


Célia Luiza Petersen Vitello Kalil1; Matheus Silva Melo1; Giulia Dambrós Malacarne1; Isabela de Liz Pereira1
Funding source: None
Conflict of interest: None
Submitted on: 10/22/2025
Final decision: 12/19/2025
How to cite this article: Kalil CLPV, Melo MS, Malacarne GD, Pereira IL. Rosacea: pathophysiology and therapeutics. Surg Cosmet Dermatol. 2026;18:e20260526.
Rosacea is a chronic, multifactorial inflammatory dermatosis involving immune dysregulation, neurovascular alterations, and microbial imbalance. Overexpression of TLR2, activation of TRP channels, and increased LL-37 cathelicidin are central to its pathophysiology. Therapeutic management includes behavioral strategies, topical treatments (metronidazole, ivermectin, azelaic acid, brimonidine), systemic agents (doxycycline, isotretinoin), and procedures such as laser and intense pulsed light. A personalized, multifaceted approach combining trigger control, pharmacologic therapy, and physical interventions is crucial for reducing symptoms and improving patient quality of life.
Keywords: Rosacea; Innate immunity; Cathelicidins; Botulinum toxin type A; Tetracyclines; Technology
Rosacea is a common chronic inflammatory dermatosis that preferentially affects the centrofacial region, characterized by persistent or episodic erythema, telangiectasias, papules, and pustules. It may also present with phymatous and ocular manifestations. Its epidemiology shows considerable variability: global prevalence is estimated to range between 2% and 10% of the adult population, but higher rates, of up to 18%, have been reported in Northern European populations, where lighter skin phototypes (I–II) predominate.1,2 In Asian and Latin American countries, reported prevalence is lower, although cultural factors, lower physician familiarity with the disease, and atypical clinical presentations are known to contribute to underdiagnosis.3
Rosacea typically manifests between the fourth and sixth decades of life, although cases in young adults are not rare. It affects both sexes but shows striking differences in presentation: the erythematotelangiectatic and papulopustular forms occur more frequently in women, whereas the phymatous form is more prevalent in men, particularly at older ages. Involvement in children is rare, with ocular disease being the primary manifestation, frequently underestimated or mistaken for recurrent conjunctivitis.4 Known predisposing factors include light skin phototype, positive family history, and cumulative sun exposure, as well as environmental triggers such as extreme temperatures, alcohol consumption, spicy foods, and emotional stress, all associated with the vascular hyperreactivity characteristic of the disease.5,6
From a clinical standpoint, rosacea is notoriously heterogeneous. In addition to persistent centrofacial erythema and episodes of flushing, often exacerbated by environmental stimuli, visible telangiectasias are common, as are inflammatory flares of papules and pustules, without the presence of comedones, which helps differentiate rosacea from acne vulgaris. Up to 90% of patients report subjective symptoms such as stinging and burning sensation of the skin, pruritus, and skin hypersensitivity, which explains the frequent perception of "sensitive skin."3,6
The clinical spectrum also includes less common variants, such as granulomatous rosacea, characterized by firm, monomorphic erythematous or yellowish papules, and persistent solid edema (lymphedematous rosacea), which is difficult to manage and associated with chronic facial lymphedema.3,4 Ocular involvement occurs in up to 50% of cases and ranges from mild blepharitis to more severe complications such as keratitis, episcleritis, and uveitis, with a potential risk of visual loss if not diagnosed and treated promptly.6,7 The most common symptoms include foreign-body sensation, pruritus, photophobia, and conjunctival hyperemia. The lack of correlation between cutaneous and ocular severity makes active screening for these manifestations essential.6
The clinical significance of rosacea transcends its cutaneous and ocular manifestations. Several studies have documented its psychosocial impact, with frequent reports of social stigmatization, low self-esteem, and impaired interpersonal interactions. In quality-of-life assessments, patients with rosacea score comparably to those with chronic diseases such as psoriasis and atopic dermatitis.2,3 In addition, increasing evidence suggests an association between rosacea and systemic comorbidities, including gastrointestinal disorders (Helicobacter pylori infection, irritable bowel syndrome, and inflammatory bowel disease), neurological conditions (migraine and Parkinson's disease), and psychiatric disorders (anxiety and depression), suggesting that the disease may reflect a systemic inflammatory state.3,4
Historically classified into 4 clinical subtypes (erythematotelangiectatic, papulopustular, phymatous, and ocular), this categorization has run into limitations in clinical practice due to frequent overlap of findings. In 2017, the international ROSCO panel (Rosacea Consensus) proposed a phenotype approach based on primary (persistent erythema, papules/pustules, telangiectasias, phymatous changes, and ocular signs) and secondary features (flushing, stinging, burning, edema, and extracutaneous manifestations). This approach improves diagnostic accuracy and facilitates the development of individualized therapeutic strategies.3,6
Regarding therapeutic management, rosacea encompasses a spectrum of options ranging from general measures, such as identification and avoidance of triggers, strict photoprotection, and skin barrier care, to pharmacological interventions and specific procedures. Topical treatments include brimonidine and oxymetazoline (vasoconstrictors for erythema), metronidazole, ivermectin, and azelaic acid (anti-inflammatory and antiparasitic agents). Low-dose oral antibiotics (such as subantimicrobial doxycycline), isotretinoin in refractory cases, and more recently investigations involving immunomodulatory agents stand out among systemic therapies. Physical modalities such as laser therapy and intense pulsed light (IPL) play an important role, particularly in controlling telangiectasias and persistent erythema. Treatment should be guided not only by the predominant phenotype but also by symptom severity and the impact on the patient's quality of life.5,6
Given its high prevalence, diversity of clinical manifestations, psychosocial impact, and potential association with comorbidities, rosacea represents a frequent and relevant challenge in dermatological practice. Therefore, this study aimed to review the therapeutic approach to erythematotelangiectatic and papulopustular rosacea in light of the most recent evidence, without addressing in detail the phymatous and ocular forms, which fall outside the scope of this study.
