the eyelid, subdivided into:
a) Idiopathic primary cutaneous hyperchromia: a congenital, idiopathic condition resulting from the deposition of melanin in the epidermis and dermis, predominantly in dark-eyed, dark-haired adult females,1 with autosomal dominant inheritance and variable penetrance.2
b) Hyperchromia secondary to post-inflammatory hyperpigmentation, caused by atopic dermatitis,3 allergic contact dermatitis,4 or excessive friction.5
c) Hyperchromia secondary to physiological and pathological conditions that stimulate the deposition of melanin in the skin: exogenous6 or endogenous estrogens and progestins, pregnancy, breastfeeding,3 and systemic diseases such as Addison's disease, pituitary tumors, thyroid disorders, Cushing's syndrome, hemochromatosis (due to increased melanin in the basal layer), and others.
d) Photosensitivity caused by drugs, such as arsenic, phenothiazines, phenytoin, antimalarials, and aromatic hydrocarbons.
e) Increase (250-fold) in the deposition of melanin granules in epidermal melanocytes, and a sixfold increase in dermal melanocytes, caused by the use of local prostaglandin analogues (bimatoprost, lanatoprost) in a 0.03% solution.7 Kohl, a black pigment containing lead that is used around the eyes, especially by Indian women, is also deposited in the dermis and stimulates the deposition of melanin in the epidermis.8
f) Ultraviolet radiation causes skin atrophy, increased blood vessels, and darkens the skin, due to the presence of ephelides or melanoses.
The main differential diagnoses of infraorbital dark circles are acanthosis nigricans,9 periorbital amyloidosis,10 ecchymosis, melasma, Riehl melanosis, lentigines, and nevi (Ota). There is a complete absence of hemosiderin in the pathogenesis of dark circles.11
2. Visible musculature and superficial blood vessels in the lower eyelid: the hypervascular appearance is due to excessive subcutaneous vascularization and hypertransparency of the skin, with little subcutaneous tissue,4 which allows greater visibility of the underlying vessels and the orbicular muscle.12
The vascular factor seems to explain the worsening of dark circles in cases of dehydration, acute illnesses, sleep, systemic diseases, and stress. Due to dehydration, in an area with little subcutaneous tissue, the effect of light on the tissue promotes a bluish shaded color.5
In atopy, allergic rhinitis causes eyelid venous stasis, due to the prolonged edema of the nasal and paranasal mucous membranes, which is aggravated by the allergic spasm of Müller's muscle (superior palpebral muscle), which affects the eyelids' venous drainage.13
3. Lower eyelid contour changes:
a) Eyelid laxity due to photoaging, with skin atrophy due to the loss of collagen and fat.4,14
b) Bone configuration of the orbit, with formation of deeper palpebromalar and nasojugal folds, which produce a shadow on the lower eyelid.
c) Lower eyelid bag, caused by orbital septum laxity and retro-septal fat bulging, forming a fold under the bag.3 This is the most common causal factor of dark circles due to the natural aging of the periorbital region.
Treatment of Infraorbital Dark Circles
Treatment should be based on the subtype. When dark circles are caused by melanin deposition, the following treatments are recommended: chemical peels (phenol, TCA), retinoic acid, topical bleaching products (hydroquinone, kojic acid),1 intense pulsed light11 and lasers that target melanin (Q-Switched Ruby - 694 nm,4,14 Alexandrite -755 nm,15 Nd:Yag -1064 nm),14,15 ablative and non-ablative (CO2 -10,600 nm and Erbium -1540, 1550, 2940 nm), and fractional16,17 and non fractional lasers.18
For dark circles predominantly caused by hypervisibility of the musculature and vasculature, no treatment is recommended, because the cosmetic benefit is minimal.
In cases of contour changes due to eyelid skin laxity, chemical peels (phenol, TCA), intense pulsed light, non-ablative and ablative, non-fractioned and fractioned lasers may be used.
When contour changes are due to alterations in orbital volume, transconjunctival blepharoplasty19 and filling techniques can be employed. Filling is useful when the orbital septum laxity forms a fat bag, with a corresponding deepening of the nasojugal and palpebromalar folds, or when the orbital bone configuration predisposes the formation of deep nasojugal and palpebromalar folds, causing shadows to appear.
