


Doris Hexsel; Ana Carolina Krum dos Santos; Nathalia Hoffman Guarda Aguzzoli; Vitor Costa Fabris
Funding: None
Conflict of interest: None
Submitted on: 06/30/2025
Final decision: 10/23/2025
Ethical approval: This study protocol was approved by the Hospital Moinhos de Vento Research Ethics Committee on 02/27/2023, under registration number CAAE 65633122.3.0000.5330. Participants signed the Informed Consent Form or Informed Assent Form, and their participation was anonymous.
Acknowledgments: We would like to thank all study participants and dermatologists who shared it, with special mention to Dr. Ilner Souza, who publicized the survey in Brazil's North.
How to cite this article: Hexsel D, Santos ACK, Aguzzoli NHG, Fabris VC. Prevalence of cellulite in Brazilian women: a cross-sectional study. Surg Cosmet Dermatol. 2025;17:e20250489.
INTRODUCTION: Cellulite is a highly prevalent condition among women. However, its prevalence is not currently based in high-quality population studies.
OBJECTIVES: To estimate the prevalence of cellulite among Brazilian women.
METHODS: Cross-sectional study with 385 participants and a convenience sampling. The survey was based on the Hexsel & Hexsel cellulite evaluation scale and shared by SBD members.
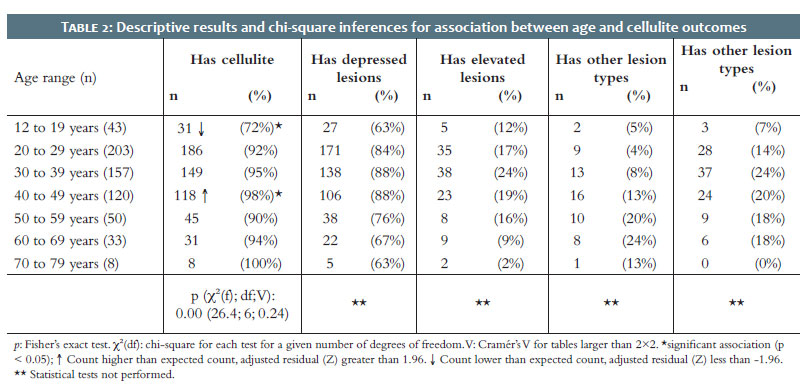
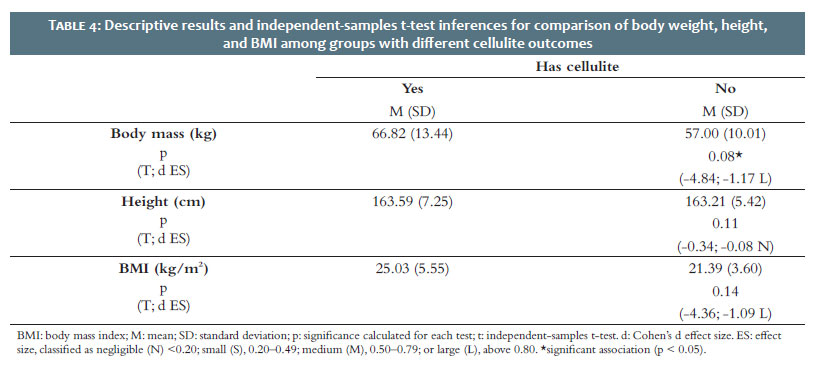
RESULTS: The study included 614 women, primarily between 20 and 29 years-old (32.8%). The prevalence of cellulite was 92.5%. In women between 12 and 19 years-old, the prevalence reached 72%; above 70 years-old, it was 100%. Among women reporting cellulite, 82.7% reported depressed lesions and 19.4% described elevated lesions. There was a significant association between body weight and presence of cellulite.
CONCLUSIONS: Cellulite has an estimated prevalence rate of 92.5% in the Brazilian population; it is less prevalent among adolescents (72%) and reaches scores close to 100% among women over 70 years-old. It is most prevalent among overweight and obese women.