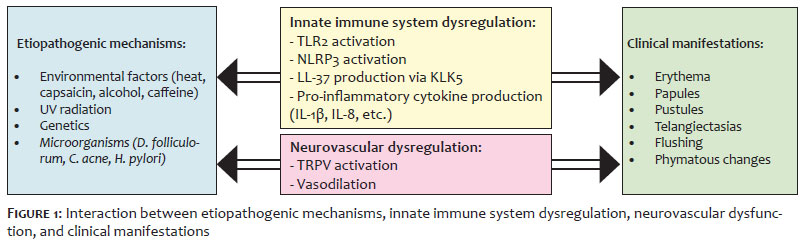
The pathophysiology of rosacea is multifactorial and complex, resulting from the dynamic interaction between genetic predisposition, immune dysfunction, neurovascular alterations, skin dysbiosis, and environmental factors. Although it is not yet fully understood, this network of mechanisms contributes to the development and perpetuation of the chronic skin inflammation characteristic of the disease.7 To facilitate understanding of this process, the main pathophysiological elements can be divided into the following topics:
exacerbated innate immune response and production of pro-inflammatory cathelicidin;
neurovascular dysfunction and hypersensitivity to stimuli; and
various etiopathogenic mechanisms, particularly the role of microorganisms (Figure 1).
Each of these mechanisms will be discussed below in light of current evidence, with the aim of integrating pathophysiological findings with clinical practice and therapeutic management of rosacea.
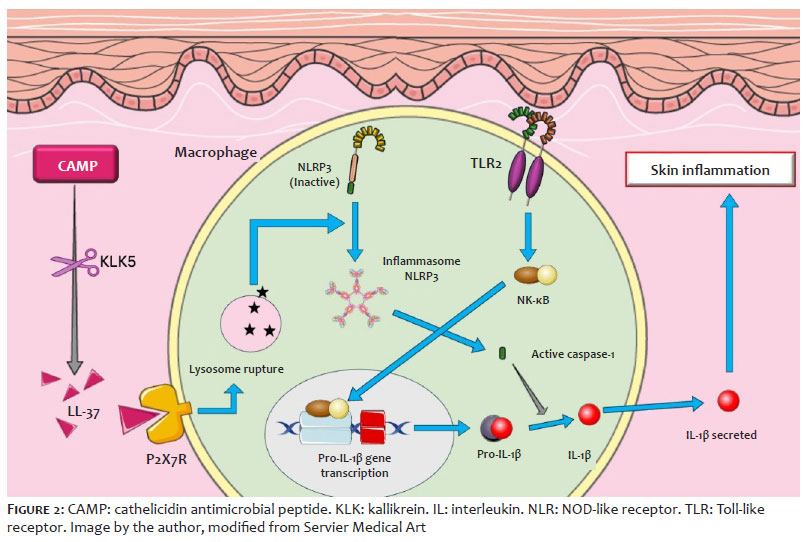
Although its pathogenesis is not fully understood, the role of innate immunity as a central factor in the initiation and perpetuation of skin inflammation is increasingly recognized. This means that receptors such as Toll-like receptors (TLRs) and NOD-like receptors (NLRs) have emerged as key elements in the activation of inflammatory pathways in the skin.7 Understanding the mechanisms involving these receptors helps clarify the molecular processes underlying the clinical manifestations of the disease (Figure 2).
TLRs constitute a class of transmembrane proteins expressed mainly in cells of the innate immune system, such as keratinocytes, macrophages, and dendritic cells. They act as molecular sensors capable of recognizing pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs), triggering pro-inflammatory signaling cascades. These receptors may be found both in the plasma membrane (such as TLR2 and TLR4), where they recognize bacterial surface components, or in endosomal compartments (such as TLR7 and TLR9), where they detect viral and bacterial nucleic acids.7,8
At least 10 functional TLRs have been identified in humans (TLR1 to TLR10), each with specificity for different classes of ligands. For example, TLR2 recognizes lipoproteins and peptidoglycans from gram-positive bacteria, TLR4 recognizes lipopolysaccharides (LPS) from gram-negative bacteria, and TLR7 and TLR9 recognize viral nucleic acids.7,8
In rosacea, there is particularly noteworthy overexpression of TLR2 in the epidermis, sebaceous glands, and adnexal structures. This increase lowers the threshold for skin immune activation, making it hyperresponsive to normally innocuous stimuli, such as temperature changes, topical products, or even the resident microbiota.5,8
NLRs, in turn, are intracellular receptors. Unlike TLRs, which detect threats in extracellular space or endosomal compartments, NLRs recognize microbial components and signs of cellular stress. Activation of NOD receptors leads to signaling through pathways such as nuclear factor kappa B (NF-κB), resulting in the production of pro-inflammatory cytokines such as interleukin (IL)-1β, IL-6, and tumor necrosis factor-α (TNF-α). In addition, NLRs participate in the formation of inflammasomes, intracellular protein complexes that activate caspase-1 and promote the release of IL-1β, a cytokine widely associated with inflammatory lesions in rosacea.7,8
Both TLR2 overexpression and exacerbated activation of the NOD2 intracellular receptor contribute to the amplification of the inflammatory response in rosacea through increased production of cathelicidins, a family of small antimicrobial peptides present in humans and animals that play an important role in the innate immune system.9 A particularly noteworthy member of this group is LL-37, which is generated through cleavage of cathelicidin antimicrobial peptide (CAMP), its inactive precursor. This cleavage is performed by the enzyme kallikrein 5 (KLK5), whose expression is also stimulated by TLR2.5,8,10 KLK5 is a serine protease that plays an important role in the skin, more specifically in the stratum corneum of the epidermis. Encoded by the KLK5 gene, it is involved in the regulation of skin desquamation and may also contribute to skin inflammation because it can cleave protease-activated receptors (PARs) in keratinocytes, leading to the release of inflammatory cytokines.11
Once formed, LL-37 acts on different types of receptors, triggering intracellular signaling cascades (such as activation of NF-κB) that result in the production of inflammatory cytokines (IL-1β, IL-6, and TNF-α), induction of vasodilation, recruitment of immune cells, and vascular remodeling. The abnormal and persistent accumulation of LL-37 in the skin of patients with rosacea therefore not only reflects a dysfunction in the regulation of innate immunity but also represents a point of convergence between different inflammatory pathways involved in the pathogenesis of the disease.10
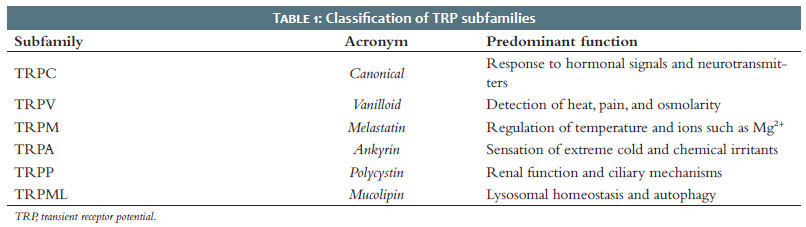
Neurovascular dysregulation constitutes one of the central pillars of rosacea pathophysiology, particularly in clinical forms characterized by persistent erythema, flushing, and telangiectasias. One of the molecular mechanisms that explains this hyperreactivity involves the overexpression and abnormal activation of transient receptor potential (TRP) channels. TRP channels are a superfamily of nonselective ion channels that regulate the influx of cations, especially calcium (Ca2+) and sodium (Na+), in response to various environmental and endogenous stimuli. Present in multiple tissues, including the skin, TRP channels act as molecular sensors that translate thermal, mechanical, chemical, and osmotic stimuli into electrical and biochemical signals. They are particularly abundant in sensory nerve endings, where they contribute to the perception of pain, pruritus, heat, cold, and inflammation.12