Anatomy of the Periorbicular Region
The lower eyelid structure has a free upper margin comprised of anterior, middle, and posterior lamellae layers. The anterior lamella consists of skin and the orbicularis muscle (divided into orbital and palpebral portions). The middle lamella is composed of the orbital septum, orbital fat, and the sub-orbicular fibrotic fatty tissue. The orbital septum is an inelastic fibrous tissue that separates the orbital contents (orbital fat) from the external (pre-septal) contents, acting as a diaphragm. The weakening of this structure leads to post-septal fat prolapse, causing a pseudo-herniation. The sub-orbicularis oculi fat (SOOF)is located below the orbital portion of the orbicularis muscle and anterior to the orbital septum. The SOOF clings to the arcus marginalis of the inferior orbital rim. During youth, the more superior position of the SOOF allows the orbicularis muscle to override it.20-22 The posterior lamella is composed of the tarsus, conjunctiva, and retractor muscles.22
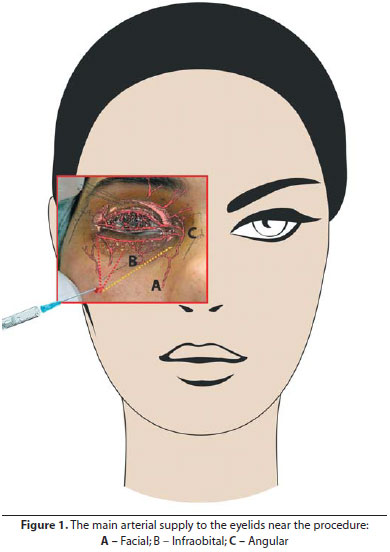
The main arterial supply to the eyelids comes from the distal branches of the internal (lacrimal, supraorbital, ophthalmic, nasal, and frontal arteries) and external carotid system, which contributes to the vascularization of the mid-face and lower eyelids (superficial temporal, infra-orbital, and angle arteries). The angle artery is located on the nasal dorsum, in the region of the lacrimal sac. In the lower lid, there is a poor network of anastomoses, which forms the marginal arcade. Laterally, there are lacrimal artery anastomoses (internal carotid system) with the zygomaticofacial artery, a branch of the superficial temporal artery (external carotid system)22 (Figure 1).
The central retinal artery is a proximal ramification of the ophthalmic artery. The filler penetration and retrograde and anterograde movements within vessels, including the internal carotid and ophthalmic arteries and their ramification, could cause the occlusion of the central retinal artery.
Pathophysiology of the Aging Process of the Lower Periorbital Region
The nasojugal fold becomes more prominent over time because it has little subcutaneous fat. This concave deformity consists of thin skin attached to the orbicularis muscle near its insertion in the orbital rim. The accentuation of this concavity is often associated with the herniation of lower eyelid fat pockets and ptosis of the SOOF.
The pseudo-herniation of orbital fat due to the weakening of the orbital septum, associated with hypotrophy of the orbicularis muscle and SOOF ptosis, leads to the skeletonization process of the inferior orbital rim. The orbital-malar and zigomatic-cutaneous retaining ligaments adhered to the inferior orbital rim and the skin support the orbicularis muscle and orbital fat pockets. Thus, there is a separation between the periocular and mid-face regions, deepening the nasojugal and palpebromalar folds, respectively, which creates a double appearance of convexity22-24 (Figure 2).
This study focuses on the etiopathogenic classification and treatment of dark circles caused by lower eyelid contour changes. A new technique of hyaluronic acid (HA) application is presented that uses a blunt cannula, emphasizing anatomical sites of application, safety, and aesthetic results.
Fillers Previously Used in the Lower Eyelid Calcium Hydroxyapatite
Radiesse®, calcium hydroxyapatite spheres in a sodium carboxymethylcellulose gel (Bioform Medical Inc, Fransville, WI, USA), can be injected25 by a single supraperiostal puncture at the inferior orbital rim, or jaw, followed by molding to adjacent regions. It presents a high risk of complication26 and does not always provide regular contour. Reinjection might be difficult because the tissue becomes hardened.
Autologous Fat
Filling with autologous fat is laborious, and is done under local anesthesia and intravenous sedation. Donor areas are the abdomen and the medial and lateral regions of the thigh. The application is supraperiostal or subcutaneous, using a cannula. Approximately 3 ml of fat are used in each periorbital area (maximum 6 ml). The injected volume stabilizes at around 12 weeks.
