


Sabrina Covre Jaques1; Isadora Busto Silva2; Beatriz Azevedo Nunes1; Carlos Augusto Silva Bastos2; Betina Werner3
Funding: None
Conflict of interest: None
Submitted on: 06/26/2025
Final decision: 09/22/2025
How to cite this article: Jaques SC, Silva IB, Nunes BA, Bastos CAS, Werner B. Collision tumor of melanoma and basal cell carcinoma: case report with exuberant dermoscopy. Surg Cosmet Dermatol. 2025;17:e20250487.
A collision tumor is a rare condition that occurs when two or more cutaneous tumors coexist in the same anatomic region. The objective of this study is to present the case of a 70-year-old male patient with a collision tumor of melanoma in situ and a nodular basal cell carcinoma, discussing clinical, histological, and therapeutic aspects, highlighting the importance of differential diagnosis in complex cutaneous neoplasms. Given the limited number of cases in the literature, predicting the biological behavior of collision tumors is challenging. Therefore, careful patient follow-up and further studies are necessary to better understand this condition.
Keywords: Collision Tumor; Melanoma; Basal Cell Carcinoma; Dermoscopy
The simultaneous presence of two distinct neoplastic cell populations in adjacent areas, maintaining well-defined histological boundaries, defines collision tumors. This is an extremely rare event when it involves two malignant neoplasms.1,2 The literature on this entity remains limited, both in terms of the number of documented cases and the elucidation of the mechanisms that lead to the coexistence of two distinct patterns of tumor differentiation.
This case report describes a patient with a collision tumor of melanoma and basal cell carcinoma (BCC), addressing clinical, histological, and therapeutic aspects and highlighting the importance of differential diagnosis in complex cutaneous neoplasms.
A 70-year-old male construction worker was referred to the Dermatology service due to a lesion on his back. The patient could not report how long the lesion had been present, possible ectoscopic changes over time, or associated symptoms. His comorbidities included hypertension and cardiac arrhythmia
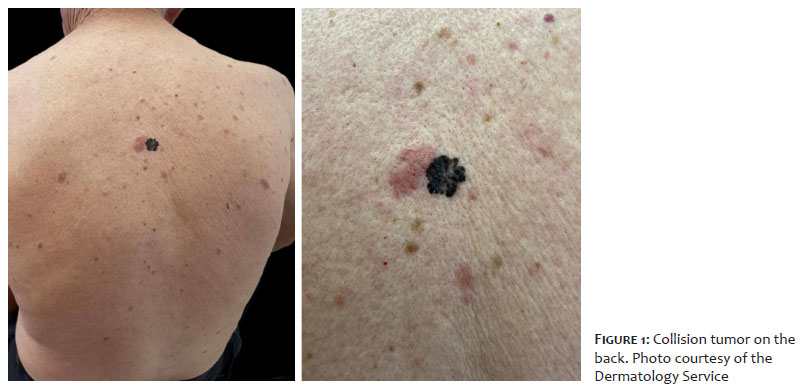
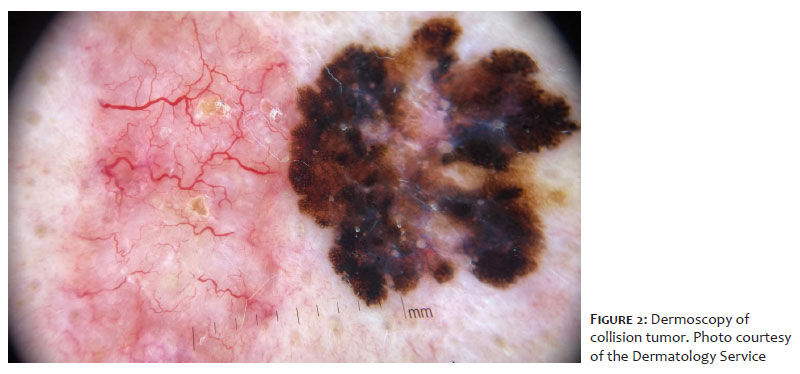
Complete dermatological examination revealed an asymmetric plaque with irregular borders measuring approximately 2.94 × 2.55 cm, consisting of two adjacent lesions with distinct characteristics (Figure 1). On the left, the lesion was erythematous, poorly defined, elevated, with coarse arborizing telangiectasias and small ulcerations on dermoscopy, measuring approximately 1.41 × 2.55 cm. On the right, the lesion was darkly pigmented, well-defined, measuring 1.57 × 1.53 cm, with a multicomponent dermoscopic pattern, showing an atypical network, branched streaks, amorphous areas, and a blue-gray veil (Figure 2). No lymphadenopathy was identified on physical examination.
