


Luiz Roberto Dal Bem Pires Júnior1,2; Carlos Augusto Silva Bastos1
Fonte de financiamento: Não
Conflito de interesses: Não
Data de submissão: 12/07/2025
Decisão final: 11/09/2025
Como citar este artigo: Pires Júnior LRDB, Bastos CAS. Estratégia reconstrutiva com retalhos de avanço na correção bilateral da região malar medial: aplicação dos retalhos de McGregor e Burow. Surg Cosmet Dermatol. 2026;18(1):e20260494.
A reconstrução da região malar é um desafio cirúrgico devido à importância estética e à necessidade de preservar a função. Relata-se o caso de um homem de 75 anos com carcinomas basocelulares bilaterais em malar medial. Após exérese, optou-se por técnicas com retalhos de avanço: retalho de McGregor à direita e retalho de Burow à esquerda. Os retalhos de avanço mostraram-se eficazes por sua simplicidade, boa mobilidade tecidual e capacidade de adaptação às unidades estéticas da face. O paciente evoluiu sem complicações, com bom resultado funcional e estético, reforçando o valor desses retalhos na reconstrução da face.
Keywords: Retalhos Cirúrgicos; Carcinoma Basocelular; Oncologia Cirúrgica; Dermatologia; Face
The malar region represents the largest cosmetic unit of the face, characterized by a slightly convex contour, minimal shadowing or depressions, and heterogeneous skin texture. Despite its skin reservoir, camouflaging surgical scars in this area remains challenging.1
Anatomically, the malar region is divided into 4 subunits: medial, lateral, zygomatic, and buccal. The medial portion is bounded by the lower eyelid, medial canthus, nasofacial sulcus, perialar region, and the superior portion of the nasolabial fold.2 Positioning suture lines along these peripheral boundaries improves scar concealment. When this is not feasible, incisions should follow relaxed skin tension lines (RSTLs) to reduce tension and enhance aesthetic outcomes.3
For small defects in the medial malar region, elliptical excision followed by primary closure with scars aligned along RSTLs is an excellent option. In larger defects, local flaps are preferred, including advancement flaps and their variations.
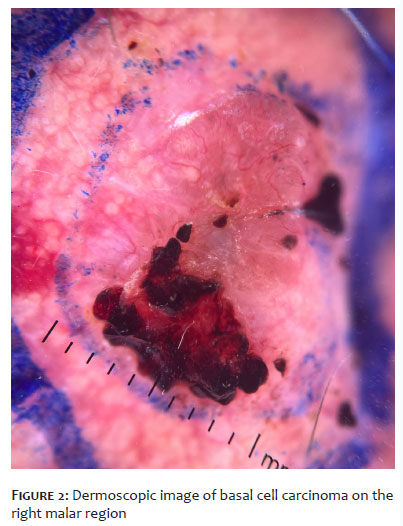
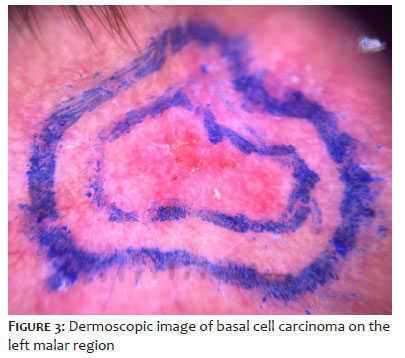
A 75-year-old man, under outpatient follow-up for pemphigus foliaceus and on continuous azathioprine therapy (100 mg/day), presented with a history of multiple basal cell carcinomas (BCCs) on the face. He was diagnosed with 2 new nodular BCCs (Figure 1): one located in the right medial malar region extending to the lower eyelid and lateral nasal wall (Figure 2), and another in the left medial malar region adjacent to the nasal ala (Figure 3).