Complications include contour alterations27 (excessive volume injected, or too superficial an injection), persistent malar edema, overcorrection, infection, cerebral and ocular arterial embolism,28 neural injury,24 and periorbital lipogranulomas.29
Hyaluronic Acid
Filling techniques for the nasojugal and palpebromalar folds are diverse and use needles or cannulas. Most articles describe techniques using needles, with topical anesthesia (25 mg lidocaine, 25 mg prilocaine,) or an infraorbital nerve block.4,25,30-34 In one of the techniques described, the authors used a 30 G or 31 G needle to puncture 3-8 sites on each side of the eyelid (on the edge of the orbital rim). The needle went through the supraperiostal region and HA was injected in a retrograde fashion, in small quantities, after preventive aspiration. Approximately 0.1 ml was injected on each side.
One study describes a technique using 25-50 punctures,32 while another describes punctures in the lateral to nasal regions.34 During and after the injections, massages are performed, to correctly mold the HA.4,25,31-34
In another technique described, HA was injected with a 30 G cannula through a 25 G needle hole punctured in the nasojugal fold.30 Small volumes (0.01-0.05 cc) were injected in a retrograde manner. The injection was intraorbicular, superficial to the periosteum of the orbital rim, and discontinuous (medial to lateral) in small quantities. To avoid injecting a large volume in a single pathway, more entry points were used: two or three in the central and medial regions, and one or two in the lateral region.
Description of Hyaluronic Acid
Non-animal stabilized hyaluronic acid (NASHA) is produced from the fermentation of strands of Streptococcus. The product is stabilized by a series of cross-linkings. It is biocompatible, easy to store, and non-immunogenic. The use of Restylane®, Perlane®, Sub-Q (Q-MED AB, Uppsalla, Sweden), Juvederm®, Juvederm Voluma (Allergan, Irvine, CA), Hylaform® (Genzyme Corporation, Ridgefield, NJ, USA), and Teosyal global® (Teoxane, Geneva, Switzerland) for the pre-orbital area filling has already been described in literature.
Application Technique
After local asepsis (chlorexidine gluconate 2-4%), the patient is reclined at 30 degrees from the vertical position and is asked to look up, to make the nasojugal and palpebromalar folds most visible. Sterile gloves and gauze are used and a blunt cannula (26-27 G/ 35-37 mm) is introduced through a skin orifice with a 22 G needle, through the entire skin thickness.
A "curtain maneuver"31 may be necessary as the cannula is introduced, pressing the skin to the front of the cannula to make sure the administration is not too shallow. The cannula is introduced perpendicularly to the skin and directed to the nasojugal fold in the intramuscular area. It easily slides through the medial region after going through the orbicular muscle, with minimal pressure. The tip can be viewed through its depression, following it through the upper portion of the nasojugal fold up to the lacrimal points. In a second movement, it can be directed at a laterosuperior angle up to the more lateral portions of the malar fold.
A slow, discontinuous retroinjection of the product is made at the supraperiostal level (0.5-1 m per eyelid). Then the filler is molded with the fingers' pressure. To minimize the risk of vascular embolism, the procedure must be interrupted if bruises appear.
Corrective procedures with HA must use a 1:1 ratio; that is, the quantity of filler injected that can be viewed promotes a volume increase that should be kept after the end of the edema caused by HA injection. Caution must be used during injection in the medial area of the nasojugal fold in order to avoid the angular vein. It mustbe lateral to the lacrimal point, for medial filling at this point can lead to artificial results. It is necessary to act relatively quickly, so that the edema caused by the injection does not distort the area's anatomy.
Recommendations to be followed after the procedure include placing ice on the area while the patient is lying down and elevated. Local massaging should be avoided until the resolution of the edema (on average, 7-10 days). If bruises develop, tinted solar protection agents or corrective make-up are recommended for 24 hours after the procedure to avoid skin hyperpigmentation.
Procedures with botulinum toxin in the same region must be avoided for 10 days, so that the edema caused by the filling does not cause an infero-medial displacement of the toxin.
Possible Complications
1. Diffused malar edema, which may last up to three weeks or be persistent and resistant to hyaluronidase. HA should not be used in patients with a tendency to retain fluid in the orbital area. Treatment is made using oral prednisone, 0.5 mg/kg for 1 to 3 days after the procedure. More persistent cases may need a local injection of hyaluronidase, 5-20 units per point of injection (Hyalozima® 200 U/ml), totaling to 25-50 units per side. Improvements in contour irregularities or edema begin to show24 hours after treatment.35
2. Ecchymosis. This type of complication is rare with cannulas and lasts, on average, 7-10 days. The placement of ice and compression immediately after the procedure, and the avoidance of prior use of anti-platelet agents and anticoagulants, minimize the occurrence of ecchymosis.