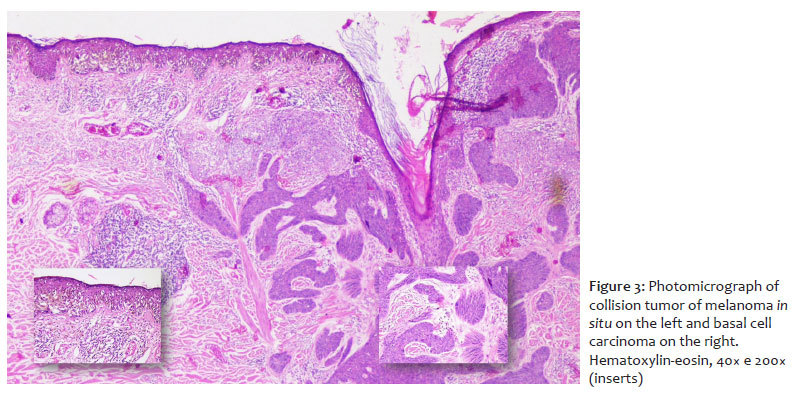
The lesion was excised, and histopathological examination confirmed the diagnosis of a collision tumor composed of melanoma in situ (on the right) and nodular BCC (on the left). The melanoma was classified as Clark level I, and showed absence of ulceration, absence of mitoses, lymphovascular embolization, and neurotropism, moderate lymphocytic infiltration, presence of tumor regression of less than 75%, absence of microsatellitosis, and free lateral and deep margins (Figure 3). The melanocytic neoplasm consisted of isolated cells and nests of atypical epithelioid cells, with multifocal pagetoid scatter and abundant pigmentation. In the underlying dermis, pigment incontinence, moderate lymphocytic infiltrate, and signs of severe actinic damage were observed. The BCC exhibited nodular, solid, and adenoid patterns, with infiltrative areas and focal pigmentation; ulceration; involvement up to the mid-reticular dermis; absence of perineural infiltration; and free lateral and deep margins.
The patient underwent margin widening, and histopathological examination revealed actinic damage, cicatricial changes, and diffuse melanocytic hyperplasia with a reactive pattern.
During follow-up, the surgical wound was intact, with no signs of relapse. A new non-melanocytic lesion was identified on the right pectoral region, and histopathological examination confirmed the diagnosis of pigmented and ulcerated BCC with an expansive growth pattern. The patient remained under regular follow-up at the service, with no new lesions or suspicion of local relapse.
Among collision tumors, reports of melanoma associated with BCC are uncommon. Collision tumors, whether benign or malignant, result from the proliferation of cells from different lineages and may coexist within the same lesion, forming tumor combinations.3
Collision tumors are defined as the occurrence of two neoplasms in close proximity that maintain sharply distinct boundaries.1 Some authors suggest the possibility of a single histogenesis with unknown biological behavior.4 Others consider these combinations to occur by coincidence, while still others hypothesize that the presence of one tumor may induce stromal changes responsible for the development of a second tumor.2 In cases of collision between melanoma and BCC, the melanoma may arise randomly from nests of melanocytic cells present within the BCC.5
The association of two malignant neoplasms is a rare event. The first documented case of melanoma associated with BCC was reported by Kao in 1983.2 The largest review on the subject analyzed 78,000 skin cancer biopsies and identified only 11 cases of collision of melanoma and BCC.3 Of these, seven were located on the trunk and four on the upper limbs. Among the patients, six were men and five were women, with a mean age of 53 years.3
The literature still contains few reports on this condition, as well as the exact etiology underlying this bidirectional differentiation, and reports of collision tumors of BCC and melanoma are even scarcer. A literature review identified 27 cases of collision tumors involving melanoma and BCC, most of which showed no intermingling of tumor cells and had well-defined margins.6
Given the rarity of these cases, there is ongoing debate regarding the most appropriate terminology. Terms proposed in the literature include “malignant melanocytic basal tumor,” describing a biphasic tumor composed of BCC and malignant melanoma7; “colonization,” referring to the unique situation in which melanoma in situ extends and colonizes a BCC3; and “melanoma associated with BCC.”2