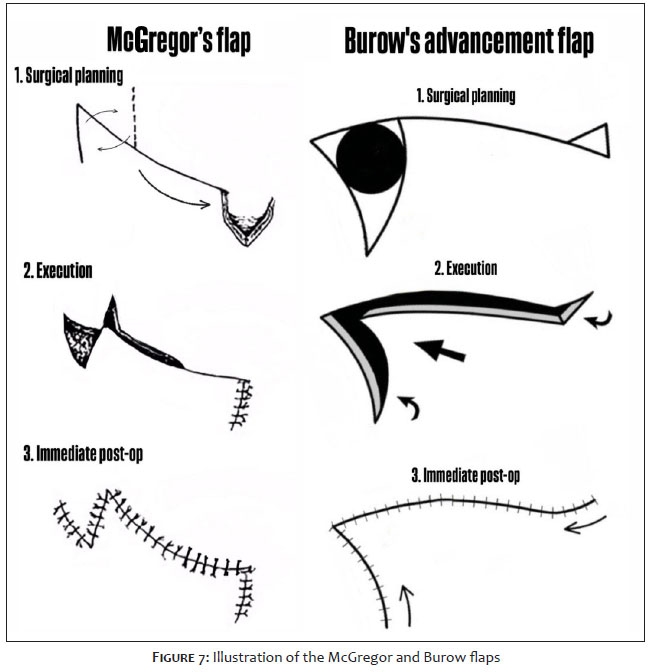
After complete excision of both lesions with adequate resection margins (Figure 4), reconstruction of the right-sided defect was performed using a McGregor flap (Figure 5). This technique involves a lateral incision following the natural curvature of the lower eyelid, which may extend toward the preauricular region anterior to the hairline depending on the defect size. This curvature is essential to provide adequate flap height. At the lateral end of the incision, a Z-plasty was performed, in which the central limb corresponded to the width of the defect, while the ascending and descending limbs were of equal length and oriented at 60° relative to the central limb, facilitating tissue rotation and advancement. Dissection was performed in the subcutaneous plane, allowing appropriate mobilization and subsequent transposition of the flap in the Z-plasty. A Burow's triangle was excised perpendicular to the main incision line to accommodate excess skin. Closure was achieved with 5-0 Vicryl for the deep layer and 6-0 nylon for the superficial layer.
On the left side, the defect was reconstructed using a Burow advancement flap (Figure 6). The defect was initially converted into a triangular shape through an incision extending its base to include the nasolabial fold, aiming to optimize tissue mobilization and improve scar camouflage. Secondary movement of the flap resulted in a skin protrusion (dog ear), which was corrected by excision of a Burow's triangle distant from the primary defect. Dissection was performed in the subcutaneous plane, and closure was achieved with 5-0 Vicryl for the deep layer and 5-0 nylon for the skin (Figure 7).
The patient had an uneventful postoperative course, with satisfactory functional, oncologic, and aesthetic outcomes (Figure 8).
Successful facial reconstruction requires careful consideration of multiple factors. In the present case, the patient posed a particularly challenging scenario, with bilateral involvement of the primary cosmetic unit of the face, a history of multiple prior surgical procedures, and immunosuppression — factors that required careful reconstructive planning.
Advancement flaps were selected due to their simplicity and efficacy. First described more than 2000 years ago by Aulus Cornelius Celsus in De Medicina Octo Libri,4 this type of flap is based on the sliding of adjacent tissue along a single direction vector. Among its variations, U-plasty is widely used across multiple anatomic sites.5,6 When applied to the nasal dorsum in combination with Burow's triangles lateral to the glabellar pedicle, it is referred to as the Rintala flap, as described in 1969.7 H-plasty (or O-H flap) consists of bilateral advancement and is particularly suited to areas with parallel skin tension lines, such as the forehead and eyebrows6; however, their dissection may pose a risk of paresthesia or dysesthesia due to proximity to the supratrochlear and supraorbital nerves.8 T-plasty (or A-T flap), in turn, is useful in regions with limited tissue mobility, such as the lip border and hairline.9,10 The O-L flap represents a unilateral advancement and is termed a Burow flap when combined with excision of Burow's triangles. Its main advantage lies in redistributing dog ears to less conspicuous areas, thereby improving tissue accommodation,10 as demonstrated in the present case, in which lateral skin laxity was used to facilitate closure of the surgical defect.