3. Contour changes. One of the most common complications; such changes are more likely to occur in patients with thin and flaccid skin. Superficial application of HA, as well as its use in bigger particles, must be avoided. The risk decreases with deeper injections (supraperiostal area). Massage can resolve surface irregularities related to deep injections, while those caused by more superficial injections may require hyaluronidase.
4. Erythema.
5. Granulomas.29
6. Hypersensitivity reaction – 0.02%.
7. Color changes (5% of cases): bluish or grayish coloration due to superficial injection, or sometimes with deeper injections as well. The filler becomes visible, causing a light refraction effect known as Tyndall.
8. Cellulitis – 0.7%.31,34
9. Headache – 0.3%.31
Most adverse effects are self-limited and resolve spontaneously. There are no reports in the literature of amaurosis with HA injected in the face.36,37
This technique differs from the ones already studied, since we used only one entry into the skin for injection with a blunt cannula. The puncture is located temporally and inferiorly to the infraorbital foramen, which provides both ease of access to the nasojugal and palpebro-malar folds and safety against vascular accidents when opening the entry into the skin. Using this technique, the cannula goes through the intramuscular plane, passing superiorly and superficially to the components of the infraorbital foramen.
Blepharoplasty to remove fat tissue, whether removing skin or not, does not treat the cause of the problem. Combined treatments that include removing fat pouches, orbital septum strengthening under the Lockwood ligament, and insertion of filling substances (such as HA) in the nasojugal and orbital-malar folds have better results than exclusively surgical methods. In many cases, treatment with HA only is sufficient to meet the patient's aesthetic needs.
Theoretically, HA is reabsorbed within about one year. However, we have verified through clinical observation that a partial volumetric effect lasts longer than this. The mechanism through which HA promotes filling involves the attraction of water molecules to the extracellular matrix of its injection point. In addition, it improves dermis elasticity as it stimulates neocollagenesis. NASHA significantly increases the production of type-1 procollagen and the gene expression of types 1 and 2 procollagen, as well as profibrotic growth factors during weeks 4 and 13 after HA injection.38
In addition to being biocompatible, easy to store, and nonimmunogenic, HA offers a strong benefit over all other skin fillers: it can be dissolved with hyaluronidase. This allows the correction of excessive injections and the total removal of the product in case of any chronic reactions.
The palpebromalar fold must be filled in to promote a "lifting" effect and allow the injection of lesser quantities of the filler into the nasojugal fold, as well as restore the convex shape of the cheeks.
The superficiality of the injection is inversely proportional to the quantity of filler needed to attain the same volumetric effect. The combination of a deep (supraperiostal) injection and a more superficial one, at the plane between the deep dermis and the orbicularis muscle, can be used. Filling the medial-malar area (a central and triangular depression) may help achieve a more uniform face volume and correct malar pouches.
The satisfaction level after initial treatment reaches 80% and the treatment effect duration reaches two years in some cases. Recurrence may occur due to product absorption, associated with the natural continued aging of the area. It is difficult to determine how much each of these factors contributes to recurrence.
Advantages of the New Technique
1. It is safer than using needles, helping to eliminate the risk of accidental intravascular injection. Hematomas represent a risk of embolism, loss of volumetric parameters for filling, and a possible decrease in the duration of the filler effect. Although we have not found cases of amaurosis by HA injection in the face in the literature, unreported cases are a possibility.
Some reports of vascular embolism causing strokes, amaurosis, and cutaneous necrosis related to the injection of autologous fat, silicon,collagen, polymethylmetacrilate, Cymetra (LifeCell Corp., Branchbrug, NJ, USA), and corticosteroids can be found in the literature.39-48
2. The technique does not require the use of local anaesthesia, which lowers the risk of skin or ocular reactions.
3. Pain is minimal.
4. The technique uses only one entry orifice.
5. The satisfaction level is very high, due to the aesthetic results and the ability to immediately resume normal activities.
The reformulation of the ranking system for dark circles is useful for choosing the best therapeutic modality. We also conclude that filling with HA in the inferior orbital area using this new technique with a blunt-tipped cannula has proved safe, effective, and beneficial in our practice compared to other techniques.
1. Aqulera Díaz L. [Pathology and genetics of bipalperbral hyperpigmentation]. Actas Dermosifiliogr. 1971;62(9):397-410.
2. Hunzinker N. A propos de l´hyperpigmentation familiale dés paupières. J Génét Hum. 1962;11:6-21.
3. Epstein JS. Management of infraorbital dark circles. A significant cosmetic concern. Arch Facial Plast Surg. 1999;1(4):303-7.