Studies indicate that collision tumors, such as melanoma associated with BCCs and squamous cell carcinomas (SCCs), occur more frequently in patients under intense sunlight exposure or with genetic predisposition, reflecting the complexity of carcinogenic processes.8 In the present case, the patient had risk factors such as a low phototype and marked sunlight exposure. Collision tumors seem to affect men more frequently than women, with a higher incidence after 50 years of age.3 Case reports of tumor collision involve various anatomical sites, including the back, cervical region, ears, and face.5,9,10,11 Although melanomas associated with BCC or SCC may, in some situations, exhibit less aggressive behavior, there are case reports of fatal outcomes, often associated with Breslow’s depth greater than 1.5 mm.3 Prognosis and treatment depend on the most aggressive tumor; however, early intervention and excision with adequate margins generally result in favorable outcomes, as observed in the present case.6
Outpatient follow-up for a period of 5 to 10 years is essential to assess for possible local relapse and for the early diagnosis of a second primary melanoma at another site. Patients with a prior history of melanoma have a 10% risk of developing a second melanoma within 5 years.6 After a second episode, this likelihood increases to 30%.6 In this case report, a new BCC was diagnosed in the pectoral region during follow-up, with no other suspicious melanocytic lesions identified through early 2025.
Given the limited number of case reports available in the literature, predicting the biological behavior of these lesions is challenging. Therefore, rigorous patient follow-up and further studies aimed at improving our understanding of this condition are necessary.
Sabrina Covre Jaques
ORCID: 0000-0001-5617-0533
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Critical review of the literature, Critical revision of the manuscript
Isadora Busto Silva
ORCID: 0000-0003-3502-1840
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Critical review of the literature, Critical revision of the manuscript.
Beatriz Azevedo Nunes
ORCID: 0000-0001-8057-0799
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Critical review of the literature, Critical revision of the manuscript.
Carlos Augusto Silva Bastos
ORCID: 0000-0003-0255-2696
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Betina Werner
ORCID: 0000-0002-9671-5603
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. Boyd AS, Rapini RP. Cutaneous collision tumors: an analysis of 69 cases and review of the literature. Am J Dermatopathol. 1994;16:253-7.
2. Papa G, Grandi G, Pascone M. Collision tumor of malignant skin cancers: a case of melanoma in basal cell carcinoma. Pathol Res Pract. 2006;202:691-4.
3. Satter EK, Metcalf J, Lountzis N, Elston DM. Tumors composed of malignant epithelial and melanocytic populations: a case series andreview of the literature. J Cutan Pathol. 2009;36(2):211-9
4. Scruggs JM, Rensvold EA, Parekh PK, Butler DF. Cutaneous collision cancers: a report of two squamomelanocytic malignancies and review of the literature. Dermatol Surg. 2011;37(11):1679-83.
5. Hirakawa E, Miki H, Kobayashi S, Nomura Y, Ohmori M. Collision tumor of cutaneous malignant melanoma and basal cell carcinoma. Pathology - Research and Practice, 1998;194(9):649–53.
6. Medeiros PM, Alves NRM, Silva CC, Faria PCP, Barcaui CB, Piñeiro-Maceira J. Colisão de neoplasias malignas na pele: melanoma associado a carcinoma basoescamoso. An Bras Dermatol. 2015;90(3 Supl 1):S38-41.
7. Pool SE, Manieei F, Clark WH, Harrist TJ. Dermal squamomelanocytic tumor: a unique biphenotypic neoplasm of uncertain biological potential. Hum Pathol 1999;30:525.
8. Sahu, AK. "Coexistence of melanoma and non-melanoma skin cancer: a rare occurrence." Clin Exp Dermatol. 2019;44(5):510-3.
9. Coskey RJ, Mehregan AH. The association of basal cell carcinomas with other tumors. J Dermatol Surg Oncol. 1987;13:553–5.
10. Burkhalter A, White WL. Malignant melanoma in situ colonizing basal cell carcinoma: a simulator of invasive melanoma. Am J Dermatopathol. 1997;19:303–7.
11. Wang H, Benda PM, Piepkorn MW. Parasitism of basal cell carcinoma by lentigo maligna melanoma. J Am Acad Dermatol. 2003;48:S92–4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}