Keywords: Cellulite; Prevalence; Cross-Sectional Studies
Cellulite is a highly prevalent condition in the female population, characterized by irregularities on the skin surface, and it affects primarily the thighs and buttocks. Its typical clinical presentation consists of depressed and elevated skin lesions, especially in areas with a higher percentage of body fat and greater laxity. Although it is highly prevalent among women, with some authors estimating rates of 80% to 90% worldwide, these figures are not based on observational studies conducted at national or global levels.1,2
Specifically in Brazil, one regional study assessed the prevalence of cellulite among female adolescents in the state of São Paulo,3 but there are still no representative data on the prevalence of this condition among Brazilian women as a whole.
Given this gap in statistical knowledge regarding such a highly prevalent condition, this study intended to estimate the prevalence of cellulite among Brazilian women aged 12 years and older.
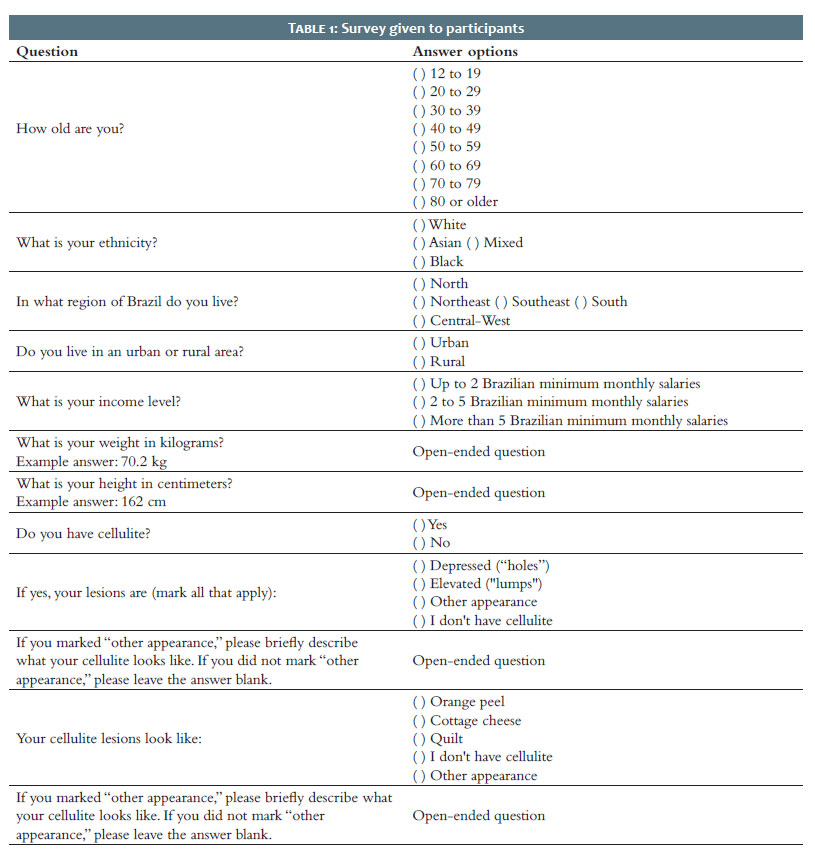
This is a cross-sectional study with a convenience sample, and the inclusion criteria were Brazilian women, literate, aged 12 years or older. Data collection was conducted through an online survey on the Google Forms platform, completed anonymously either by the participant directly or by her legal guardian, after signing the Informed Consent Form (or the Informed Assent Form for participants aged 12 to 18). The instrument was based on the validated Hexsel & Hexsel cellulite scale.4
The survey asked participants about their age, self-declared ethnicity, region of residence, place of residence (urban or rural), income range, weight, height, presence of cellulite in any body area, and the appearance of their lesions. All information was self-assessed.
The survey was distributed and publicized via the Internet. The survey link was shared by the researchers to their contact networks and, in each region of the country, sent to dermatologists through members of the Regional Chapters of the Brazilian Society of Dermatology. The survey was shared through different regional groups as a strategy to mitigate the selection bias inherent to the study design and thereby ensure better representativeness of the Brazilian population. The data were collected from 04/14/2023 to 03/05/2025.5
The project was approved by the Hospital Moinhos de Vento de Porto Alegre Research Ethics Committee before its execution, and the researchers followed the principles of the Declaration of Helsinki and Good Clinical Practice. The sample size was calculated based on the profile of the Brazilian female population according to 2019 data from the Brazilian Institute of Geography and Statistics (IBGE).5 The Brazilian population profile was considered according to age, region, income, place of residence, and color or race, with a tolerance interval of 5% for each category. This resulted in a minimum sample size of 385 participants for the primary objective of the study (analysis of cellulite prevalence).