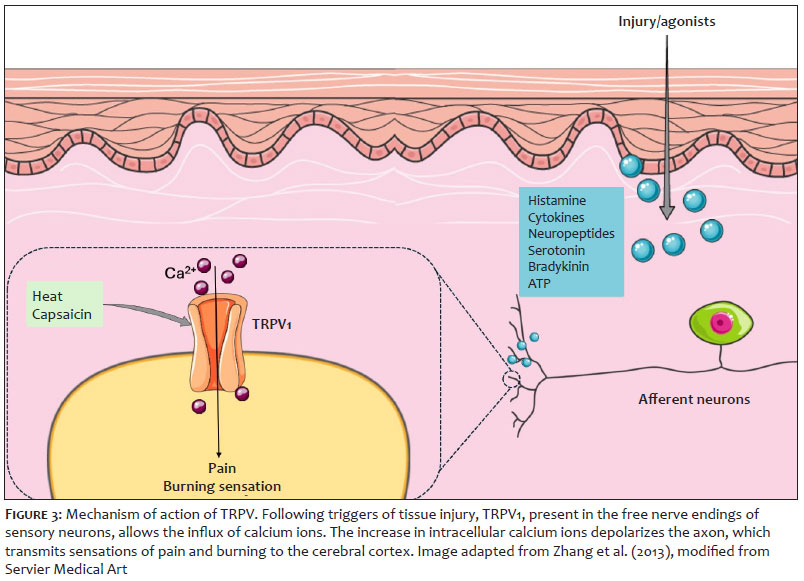
The TRP family is subdivided into 6 main subgroups based on sequence homology and functional characteristics. Table 1 summarizes these proteins. The overexpression and abnormal activation of specific TRP subtypes have been observed in the skin of individuals with rosacea, particularly TRPV1, TRPA1, and TRPV412 (Figure 3).
Among external factors, microorganisms have been implicated as important triggers or modulators of skin inflammation. Although the presence of these organisms is not pathognomonic for the disease, increasing evidence suggests that they play an important role in perpetuating the inflammatory response.7,10,13
The mite Demodex folliculorum is a commensal ectoparasite of human skin with a predilection for the pilosebaceous follicles of the face. Studies have shown a significant increase in Demodex density in patients with rosacea, particularly in papulopustular and granulomatous forms. A high parasite load may disrupt the local immune balance and trigger an exacerbated inflammatory response. It is believed that antigenic products from Demodex, as well as symbiotic microorganisms living within the mite (such as Bacillus oleronius), stimulate overexpression of TLR-2 and promote activation of the LL-37 cathelicidin pathway, favoring neutrophil chemotaxis and the release of metalloproteinases. In addition, follicular degradation caused by the parasite may act as a DAMP, amplifying the immune response.7,8,14
The management of rosacea is based on the adoption of behavioral measures, which include patient education about the disease, identification of triggering factors, and the implementation of specific skin care practices.13
Identification and prevention of aggravating agents, such as sun exposure, temperature variations, psychosocial stress, alcohol consumption, diet, caffeine intake, strenuous exercise, and the use of potentially irritating cosmetics, are essential elements for understanding and individualizing disease management. Evidence indicates that more than 90% of patients are able to associate worsening of the clinical condition with triggering factors, reinforcing the importance of educational strategies aimed at reducing flare-ups.15 In addition, the adoption of personal records, such as diaries, helps identify individual patterns of exacerbation and promotes more effective disease control.15,16
Among aggravating factors, the consumption of alcohol (especially wine and spirits), hot drinks, and foods containing capsaicin and cinnamaldehyde is correlated with worsening of the clinical condition. Exposure to heat and the consumption of foods containing capsaicin may lead to activation of TRPV vanilloid channels, particularly subtypes 1 and 6, which are involved in vasodilation and increased skin sensitivity, thereby contributing to flushing and burning sensations in rosacea.17
Exposure to UV radiation, in turn, induces an innate immune inflammatory response mediated by antimicrobial peptides such as LL-37 and pro-inflammatory cytokines such as IL-33, which promote angiogenesis and vascular hyperreactivity.10
The relationship between smoking and rosacea shows a protective association. In a large population-based analysis conducted in the United Kingdom, a lower risk of rosacea was observed in smokers.18 Furthermore, there was also a significant reduction in the risk of developing rosacea among smokers. However, the nicotine from tobacco has angiogenic effects that may trigger rosacea symptoms and aggravate pustular lesions and rhinophyma. Therefore, given the negative impact of tobacco on overall and skin health, patients with rosacea should be counseled on the importance of smoking cessation despite the paradoxical associations described.17
In addition to the management of aggravating factors, rosacea substantially compromises the integrity of the skin barrier, leading to dehydration, irritability, and increased sensitivity.10 In this context, specific and individualized skin care becomes essential for optimizing therapeutic response. For cleaning, the use of mild, soap-free cleansers with a pH around 5.5 is recommended once or twice daily. In addition to cleaning, moisturization should also be incorporated into the daily skin care routine, as it is essential for restoring barrier function and relieving symptoms such as burning, pruritus, and xerosis. Formulations should be gentle, contain soothing and reparative agents, and be free of potentially irritating or sensitizing substances.19
Complementarily, broad-spectrum photoprotection should be incorporated into rosacea treatment. Daily use of water-based sunscreens with a sun protection factor (SPF) of 30 or higher is recommended, with frequent reapplication. Sunscreens formulated with vehicles containing dimethicone and cyclomethicone are preferable to minimize skin irritation.18,20 In addition, formulations containing physical filters such as zinc oxide and titanium dioxide have good tolerability profiles.20
Beyond these measures, the use of corrective cosmetics to camouflage erythema may be a useful strategy to mitigate the psychosocial impact of the disease. Among available options, mineral makeup is one of the most recommended because of its good tolerability, photoprotective properties, anti-inflammatory effect, and low comedogenic potential.17,20
Brimonidine and oxymetazoline act as topical α-2 and α-1 adrenergic receptor agonists, respectively.7 Topical use of these agents promotes transient vasoconstriction of dermal vessels, with a rapid onset of action, within about 30 minutes. Their effects may last between 3 and 12 hours.10,15
