


Ana Vitoria Lins de Paiva Antunes; Clarissa Brito de Farias; Luciana Cavalcante Trindade; Kamila Pascoal Magno do Nascimento
Funding source: None
Conflict of interest: None
Submitted on: 09/12/2025
Final decision: 10/15/2025
How to cite this article: Antunes AVLP, Farias CB, Trindade LC, Nascimento KPM. Distant cutaneous metastasis from solid neoplasm: a case report. Surg Cosmet Dermatol. 2026;18(1):e20260515.
Cutaneous metastases (CMs) are uncommon manifestations of systemic malignancies, usually indicating poor prognosis. Breast cancer, lung cancer, and melanoma are the main primary tumors associated with CMs. Lesions may mimic several dermatological conditions, which makes diagnosis challenging. Clinical history, histopathology, and immunohistochemistry are essential for confirmation. Management depends on the primary tumor and may include adjuvant therapies tailored to cutaneous involvement. This study reports a case of a patient with CM from a primary pulmonary carcinoma, initially suspected to be a fibroepithelioma of Pinkus, highlighting the importance of differential diagnosis and complementary examinations in clinical practice.
Keywords: Neoplasm Metastasis; Immunohistochemistry; Lung Neoplasms
Metastasis is defined as the development of a tumor at some distance from the primary site and may involve any organ in the body, including the skin.1–5 Cutaneous metastases (CMs) are uncommon, occurring in fewer than 10% of oncology patients, and generally develop months to years after the diagnosis of the primary neoplasm, being associated with a worse prognosis.5–7 The primary tumors that most commonly metastasize to the skin are breast carcinoma, lung carcinoma, and melanoma.2,11
Clinically, CMs may present in a variety of forms, mimicking numerous dermatoses, such as inflammatory diseases, benign tumors, or even primary malignant skin neoplasms, which makes diagnosis challenging for dermatologists.6 In addition, lesions may be asymptomatic or associated with pain and tenderness,3,8 making a detailed clinical history, together with histopathological examination, essential for diagnosis. In some cases, immunohistochemistry is also required for a conclusive diagnosis.
The aim of this study is to report the case of a patient with distant CM from a solid pulmonary neoplasm, initially suspected to be fibroepithelioma of Pinkus. This report emphasizes the importance of including CMs in the differential diagnosis in dermatological practice, particularly in patients with a history of prior malignancies.
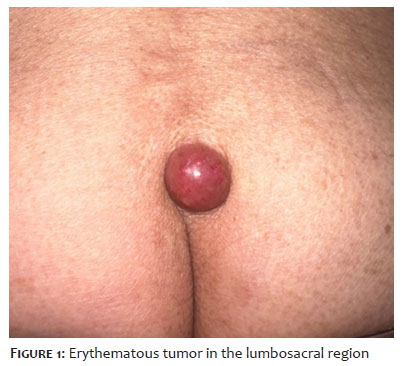
An 84-year-old male patient presented to the outpatient clinic with a lesion in the lumbosacral region, with onset 6 months earlier, associated with intense pain and progressive growth. On physical examination, an erythematous, pearly, rounded, and well-demarcated tumor was observed, with fibroelastic consistency and marked tenderness on palpation (Figure 1). Dermoscopy revealed a pink background lesion with amorphous areas and whitish streaks interspersed with telangiectasias (Figure 2).
The patient had a history of pulmonary adenocarcinoma diagnosed in June 2016, treated with segmentectomy and adjuvant therapy. In addition, metastatic bone lesions were diagnosed in the thoracic spine in 2017 and in the sacrum, iliac bones, and ischium in 2022. At the time of consultation, chemotherapy was on hold due to ongoing cardiologic evaluation.
The diagnostic hypotheses included fibroepithelioma of Pinkus, CM from a primary lung tumor, pilonidal cyst, and amelanotic melanoma.
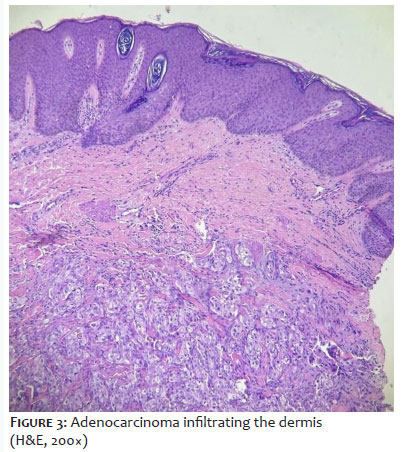
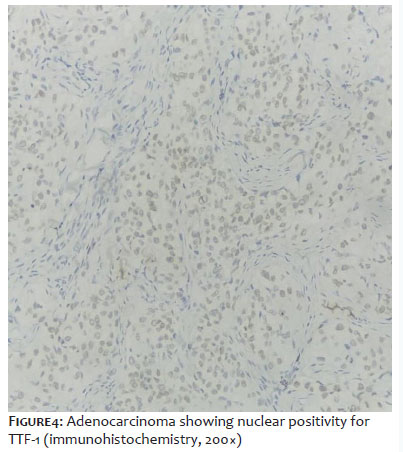
Biopsy and histopathological examination of the lesion revealed an undifferentiated neoplasm with an epithelioid pattern diffusely infiltrating the dermis, with perineural and angiolymphatic involvement (Figure 3). Immunohistochemical analysis of the skin specimen showed morphological features compatible with primary pulmonary adenocarcinoma (Figure 4).
The patient remains under follow-up in the clinical oncology service.