For the statistical analysis of categorical variables (Tables 1 and 2), the chi-square test was used to evaluate the association between each variable (age, income, and race/ethnicity) and the presence or absence of cellulite. When conducting the chi-square test, if the association Tables and expected count Tables did not meet the prerequisite of expected frequencies equal to or greater than 5, Fisher’s exact test was applied. The significance level for all tests was set at α < 0.05. Cramér’s V coefficient (V) was also calculated to assess the degree of association in Tables larger than 2×2. In statistically significant associations, the adjusted standardized residual, also known as the Z-residual, was calculated as a post-hoc interpretation method. Residual differences were considered significant when greater than 1.96 or lower than -1.96 (confirmation of the null hypothesis = -1.96 > Z > 1.96), with the Z value corresponding to a significance level of alpha equal to 5% (α < 0.05).
The independent-samples t-test was used in the analysis of numerical variables (Table 3) to assess differences in body mass, height, or BMI given the presence or absence of cellulite. In these cases, Cohen’s d effect size was calculated and classified as: negligible (N) < 0.20; small (S), 0.20–0.49; medium (M), 0.50–0.79; or large (L), above 0.80.6,7 The significance level adopted for all analyses was set at α < 0.05. The statistical procedures followed the recommendations of Field (2013)8 and were performed using IBM SPSS Statistics, version 23.0. The sample size was not based on the objectives of the analyses presented in Tables 2 and 3 and, therefore, the data should be interpreted with caution and as exploratory in nature.
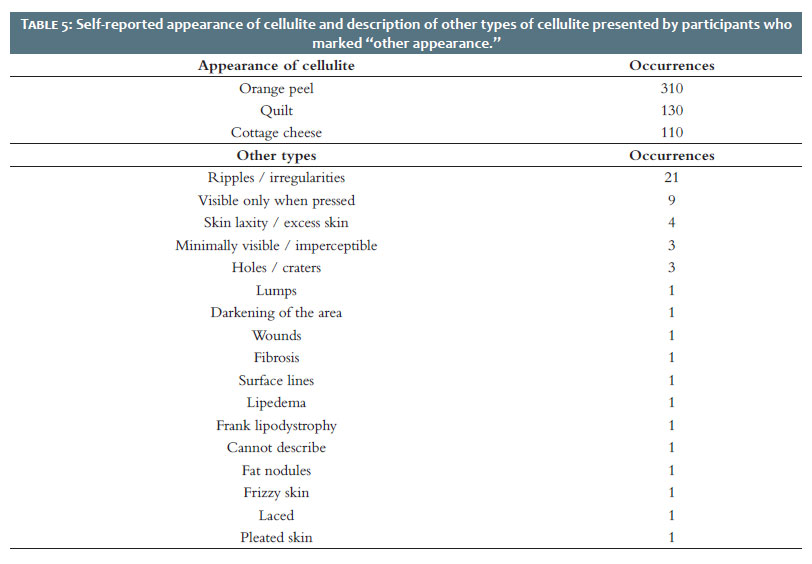
In total, 614 women participated in the study. Participants aged 18 years or older accounted for 98.7% of respondents, whereas adolescents between 12 and 17 years represented only 1.1%. The age group with the highest representation in the sample was 20 to 29 years (32.8%). Of the total, 608 (99.1%) lived in urban areas. The sample included participants from all regions of Brazil: 29 (4.7%) from the Central-West, 41 (6.7%) from the North, 155 (25.2%) from the Northeast, 178 (29%) from the Southeast, and 211 (34.3%) from the South. Complete demographic data are shown in Table 1. Tables 3 and 4 show the relationship between the presence of cellulite and self-reported ethnicity, income, weight, height, and BMI. Table 5 presents reports from participants who classified the appearance of their cellulite as “other appearance.”