Brimonidine 0.33% gel was approved in 2013 by the U.S. Food and Drug Administration (FDA) for symptomatic relief of persistent facial erythema. Its main mechanism of action involves highly selective vasoconstriction of dilated superficial vessels, in addition to exerting anti-inflammatory effects, mainly through the reduction of mast cells and neutrophilic infiltrate.21 It has demonstrated efficacy with once-daily application, both in clinical assessments of erythema and patient self-assessment, and a favorable safety profile when associated with other topical and physical therapies, such as IPL.17,21
Oxymetazoline is an imidazole derivative approved in 2017 by the FDA in a 1% cream formulation for the treatment of moderate to severe facial erythema in adults.19,21,22 In addition to the vasoconstrictive effect described above, oxymetazoline cream exhibits anti-inflammatory properties by reducing the release of inflammatory cytokines and inhibiting neutrophil phagocytosis.21 It also exerts immunomodulatory effects by reducing the stimulatory capacity of dendritic cells on T cells and modulates arachidonic acid activity.23
Metronidazole (MTZ) is an antibiotic derived from nitroimidazoles that exhibits anti-inflammatory and antioxidant activities and is widely used in the management of papulopustular rosacea. The primary mechanism of action of MTZ involves modulation of neutrophil activity, with reduction of reactive oxygen species (ROS) and inhibition of T cells.7,13,21,22 It also acts on reducing inflammation and combating bacteria that may be involved in the development of rosacea.24 MTZ is available in different formulations, including gel, cream, or lotion at 0.75% (applied twice daily) or 1% gel (applied once daily). Comparative studies have not found significant differences in clinical efficacy between the different vehicles or concentrations.13,15
Adverse effects associated with MTZ use are generally mild and self-limited, including pruritus, burning sensation, desquamation, dryness, or local irritation.15 In mature and sensitive skin, the use of cream or lotion formulations is recommended, as they have better tolerability profiles compared with gel vehicles.22
Azelaic acid (AA) is a dicarboxylic acid indicated for the treatment of mild to moderate inflammatory rosacea. It is available in topical formulations at concentrations of 15% (gel and foam) and 20% (cream), all with comparable efficacy.21 Its mechanism of action integrates antimicrobial, anti-inflammatory, and antioxidant activities.13,21 It acts by reducing the expression and secretion of pro-inflammatory cytokines, such as IL-1β and TNF-α, by keratinocytes. In addition, it protects cells from oxidative damage by reducing ROS production by neutrophils and promoting their elimination. It also modulates cathelicidin activity by inhibiting KLK5 and regulates gene expression, promoting reduction of CAMP and KLK5 mRNA levels in the skin of patients with rosacea.7,13,21 Adverse effects include burning sensation, pain, stinging, pruritus, xerosis, and local irritation, usually mild to moderate in intensity and transient.13,21,22
Ivermectin 1% cream is widely used in the treatment of moderate to severe papulopustular rosacea due to its antiparasitic and anti-inflammatory properties. Its antiparasitic action is related to its ability to act as a ligand-gated ion channel agonist, resulting in paralysis and subsequent elimination of Demodex mites.7,22 In addition, it exerts anti-inflammatory effects by modulating innate and adaptive immune responses, inhibiting the secretion of pro-inflammatory cytokines, such as IL-1β and TNF-α, and increasing the expression of anti-inflammatory cytokines, such as IL-10. It also reduces neutrophil phagocytosis and chemotaxis.13,17,21
In addition to its therapeutic efficacy, ivermectin 1% cream offers the convenience of once-daily application, making it more practical for patients. Adverse effects are mostly mild and localized and it has high tolerability, potentially making it safer and more tolerable than other available topical agents.21
Ivermectin 1% cream has demonstrated superiority in reducing the social burden associated with rosacea when compared with other topical agents,21 although caution is recommended during pregnancy and lactation due to potential risks to fetuses and infants.14
Minocycline is a semi-synthetic antibiotic belonging to the tetracycline class, notable not only for its bacteriostatic activity but also for its anti-inflammatory, immunoregulatory, and anti-angiogenic properties.6,25 Its anti-inflammatory activity occurs through suppression of neutrophil recruitment and pro-inflammatory cytokines, such as TNF-α, IL-6, and IL-1β.6 An experimental study, conducted both in vitro and in vivo, helped elucidate the anti-inflammatory mechanism of minocycline by exposing HaCaT cells and BALB/c mice to inflammatory induction with LL-37 and subsequently treating them with the medication. Treatment significantly reduced the expression of TLR4, NF-κB, inflammatory cytokines, and ROS, suggesting an effect mediated through the TLR4/NF-κB signaling pathway.25 The topical formulation of minocycline 1.5% foam was approved in the United States in 2020, making it the first topical minocycline therapy indicated for treatment of moderate to severe papulopustular rosacea.21 In 2 identical phase III randomized clinical trials, patients who applied minocycline 1.5% foam once daily for 12 weeks showed a reduction in inflammatory lesions compared with the group using vehicle alone. At the end of the study, more than 80% of patients had only residual telangiectasias or mild erythema at the application site. In addition, improvement was observed in Investigator Global Assessment (IGA) success rates, with at least a 2-grade improvement from baseline at week 12.6,25,26 The foam formulation demonstrated good tolerability and may have a lower incidence of systemic adverse effects compared with oral administration.26
Calcineurin inhibitors, such as cyclosporine, pimecrolimus, and tacrolimus, are used in the management of rosacea due to their immunomodulatory and anti-inflammatory properties.