4. Lowe NJ, Wieder JM, Shorr N, Boxrud C, Saucen D, Chalet M. Infraorbital pigmented skin. Preliminary observations of laser therapy. Dermatol Surg. 1995;21(9):767-70.
5. Winkelmann RK. Dark circles under the eyes. JAMA. 1965;93:61.
6. Garcia A, Fulton JE Jr. The combination of glycolic acid and hydroquinone or kojic acid for the treatment of melasma and related conditions. Dermatol Surg. 1996;22(5):443-7.
7. Priluck JC, Fu S. Latisse-induced periocular skin hyperpigmentation. Arch Ophthalmol. 2010;128(6):792-3.
8. El Safoury OS, El Fatah DS, Ibrahim M. Treatment of periocular hyperpigmentation due to lead of kohl (surma) by penicillamine: a single group non-randomized clinical trial. Indian J Dermatol. 2009;54(4):361-3.
9. Ing EB, Buncic JR, Weiser BA, de Nanassy JD, Boxall L. Periorbital hyperpigmentation and erythema dyschromicum perstans. Can J Ophthalmol. 1992;27(7):353-5.
10. van den Berg WH, Starink TM. Macular amyloidosis, presenting as periocular hyperpigmentation. Clin Exp Dermatol. 1983;8(2):195-7.
11. Cymbalista NC, Prado de Oliveira ZN. Treatment of idiopathic cutaneous hyperchromia of the orbital region (ICHOR) with intense pulsed light. Dermatol Surg. 2006;32(6):773-83; discussion 783-4.
12. Elson ML. Evaluation and treatment of the aging face. New York: Springer-Verlag; 1995.
13. Marks MB. Allergic shiners. Dark circles under the eyes in children. Clin Pediatr (Phila). 1966;5(11):655-8.
14. Boxrud C, Shorr N, Steisapir K. Management of dark circles around the eyes. In: American Society of Ophthalmologic Plastic and Reconstructive Surgeons. Chicago; 1993. [abstracts].
15. Rosenbach A, Williams CM, Alster TS. Comparison of the Q-switched alexandrite (755 nm) and Q-switched Nd: YAG (1064 nm) lasers in the treatment of benign melanocytic nevi. Dermatol Surg. 1997;23(4):239-44; discussion 244-5.
16. Tierney EP, Hanke CW, Watkins L. Treatment of lower eyelid rhytids and laxity with ablative fractionated carbon-dioxide laser resurfacing: Case series and review of the literature. J Am Acad Dermatol. 2011;64(4):730-40.
17. Sukal SA, Chapas AM, Bernstein LJ, Hale EK, Kim KH, Geronemus RG. Eyelid tightening and improved eyelid aperture through nonablative fractional resurfacing. Dermatol Surg. 2008;34(11):1454-8.
18. Lupton JR, Alster TS. Evaluation of one-pass CO2 laser resurfacing for infraorbital hyperpigmentation. Lasers Surg Med. 2002;14:21.
19. Zarem HA, Resnick JI. Expanded applications for transconjuntival lower lid blepharoplasty. Plast Reconstr Surg. 1991;88(2):215-20; discussion 221.
20. Rohrich RJ, Arbique GM, Wong C, Brown S, Pessa JE. The anatomy of suborbicularis fat: implications for periorbital rejuvenation. Plast Reconstr Surg. 2009;124(3):946-51.
21. Kakizaki H, Malhotra R, Madge SN, Selva D. Lower eyelid anatomy: an update. Ann Plast Surg. 2009;63(3):344-51.
22. Burkat CN, Lemke BN. Anatomy of the orbit and its related structures. Otolaryngol Clin North Am. 2005;38(5):825-56.
23. Glasgold M, Lam SM, Glasgold R. Volumetric rejuvenation of the periorbital region. Facial Plast Surg. 2010;26(3):252-9.
24. Haddock NT, Saadeh PB, Boutros S, Thorne CH. The tear trough and lid/cheek junction: anatomy and implications for surgical correction. Plast Reconstr Surg. 2009;123(4):1332-40; discussion 1341-2.
25. Buckingham ED, Bader B, Smith SP. Autologous fat and fillers in periocular rejuvenation. Facial Plast Surg Clin North Am. 2010;18(3):385-98.
26. Hirman H. Anatomy and nonsurgical correction of the tear trough deformity. Plast Reconstr Surg. 2010;125(2):699-708.
27. Roh MR, Chung KY. Infraorbital dark circles: definition, causes, and treatment options. Dermatol Surg. 2009;35(8):1163-71.