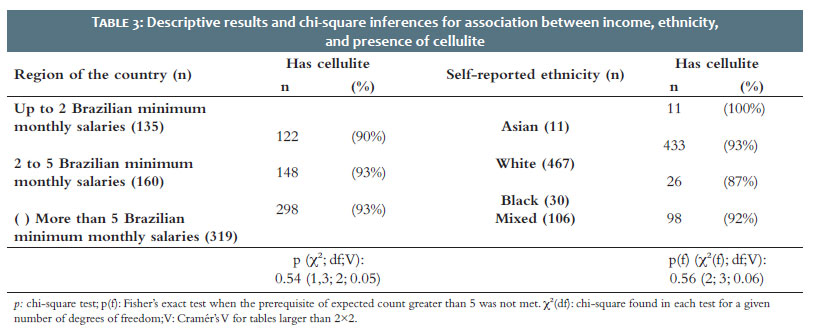
The vast majority of participants (92.5%) reported having cellulite. Of these, 82.7% reported depressed lesions, and 19.4%, elevated lesions. A little more than half (50.3%) reported an “orange peel” appearance. When stratified by region, 100% of participants from the North and Center-West reported having cellulite, as did 93% in the South and Southeast and 88% in the Northeast.
This study estimated the prevalence of cellulite across different age groups in the Brazilian female population. The finding that cellulite is less prevalent among younger women (12 to 19 years) is consistent with expectations, given what is known about the pathophysiological mechanisms involved in the development of cellulite.9-11 Interestingly, the self-reported prevalence in this age group was similar to that found in the study by Soares et al.,3 which estimated the prevalence of cellulite in adolescents through clinical evaluation conducted by trained professionals. This indicates that self-diagnosis of cellulite is reasonably accurate even when performed by younger patients.
The prevalence of 100% in the population aged 70 to 79 years was also expected, since skin laxity is an aggravating factor for cellulite that worsens with aging, showing that the pathophysiological mechanisms responsible for the onset of cellulite tend to add up and intensify with advancing age.9-11 The study also found increased prevalence of cellulite in the 40 to 49 age group. This finding may be a statistical fluctuation in the analysis (type I error, false positive) and/or be the result of the fact that assessments were self-reported. Participants in this age group may be more perceptive than others regarding changes in how their body looks.
No statistically significant differences were observed in the prevalence of cellulite among patients of different ethnicities or household income levels, underlining the universality of this condition among Brazilian women. Traditionally, Caucasian ethnicity has been considered a risk factor for developing cellulite,12,13 but the data from this study do not support that hypothesis. Because Brazil is a highly mixed-race country, it is possible that ethnic influences on the development of cellulite play a smaller role among Brazilians, with their effect overwhelmed by factors such as overweight and age.
Many studies cite estimates of 80% to 90% prevalence for cellulite in the general female population,13,14 but the data that originated these estimates lack statistical grounding in prevalence studies with broad population coverage. Several articles mention these estimates without citing primary sources. The data from this study indicate an even higher overall prevalence of cellulite among Brazilian women, at 92.5%.
In this study, individuals with cellulite also had higher body weight, but no significant differences were found in terms of height or BMI compared with women without cellulite. A higher prevalence of cellulite among women with greater body weight was expected, given that the thickness of the subcutaneous adipose tissue influences how the skin surface looks. 9,10 The mean BMI of participants with cellulite was 25.03, compared with 21.39 for participants without cellulite. This difference was not significant, likely due to the study’s low statistical power, since this was a secondary analysis variable that was not included in the sample size calculation.
Regarding statistical analyses of secondary data, subgroup analyses were not performed based on the type of cellulite lesion reported by participants (for example, depressed versus elevated lesions). Given the large number of analyses that would have been required (more than 60) and the considerable sample size of this study (614), there would have been a prohibitively high probability of type I errors (false positives), which would have made a reliable interpretation of the results impossible. Thus, the data were reported quantitatively and descriptively in Table 1, stratified by age group. In the specific case of cellulite prevalence by region, statistical tests were not performed because the participants’ region of residence is only a confounding factor, indirectly related to determinants that could actually influence the development of the condition, such as ethnicity, income, and weight.13
This study has limitations. The main one is the use of a convenience sampling rather than a randomized sample, which increases the risk of selection bias, partially mitigated by the inclusion of a large number of participants. Other biases inherent to the study methodology include the exclusive participation of literate women with Internet access, which reduces participation among socially vulnerable women, and the fact that cellulite was self-assessed. In addition, although all women could participate in the survey once they received the recruitment link, it is likely that women with cellulite were more inclined to respond, possibly leading this study to overestimate the prevalence of the condition.