Cyclosporine, in a 0.05% ophthalmic emulsion formulation, is widely used for ocular manifestations of the disease and has been shown to be more effective than artificial tears in improving symptoms of ocular rosacea. Its effect results from the inhibition of pro-inflammatory cytokine production by T lymphocytes in the conjunctiva, in addition to reducing the release of IL-1, IL-8, and TNF-α by monocytes, thereby contributing to the control of local inflammation.7,13
In the skin, pimecrolimus (1% cream) and tacrolimus (0.03%-0.1% ointment) act primarily by modulating T-lymphocyte activation and inhibiting IL-2 transcription. In ocular rosacea, these agents have also been used to treat the local inflammatory process of the eyelids, promoting restoration of the epidermal barrier and control of local inflammation.7,21
Doxycycline is a second-generation tetracycline used in the treatment of papules and pustules due to its anti-inflammatory, rather than antimicrobial, effects. It is approved by the FDA at a dose of 40 mg/day for the management of papulopustular rosacea, and this dosage has been shown to be as effective as antimicrobial doses of 100–200 mg/day but with fewer adverse effects. It should be administered at the end of the day to reduce photosensitivity and taken away from meals containing dairy products, as these reduce its absorption. It is also effective in the treatment of ocular rosacea symptoms.7
Tetracycline is a first-generation antibiotic of the tetracycline family, with an effect similar to that of doxycycline. Subantimicrobial doses are also recommended in order to reduce bacterial resistance. Adverse effects may include nausea, diarrhea, and constipation. All tetracyclines are teratogenic.7
Oral minocycline may also be used off-label for the treatment of rosacea at a dose of 100 mg/day. A new modified low-dose formulation of minocycline is under investigation. Known as DFD-29 (minocycline hydrochloride capsules, 40 mg), the formulation includes 10 mg of immediate-release minocycline and 30 mg of extended-release minocycline. Two studies demonstrated a reduction in inflammatory lesions and improved IGA success rates compared with placebo and doxycycline. Regarding safety, adverse events were similar between groups and generally mild, with upper respiratory tract infection being the most common. No relevant differences were observed in laboratory tests, and no serious events attributable to the medication were reported.27
Macrolides constitute a class of antibiotics that may be used in patients with rosacea who have hypersensitivity or contraindications to tetracyclines, such as pregnant patients. These medications have anti-inflammatory and antioxidant activity. The main adverse effects are gastrointestinal, although they are less frequent with second-generation macrolides such as azithromycin and clarithromycin. Azithromycin, when used at a dose of 250 mg 3 times per week, has shown improvement in papulopustular lesions.7
A multicenter study evaluating gabapentin at a dose of 900 mg/day found improvement in flushing and redness compared with placebo. However, the therapy was ineffective for other rosacea symptoms, such as burning and tingling sensations and psychological effects.28 Another study compared gabapentin 900 mg/day with carvedilol 10 mg/day for the treatment of erythematotelangiectatic rosacea, and both therapies showed similar results in controlling facial flushing, although gabapentin produced a faster response. In addition, gabapentin may be better tolerated and provide greater benefit in patients with other comorbidities, such as migraine and sleep disorders. Mild adverse effects, such as drowsiness and nausea, were observed in 13% of patients.29
Isotretinoin, a retinoid derivative of vitamin A, may be used in cases of persistent rosacea that are resistant to other treatments. Its mechanism of action involves inhibition of pilosebaceous glands and downregulation of TLR-2.22 Although this treatment is off-label, the medication has demonstrated efficacy in patients who do not respond to topical therapies and oral antibiotics. The dose used in most studies is 0.2 mg/kg/day for 6 months. In addition, isotretinoin is effective in the treatment of phymatous rosacea and is indicated in early cases.7,26 Isotretinoin has also shown positive effects in edematous rosacea, known as Morbihan disease, suggesting that its mechanism of action extends beyond effects on sebaceous glands.26
Even at low doses, isotretinoin may cause dryness of mucous membranes and skin, which are its main adverse effects. Laboratory monitoring with liver enzyme and lipid profile measurements should be performed during treatment.22 The medication is a known teratogen and must not be used by patients attempting conception, pregnant individuals, or those who are breastfeeding.7
Antihypertensive agents may be effective in the treatment of flushing caused by rosacea. Among these, beta-blockers are the most commonly used medications, particularly propranolol and carvedilol. The use of these medications requires a prior electrocardiogram as well as consultation with and follow-up by a cardiologist, especially in patients over 50 years of age.10
IPL consists of a device in which light is filtered through specific wavelengths selected according to the absorption characteristics of the target tissues. In rosacea, the target is oxyhemoglobin. IPL acts by reducing inflammation and increasing the upregulation of anti-inflammatory cytokines while downregulating pro-inflammatory cytokines. It may also stimulate collagen synthesis and increase cellular metabolism by affecting the mitochondrial electron transport chain. In addition, it contributes to the destruction of telangiectasias, since it promotes the formation of intravascular thrombi, leading to coagulation.30
One advantage of IPL in the treatment of rosacea is the flexibility of its parameters. In other words, depending on the parameters selected, it is possible to target superficial or deep vessels as well as to focus on the caliber of the vessels to be treated. Tip size is also a favorable aspect: because it is larger than those used in lasers, it allows treatment of broader areas with fewer pulses, making the procedure faster.
IPL is the treatment of choice for the erythematotelangiectatic stage, as it acts on the vascular hyperreactivity associated with rosacea. Treatment allows reduction of blood flow, superficial telangiectasias, and erythema intensity. The therapeutic response is effective and, given the chronic nature of the disease, periodic maintenance is recommended. The generally mild adverse-effect profile also favors IPL treatment. Combining IPL with topical and systemic treatments may enable synergistic therapeutic effects, optimizing outcomes.31 The use of skincare products containing soothing and antioxidant active ingredients may reduce procedural downtime and enhance results.30
Lasers may reduce erythema and promote coagulation of rosacea-associated telangiectasias. The most commonly used are the pulsed dye laser (PDL) and the long-pulsed neodymium-doped yttrium aluminum garnet (Nd:YAG) laser. Studies have compared the efficacy of IPL and PDL and failed to find statistically significant differences between the two methods. IPL appears to be more effective in the treatment of erythema than telangiectasias in severe forms of rosacea. Both techniques are effective when repeated sessions are performed.10 In addition to these options, both fractional and non-fractional ablative lasers, including carbon dioxide lasers (CO2, 10,600 nm) and erbium-doped yttrium aluminum garnet lasers (Er:YAG, 2940 nm), have been used in the treatment of rhinophyma and will be discussed later in this article.