CM is a rare clinical entity in oncology patients and may represent either the first sign of a clinically silent neoplasm or even an indication of tumoral relapse.6,8 In most cases, metastatic skin lesions appear late in the course of the primary disease and are associated with a poor prognosis.7 The age range with the highest incidence of CM is that between 50 and 70 years of age and, on average, onset occurs approximately 5 years after the initial diagnosis.5
The primary tumors most frequently associated with CMs include breast and lung cancers and melanoma; breast cancer is more prevalent in women, whereas lung cancer predominates in men.10 Cutaneous dissemination may occur via hematogenous or lymphatic spread, direct extension, or following surgical procedures.7
Up to 12% of patients with lung cancer may develop skin metastases, most commonly involving the chest, abdomen, head, and neck.1,9 In the present case, the lesion was located in the lumbosacral region. The most common histological type of lung carcinoma that metastasizes to the skin is adenocarcinoma, followed by squamous cell carcinoma and then small- and large-cell carcinomas.8
Clinically, CMs may mimic various dermatoses, presenting as macules, plaques, nodules, blisters, or tumors. They may be asymptomatic or associated with pain, burning, pruritus, and local tenderness.6,8
Lesions secondary to primary lung tumors usually present as normochromic or slightly erythematous subcutaneous nodules, hardened and adhered to deep planes. Most of the time they appear as solitary lesions,10 as observed in the present case.
Due to their resemblance to numerous dermatoses,10 diagnosis is challenging and relies on a complete clinical examination, detailed medical history, histopathological analysis, and immunohistochemistry to determine the subtype of the primary tumor. Histopathological features of metastases tend to resemble those of the primary tumor but are usually more anaplastic.13
In most cases, treatment is directed at the primary tumor, with systemic antineoplastic therapy as the approach of choice. However, in selected cases, adjuvant therapies such as electrochemotherapy, photodynamic therapy, radiotherapy, intralesional therapy, and topical therapy may be used, as well as surgical excision in cases of solitary lesions.10–13
Although uncommon, CMs may precede the diagnosis of an as-yet unidentified primary tumor. Accordingly, dermatologists should be attentive to this possibility, especially in patients with a prior history of malignancies.
Ana Vitoria Lins de Paiva Antunes
ORCID: 0000-0002-5171-245X
Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Clarissa Brito de Farias
ORCID: 0009-0009-5395-045X
Conception and design of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical revision of the manuscript
Luciana Cavalcante Trindade
ORCID: 0000-0002-0643-1093
Author's contribution: Acquisition, analysis and interpretation of data, Critical review of the literature, Critical revision of the manuscript
Kamila Pascoal Magno do Nascimento
ORCID: 0000-0002-2793-0174
Approval of the final version of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
1. Sharma G, Kumar P, Veerwal H, Singh P, Gupta S, Dhingra V. Cutaneous metastases as initial presentation of lung carcinoma. Cureus. 2021;13(5):e15344.
2. Marcoval J, Penín RM, Llatjós R, Martínez-Ballarín I. Cutaneous metastasis from lung cancer: retrospective analysis of 30 patients. Australas J Dermatol. 2012;53(4):288-90.
3. Souza BC, Miyashiro D, Pincelli MS, Sanches JA. Cutaneous metastases from solid neoplasms: literature review. An Bras Dermatol. 2023;98:571-9.
4. Molina Garrido MJ, Guillén Ponce C, Soto Martínez JL, Martínez Y Sevila C, Carrato Mena A. Cutaneous metastases of lung cancer. Clin Transl Oncol. 2006;8(5):330-3.
5. Bittencourt MJS, Fernandes NC, Cuzzi T, Pereira FB. Cutaneous metastasis of a breast cancer diagnosed 13 years before. An Bras Dermatol. 2015;90(3 Suppl 1):134-7.
6. Komurcugil I, Gurel MS, Cakir E, Cengiz FP, Erdemir AT. Cutaneous metastases with different clinical presentations: case series and review of the literature. Dermatol Rep. 2023;15(1):9568.
7. Weimann ETS, Bezerra LS, Valente DS, Kakizaki P, Oliveira Filho RS, Sanches JA. Cutaneous metastasis as the first manifestation of occult malignant breast neoplasia. An Bras Dermatol. 2016;91(5 Suppl 1):105-7.
8. Wong CYB, Helm MA, Kalb RE, Helm TN, Zeitouni NC. The presentation, pathology, and current management strategies of cutaneous metastasis. N Am J Med Sci. 2013;5(9):499-504.
9. Khaja M, Mundt D, Dudekula RA, Al-Abbadi M, Sami S, Alraiyes AH. Lung cancer presenting as skin metastasis of the back and hand: a case series and literature review. Case Rep Oncol. 2019;12(2):480-7.
10. Miyashiro D, Souza BC, Pincelli MS, Sanches JA. Cutaneous metastases from solid neoplasms: literature review. An Bras Dermatol. 2023;98(5):571-9. doi:10.1016/j.abd.2022.04.007. PMID:37126842; PMCID:PMC10547823.
11. Ruiz SJ, García DP, García NG, Pino BG, Rueda ZV, Aristizábal AM. Unusual cutaneous metastatic carcinoma. Ann Diagn Pathol. 2019;43:151399.
12. Sariya D, Ruth K, Adams-McDonnell R, Cusack C, Xu X, Elenitsas R, et al. Clinicopathologic correlation of cutaneous metastases: experience from a cancer center. Arch Dermatol. 2007;143(5):613-20.
13. Queirós CS, Filipe PL, Soares-de-Almeida L. Cutaneous metastases from solid neoplasms in the 21st century: a retrospective study from a Portuguese tertiary care center. J Eur Acad Dermatol Venereol. 2020;34(6):1218-24.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}