Even though the distribution of participants in this study does not reflect the Brazilian population in terms of income, age group, ethnicity, and state population, the sample included 467 Caucasian women of various income levels, aged 20 to 59 years, a number large enough to ensure internal validity for data analysis in this population subgroup. Self-assessment is also not a major limitation, since, as previously discussed, even young women seem able to diagnose the presence of cellulite with a reasonable degree of accuracy. Thus, even under a conservative interpretation, the data reported in this study have external validity for the subgroup of Caucasian women aged 20 to 59 years.
Prevalence of cellulite is extremely high among Brazilian women, with an estimated rate of 92.5%. It is less common during adolescence (72%) and may reach values close to 100% in older age groups, above 70 years. It is more prevalent among women with higher body weight, and in the Brazilian population, self-declared ethnicity does not appear to be a risk or protective factor for the development of cellulite.
Doris Hexsel
ORCID: 0000-0002-0615-9026
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical revision of the manuscript.
Ana Carolina Krum dos Santos
ORCID: 0000-0001-9863-1836
Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Critical review of the literature, Critical revision of the manuscript.
Nathalia Hoffman Guarda Aguzzoli
ORCID: 0000-0001-6472-0910
Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
Vitor Costa Fabris
ORCID: 0000-0002-3540-2769
Author’s contribution: Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
1. Luebberding S, Krueger N, Sadick NS. Cellulite: an evidence-based review. Am J Clin Dermatol. 2015;16(4):243-56.
2. Nürnberger F, Müller G. So-called cellulite: an invented disease. J Dermatol Surg Oncol 1978;4(3):221–9.
3. Soares JLM, Rocha VA, Sanudo A, Miot HA, Bagatin E. Prevalence and factors associated with gynoid lipodystrophy in Brazilian adolescent girls: a cross-sectional study. Int J Dermatol. 2022;61(7):861-6.
4. Hexsel DM, Dal’Forno T, Hexsel CM. A validated photonumeric cellulite severity scale. J Eur Acad Dermatol Venereol. 2009;23(5):523-8.
5. IBGE. Diretoria de Pesquisas, Coordenação de Trabalho e Rendimento. Pesquisa Nacional por Amostra de Domicílios Contínua; 2019. Disponível em https://www.ibge.gov.br/.
6. Bakeman R. Recommended effect size statistics for repeated measures designs. Behav Res Methods. 2005;37(3):379-84.
7. Cohen J. Statistical power analysis for the behavioral sciences. Hillsdale: Erlbaum; 1988.
8. Field A. Discovering statistics using IBM SPSS statistics. Sage; 2013.
9. Hexsel DM, Abreu M, Rodrigues TC. Side-by-side comparison of areas with and without cellulite depressions using magnetic resonance imaging. Dermatol Surg. 2009; 35(10):1471–7.
10. Hexsel DM, Siega C, Schilling-Souza J. A comparative study of the anatomy of adipose tissue in areas with and without raised lesions of cellulite using magnetic resonance imaging. Dermatol Surg. 2013;39(12):1877-86.
11. Tokarska K, Tokarski S, Woźniacka A, Sysa-Jędrzejowska A, Bogaczewicz J. Cellulite: a cosmetic or systemic issue? Contemporary views on the etiopathogenesis of cellulite. Postepy Dermatol Alergol. 2018;35(5):442-6.
12. Arora G, Patil A, Hooshanginezhad Z, Fritz K, Salavastru C, Kassir M. Cellulite: presentation and management. J Cosmet Dermatol. 2022;21(4):1393-1401.
13. Gabriel A, Chan V, Caldarella M, Wayne T, O'Rorke E. Cellulite: current understanding and treatment. Aesthet Surg J Open Forum. 2023;21:5:ojad050.
14. Friedmann DP, Vick GL, Mishra V. Cellulite: a review with a focus on subcision. Clin Cosmet Investig Dermatol. 2017;10:17-23.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}