Intradermal injection of botulinum toxin diluted to 10 IU/mL may reduce erythema and facial flushing associated with rosacea. It may also reduce pore size and some papular lesions. Applications may be performed at a dose of 0.05 mL per point, spaced 0.5 cm apart.17,32 It acts by blocking mast cell activity, which reduces erythema induced by LL-37.17 In addition, it blocks the release of acetylcholine in autonomic nerves, reducing cutaneous vasodilation.33 Other neurotransmitters have also been suggested as potentially amenable to reduction by botulinum toxin type A (BoNT-A) injection, including substance P, calcitonin gene-related peptide, and glutamate 34 The effect often lasts 3-4 months, and reapplication after 4-5 months is recommended to maintain symptom remission.32 Some studies have shown that the effect of botulinum toxin in rosacea, when associated with thermal ablation of the stratum corneum using technologies such as laser and fractional thermal systems, may be prolonged.17
Bloom et al. evaluated the safety and efficacy of intradermal abobotulinumtoxinA (15–45 IU) for the treatment of facial erythema of rosacea and reported visible improvement in 93% of patients. No worsening, severe adverse events (such as anaphylaxis), or rebound effect were observed.33 AbobotulinumtoxinA has high molecular weight; therefore, its penetration into the intact stratum corneum is low and it is typically administered via intradermal injection. Methods that produce stratum corneum ablation (such as ablative lasers, microneedle radiofrequency, and electroporation) combined with botulinum toxin application have demonstrated results similar to those of intradermal injection in addition to reducing procedural pain and the risk of muscle paralysis. The primary adverse effect is erythema at the injection site, observed in approximately one-quarter of patients. Ecchymoses and facial muscle involvement were less frequent, occurring in fewer than 5% of cases.34 However, the use of botulinum toxin for the treatment of rosacea is still considered off-label, and additional randomized clinical trials are needed.
Photobiomodulation (PBM) is a therapeutic technique that uses low-intensity light to modulate cellular responses. This approach has emerged as a promising alternative in the treatment of rosacea, mainly due to its anti-inflammatory and tissue-regenerative properties.35
Although the mechanism of action of PBM is not yet fully understood, its action is known to occur largely through light absorption by mitochondrial chromophores, such as cytochrome c oxidase. This interaction stimulates adenosine triphosphate (ATP) production, improves tissue oxygenation, and modulates the inflammatory pathways involved in the pathophysiology of rosacea. Wavelengths in the red spectrum (630–660 nm) and near-infrared range (800–850 nm), commonly emitted by LEDs and low-power lasers, are among the most effective. These spectra have been associated with reduced expression of pro-inflammatory cytokines, such as IL-1β, IL-6, and TNF-α, as well as reduction of immune-cell infiltrates in tissues.35
Despite positive results and the favorable safety profile of PBM, variability among protocols and parameters, such as session frequency, dosage, and treatment duration, remains considerable. In addition, the scarcity of controlled clinical trials assessing PBM in the treatment of rosacea highlights the need for further studies to better understand this therapeutic approach and the cellular responses involved.35
Rhinophyma is a chronic and progressive condition characterized by proliferation of sebaceous glands, thickening of connective tissue, changes in skin coloration, local deformity, irregular exophytic growth, and visible telangiectasias. Although nasal presentation is the most common, similar swellings may affect other regions of the face.36
This form of rosacea responds poorly to conventional treatments, and ablative therapies are often required to reduce lesions.36
The first surgical techniques were described in the seventeenth century, and over time several approaches have been reported, including those of Von Langenbeck (healing by secondary intention), Ollier (decortication), Wood (partial skin graft), Adamopoulos (dermabrasion), Nolan (cryosurgery), and Bohigian (CO2 laser).37
Among ablative techniques, cryosurgery and electrosurgery stand out, as they allow excision of the phyma with excellent hemostasis and at a lower cost. However, they carry risks of necrosis, dyschromia, and unsightly scarring, which may be minimized with appropriate energy settings. Coblation, in turn, uses radiofrequency in a conductive medium at temperatures below 90 °C, decreasing thermal damage risk.36
Excisional techniques involve total or partial removal of the affected tissue. Full-thickness resection eliminates the risk of recurrence but is associated with a greater likelihood of graft or flap failure, less favorable aesthetic outcomes, and a potential need for corrective procedures; consequently, its use has declined in contemporary practice. Partial excision preserves pilosebaceous units and promotes spontaneous re-epithelialization at a lower cost, although strict hemostatic control is required. Dermabrasion may be used as an adjuvant procedure for aesthetic refinement.36
The use of ablative technologies has also increased in the treatment of rhinophyma. Because it has been widely studied, the CO2 laser has become one of the most effective options, producing highly satisfactory aesthetic results. Due to its specific wavelength (10,600 nm), the laser is primarily absorbed by water, enabling precise cutting and vaporization with lower depth of penetration, intraoperative hemostasis, reduced thermal damage, and low risk of scarring, while also allowing rapid re-epithelialization.36
Other ablative lasers, such as Er:YAG and diode lasers (1450–1470 nm), may also be used, providing faster recovery and fewer adverse effects, although they generally produce milder results because they are more superficial than the CO2 laser. PDL may be used as an adjuvant for treatment of vascularization.37,38
A more recent combination of helium plasma with radiofrequency has shown promising results. This technique promotes nearly instantaneous heating and cooling, allowing sequential ablation with minimal bleeding during the procedure and recovery similar to that observed with the CO2 laser, although residual erythema may persist for a longer period.36
The monoclonal antibody that inhibits the calcitonin gene-related peptide (CGRP) has been investigated as a therapeutic option for the treatment of acne and rosacea. CGRP is a peptide associated with the pathogenesis of migraine and is involved in processes of vasodilation and neurogenic inflammation. More recent studies have shown that it is also present in sebaceous glands, and its inhibition may reduce the risk of rosacea development by up to 47%.39
Zeolites, microporous aluminosilicates with tunable physicochemical properties, have the ability to adsorb toxins, modulate local inflammation, and act as carriers for antimicrobial or therapeutic agents. They may also improve dermal absorption of challenging hydrophilic compounds. One example is tranexamic acid, used in the treatment of rosacea and melasma, when combined with zeolitic imidazolate frameworks (ZIF-8). This system facilitates the expression of aquaporin-3 (AQP-3) in keratinocytes, enhancing transepidermal water and solute transport, with decreased erythema and visible skin brightening without adverse effects. Zeolite microneedles represent an evolution in transdermal drug-delivery systems, combining the mechanical integrity, porosity, and bioinertness of zeolites to achieve minimally invasive, long-acting dermal administration of both small molecules and macromolecules.40
Rosacea is a multifactorial dermatosis, and our pathophysiological understanding of the condition has advanced significantly in recent decades. Current evidence points to a complex interaction among immunological, neurovascular, microbial, and environmental factors as the main axes in the development and perpetuation of the clinical condition. Identification of elements such as TLR2 overexpression, the role of LL-37 (an antimicrobial peptide produced by the human body that is part of the innate immune system), activation of TRP channels, and the increased presence of Demodex folliculorum not only clarifies key aspects of the disease but also opens the way for more targeted therapeutic interventions.