Despite these advantages, advancement flaps have reduced tissue mobility (compared with more complex flap designs) and require larger incisions to enhance their efficacy. Since the lateral cheek rotation flap described by Mustardé in 1966, several techniques have been developed based on advancing lateral facial skin medially to reconstruct defects. Although there is relative skin laxity in this region, advancement is limited; without adjunctive measures to reduce tension on the flap, it tends to be pulled back to its original site postoperatively.11
To address these limitations, McGregor introduced, in 1973, an approach combining lateral periorbital Z-plasty with advancement flaps, thereby increasing tissue mobility and reducing tension on the lower eyelid. After 15 years of experience with this technique, he reported favorable outcomes, including preservation of the natural appearance of the lateral canthus.12 In the present report, this approach was successfully applied to reconstruction of the lower eyelid and medial malar region, yielding a favorable outcome and supporting its role as a valuable option in the reconstructive armamentarium.
In conclusion, advancement flaps represent an effective option for reconstruction of the malar region, given the relative laxity and mobility of the skin in this area. They allow adequate coverage of skin defects with favorable alignment of incision lines along facial aesthetic units. The ability to combine these flaps with adjunctive techniques, such as Z-plasty and Burow's triangles, further expands their applicability to more complex cases, enabling satisfactory outcomes even in challenging scenarios.
Luiz Roberto Dal Bem Pires Júnior
ORCID: 0009-0001-6728-420X
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Carlos Augusto Silva Bastos
ORCID: 0000-0003-0255-2696
Approval of the final version of the manuscript, Conception and design of the study
1. Menick FJ. Artistry in aesthetic surgery. Aesthetic perception and the subunit principle. Clin Plast Surg. 1987;14(4):723-35.
2. Dobratz EJ, Hilger PA. Check defects. Facial Plast Surg Clin North Am. 2009:17(3):455-67.
3. Hanks JE, Moyer JS, Brenner MJ. Reconstruction of Cheek Defects Secondary to Mohs Microsurgery or Wide Local Excision. Facial Plast Surg Clin North Am. 2017;25(3):443-61.
4. Spencer W. Books VII-VIII. In: Spencer W, ed. Celsus on medicine. Cambridge: Harvard University Press; 1994.
5. Shew M, Kriet JD, Humphrey CD. Flap Basics II: Advancement Flaps. Facial Plast Surg Clin North Am. 2017;25(3):323-35.
6. Krishnan R, Garman M, Nunez-Gussman J, Orengo I. Advancement flaps: a basic theme with many variations. Dermatol Surg. 2005;31(8Pt2):986-94.
7. Rintala AE, Asko-Seljavaara S. Reconstruction of midline skin defects of the nose. Scand J Plast Reconstr Surg. 1969;3(2):105-8.
8. Wiewrodt D, Wagner W. Long-term significance of injury to the supraorbital or supratrochlear nerves during frontoorbital advancement in infancy. Childs Nerv Syst. 2009;25(12):1589-91.
9. Stevens CR, Tan L, Kassir R, Calhoun K. Biomechanics of A-to-T flap design. Laryngoscope. 1999;109(1):113-7.
10. Cerci FB, Fantini BC. Retalhos e enxertos em cirurgia micrográfica de Mohs. São Paulo: Editora Atheneu; 2022.
11. Mustardé JC. The use of flaps in the orbital region. Plast Reconstr Surg. 1970;45(2):146-50.
12. McGregor IA. Eyelid reconstruction following subtotal resection of upper or lower lid. Br J Plast Surg. 1973;26(4):346-54.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}