28. Thaunat O, Thaler F, Loirat P, Decroix JP, Boulin A. Cerebral fat embolism induced by facial fat injection. Plast Reconstr Surg. 2004;113(7):2235-6.
29. Sa HS, Woo KI, Suh YL, Kim YD. Periorbital lipogranuloma: a previously unknown complication of autologous fat injections for facial augmentation. Br J Ophthalmol. 2011;95(9):1259-63.
30. Hirmand H. Anatomy and nonsurgical correction of the tear trough deformity. Plast Reconstr Surg. 2010;125(2):699-708.
31. Steinsapir KD, Steinsapir SM. Deep-fill hyaluronic acid for the temporary treatment of the naso-jugal groove: a report of 303 consecutive treatments. Ophthal Plast Reconstr Surg. 2006;22(5):344-8.
32. Goldberg RA, Fiaschetti D. Filling the periorbital hollows with hyaluronic acid gel: initial experience with 244 injections. Ophthal Plast Reconstr Surg. 2006;22(5):335-41; discussion 341-3.
33. Kane MA. Treatment of tear trough deformity and lower lid bowing with injectable hyaluronic acid. Aesthetic Plast Surg. 2005;29(5):363-7.
34. VIiana GAP, Osaki MH, Cariello AJ, Damasceno RW. Tratamento dos sulcos palpebromalar e nasojugal com ácido hialurônico [Treatment of tear trough deformity with hyaluronic acid gel filler]. Arq Bras Oftalmol. 2011;74(1):44-7.
35. Vartanian AJ, Frankel AS, Rubin MG. Injected hyaluronidase reduces restylane-mediated cutaneous augmentation. Arch Facial Plast Surg. 2005;7(4):231-7.
36. Bellman B. Complication following suspected intra-arterial injection of Restylane. Aesthet Surg J. 2006;26(3):304-5.
37. Lowe NJ. Arterial embolization caused by injection of hyaluronic acid (Restylane). Br J Dermatol. 2003;148(2):379; author reply 379-80.
38. Wang F, Garza LA, Kang S, Varani J, Orringer JS, Fisher GJ, Voorhees JJ. In vivo stimulation of de novo collagen production caused by cross-linked hyaluronic acid dermal filler injections in photodamaged human skin. Arch Dermatol. 2007;143(2):155-63.
39. Danesh-Meyer HV, Savino PJ, Sergott RC. Case reports and small series: ocular and cerebral ischemia following facial injection of autologous fat. Arch Ophthalmol. 2001;119(5):777-8.
40. Shin H, Lemke BN, Stevens TS, Lim MJ. Posterior ciliary-artery occlusion after subcutaneous silicone-oil injection. Ann Ophthalmol. 1988;20(9):342-4.
41. Shafir R, Cohen M, Gur E. Blindness as a complication of subcutaneous nasal steroid injection. Plast Reconstr Surg. 1999;104(4):1180-2; discussion 1183-4.
42. Rohrich RJ, Ghavami A, Crosby MA. The role of hyaluronic acid fillers (Restylane) in facial cosmetic surgery: review and technical considerations. Plast Reconstr Surg. 2007;120(6 suppl):41S-54S.
43. Dreizen NG, Framm L. Sudden unilateral visual loss after autologous fat injection into the glabellar area. Am J Ophthalmol. 1989;107(1):85-7.
44. Lemperle J, Romano JJ, Busso M. Soft tissue augmentation with artecoll: 10-year history, indications, techniques, and complications. Dermatol Surg. 2003;29(6):573-87; discussion 587.
45. Silva MT, Curi AL. Blindness and total ophthalmoplegia after aesthetic polymethylmethacrylate injection: case report. Arq Neuropsiquiatr. 2004;62(3B):873-4.
46. Coleman SR. Avoidance of arterial occlusion from injection of soft tissue fillers. Aesthet Surg J. 2002;22(6):555-7.
47. Schanz S, Schippert W, Ulmer A, Rassner G, Fierlbeck G. Arterial embolization caused by injection of hyaluronic acid (Restylane). Br J Dermatol. 2002;146(5):928-9.
48. Apte RS, Solomon SD, Gehlbach P. Acute choroidal infaction following subcutaneous injection of micronized dermal matrix in the forehead region. Retina. 2003;23(4):552-4.
This study was carried out at the Faculdade de Medicina da Universidade de São Paulo (FMUSP) – São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}