Topical treatments represent the first-line therapy for mild to moderate cases, including substances such as metronidazole, azelaic acid, ivermectin, topical minocycline, encapsulated benzoyl peroxide, brimonidine, oxymetazoline, sulfacetamide/sulfur, and, in some cases, off-label retinoids. When necessary, these therapies may be combined with oral medications, notably doxycycline, minocycline, tetracycline, isotretinoin, azithromycin, beta-blockers, and even Janus kinase (JAK) inhibitors, a class of medications that block JAK enzymes to modulate the inflammatory response of the immune system.41
In more severe cases, particularly those with phymatous changes or those refractory to conventional treatment, procedural interventions may be required. These include different laser modalities such as PDL, IPL, potassium titanyl phosphate (KTP), Nd:YAG, CO2, and Er:YAG, as well as approaches such as cryotherapy, electrosurgery, dermabrasion, and other surgical interventions.41
In addition to pharmacological and procedural measures, changes in lifestyle play a central role in the prevention and control of exacerbations. Avoiding known triggers, adopting rigorous photoprotection, using gentle skin care practices, and investing in patient education are essential strategies to minimize flare-ups.
Thus, a combined and personalized approach integrating topical and systemic therapies, procedures, and behavioral changes is fundamental for optimizing symptom control and improving the quality of life of patients with rosacea.
Célia Luiza Petersen Vitello Kalil
ORCID 0000-0002-1294-547X
Approval of the final version of the manuscript, Conception and design of the study, Effective participation in the conduct of the study
Matheus Silva Melo
ORCID 0000-0003-3027-8719
Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Critical review of the literature, Critical revision of the manuscript
Giulia Dambrós Malacarne
ORCID 0000-0002-0313-3840
Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied
Isabela de Liz Pereira
ORCID 0009-0001-4727-8400
Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature
1. Gether L, Overgaard LK, Egeberg A, Thyssen JP. Incidence and prevalence of rosacea: a systematic review and meta-analysis. Br J Dermatol. 2018;179(2):282–9.
2. Abram K, Silm H, Oona M. Prevalence of rosacea in an Estonian working population using a standard classification. Acta Derm Venereol. 2010;90(3):269–73.
3. Tan J, Almeida LMC, Bewley A, Cribier B, Dlova NC, Gallo R, et al. Updating the diagnosis, classification and assessment of rosacea: recommendations from the global ROSacea COnsensus (ROSCO) panel. Br J Dermatol. 2017;176(2):431–8.
4. Two AM, Wu W, Gallo RL, Hata TR. Rosacea: part I. Introduction, categorization, histology, pathogenesis, and risk factors. J Am Acad Dermatol. 2015;72(5):749–58; quiz 759–60.
5. Clanner-Engelshofen BM, Bernhard D, Dargatz S, Flaig MJ, Gieler U, Kinberger M, et al. S2k guideline: Rosacea. JDDG - Journal of the German Society of Dermatology. 2022;20(8):1147–65.
6. van Zuuren EJ, Arents BWM, van der Linden MMD, Vermeulen S, Fedorowicz Z, Tan J. Rosacea: New concepts in classification and treatment. Am J Clin Dermatol. 2021;22(4):457–65.
7. Geng RSQ, Bourkas AN, Mufti A, Sibbald RG. Rosacea: Pathogenesis and therapeutic correlates. Vol. 28, J Cutan Med Surg. 2024;28(2):178–89.
8. Yoon SH, Hwang I, Lee E, Cho HJ, Ryu JH, Kim TG, et al. Antimicrobial Peptide LL-37 Drives Rosacea-Like Skin Inflammation in an NLRP3-Dependent Manner. J Invest Dermatol. 2021;141(12):2885-94.e5.
9. Kościuczuk EM, Lisowski P, Jarczak J, Strzałkowska N, Jóźwik A, Horbańczuk J, et al. Cathelicidins: family of antimicrobial peptides. a review. Mol Biol Rep. 2012;39(12):10957–70.
10. Cribier B. Rosacea: Treatment targets based on new physiopathology data. Ann Dermatol Venereol. 2022;149(2):99–107.
11. Nauroy P, Nyström A. Kallikreins: essential epidermal messengers for regulation of the skin microenvironment during homeostasis, repair and disease. Matrix Biol Plus. 2019;6–7:100019.
12. Zhang M, Ma Y, Ye X, Zhang N, Pan L, Wang B. TRP (transient receptor potential) ion channel family: structures, biological functions and therapeutic interventions for diseases. Signal Transduct Target Ther. 2023;8(1):261.
13. Okońska A, Kozakiewicz J, Ziemba M, Kałuska J, Suprun T, Sokół A, et al. Rosacea pathogenesis and topical treatment options – a review. Quality in Sport. 2025;39:58360.
14. Geng R, Bourkas AN, Sibbald RG. Rosacea: Clinical aspects and treatments. Adv Skin Wound Care. 2023;36(12):626–34.
15. Frazier W, Zemtsov RK, Ge Y. Rosacea: common questions and answers. Am Fam Physician. 2024;109(6):533–42.
16. Cribier B. Rosacea: new data for better care. Ann Dermatol Venereol. 2017;144(8-9):508–17.
17. Paiva-Santos AC, Gonçalves T, Peixoto D, Pires PC, Velsankar K, Jha NK, et al. Rosacea topical treatment and care: from traditional to new drug delivery systems. Mol Pharm. 2023;20(8):3804–28.
18. Mikkelsen CS, Holmgren HR, Kjellman P, Heidenheim M, Kappinnen A, Bjerring P, et al. Rosacea: a clinical review. Dermatol Rep. 2016;8(1):6387.
19. Oliveira CMM, Almeida LMC, Bonamigo RR, Lima CWG, Bagatin E. Consensus on the therapeutic management of rosacea – Brazilian Society of Dermatology. An Bras Dermatol. 2020;95(Suppl 1):53–69.
20. Sobkowska D, Szałapska A, Pawlaczyk M, Urbańska M, Micek I, Wróblewska-Kończalik K, et al. The role of cosmetology in an effective treatment of rosacea: a narrative review. Clin Cosmet Investig Dermatol. 2023;16:1419–30.
21. Dall'Oglio F, Nasca MR, Micali G. Emerging topical drugs for the treatment of rosacea. Expert Opin Emerg Drugs. 2021;26(1):27–38.
22. Lee JJ, Chien AL. Rosacea in older adults and pharmacologic treatments. Drugs Aging. 2024;41(5):407–21.
23. Del Rosso JQ, Tanghetti E. Topical Oxymetazoline Hydrochloride Cream 1% for the treatment of persistent facial erythema of rosacea in adults: a comprehensive review of current evidence. J Clin Aesthet Dermatol. 2021;14(3):32–7.
24. McClellan KJ, Noble S. Topical metronidazole. A review of its use in rosacea. Am J Clin Dermatol. 2000;1(3):191–9.
25. Hua P, Tu Y, Yang Z, He Y, He L, Yao Q, et al. Minocycline inhibits rosacea-like inflammation through the TLR4-mediated NF-κB signaling pathway in vivo and in vitro. PLoS One. 2025;20(5):e0323598.
26. Gold LS, Del Rosso JQ, Kircik L, Bhatia ND, Hooper D, Nahm WK, et al. Minocycline 1.5% foam for the topical treatment of moderate to severe papulopustular rosacea: Results of 2 phase 3, randomized, clinical trials. J Am Acad Dermatol. 2020;82(5):1166–73.
27. Bhatia N, Del Rosso J, Stein Gold L, Lain E, Draelos ZD, Sidgiddi S, et al. Efficacy, safety, and tolerability of oral dfd-29, a low-dose formulation of minocycline, in rosacea. JAMA Dermatol. 2025;161(5):499.
28. Ma G, Zhang Y, Gao Q, Yuan X, Zhou Z, Jian D, et al. Gabapentin improves the flushing of rosacea, but not other rosacea symptoms or quality of life: results from a multicenter, randomized, double-blind, placebo-controlled pilot study. J Am Acad Dermatol. 2025;92(4):920–2.
29. Wei J, Wan M, Chen Q, Fu J, Yang L, Ni R, et al. Gabapentin is an efficacy treatment for facial flushing and erythema of erythematotelangiectatic rosacea: a randomized clinical noninferiority trial. J Am Acad Dermatol. 2025;92(4):927–30.
30. Barbarino SC, Bucay VW, Cohen JL, Gold MH. Integrative skincare trial of intense pulsed light followed by the phyto‐corrective mask, phyto‐corrective gel, and resveratrol <scp>BE</scp> for decreasing post‐procedure downtime and improving procedure outcomes in patients with rosacea. J Cosmet Dermatol. 2022;21(9):3759–67.
31. Kalil CLPV, Reinehr CPH, Milman LM. Intense Pulsed Light: review of clinical indications. Surg Cosmet Dermatol. 2017;9(1):9-17.
32. Bharti J, Sonthalia S, Jakhar D. Mesotherapy with botulinum toxin for the treatment of refractory vascular and papulopustular rosacea. J Am Acad Dermatol. 2023;88(6):e295–6.
33. Bloom BS, Payongayong L, Mourin A, Goldberg DJ. Impact of intradermal AbobotulinumtoxinA on facial erythema of rosacea. Dermatol Surg. 2015;41(Suppl 1):S9–16.
34. Alsaati AA, Alsaadoun D, Kinkar LI, Alkhamis RS, Ahmed WA, Almathami AH. The efficacy and safety of Botulinum Toxin A for the treatment of rosacea: a systematic review. Cureus. 2023;15(12):e51304.
35. Boaretto Netto J, Borges AC, Farias, TG. Could photobiomodulation be used for treatment of rosacea?. Lasers Med Sci. 2025;40(1):250.
36. Dick MK, Patel BC. Rhinophyma. 2023 Aug 8. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
37. Costa TC, Firme WAA, Brito LMR, Vieira MBG, Leite LA de S. Rinofima: opções cirúrgicas utilizadas no serviço de cirurgia Plástica do hospital Agamenon Magalhães - PE. Rev Bras Cir Plást. 2010;25(4):633–6.
38. Kamrani P, Boen M, Fabi SG, Goldman MP. From CO2 to Er:YAG: a comprehensive review of laser treatments for rhinophyma. J Drugs Dermatol. 2024;23(11):932-6.
39. Thang CJ, Lai J, Garate D, Golovko G, Wilkerson MG, Loder EW, et al. Calcitonin gene-related peptide inhibition and development of acne and rosacea. JAMA Dermatol. 2024;160(8):895–8.
40. Dring JC, Kaczynski M, Zureikat RM, Kaczynski M, Forma A, Baj J. Review of applications of zeolites in dermatology: molecular perspectives and translational potentials. Int J Mol Sci. 2025;26(14):6821.
41. Volk K, Ulfers A, Yi RC, Feldman S, Taylor SL. Treatment management for rosacea: current pharmacological and non-pharmacological options. Expert Rev Clin Pharmacol. 2025;18(8):589-605.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}