


Monika Sekar1; Sankararaman Balasubramanian2; Srivenkateswaran Kothandapany1; Vinitha Kumari1; Jayamaliga Vijayananth1
Funding: None
Conflict of interest: None
Submitted on: 05/30/2025
Final decision: 10/15/2025
How to cite this article: Sekar M, Balasubramanian S, Kothandapany S, Kumari V, Vijayananth J. Post-traumatic nail deformity presenting as a painful keel-like ridged nail and its surgical treatment. Surg Cosmet Dermatol. 2005;17:e20250479.
Trauma to the nail is a common cause of nail dystrophies and deformities. When not managed properly at initial presentation, nail injuries may result in permanent deformities and can cause functional and aesthetic abnormalities. This article reports on the case of a man who presented with a painful, ridged nail following trauma. The condition was treated with surgical excision of the keel-like nail plate and removal of the offending matrix.
Keywords: Nails; Nails, Malformed; Wounds and Injuries; Surgical Procedures, Operative
Fingernails play an important role in hand function. They protect the dorsal surface of the distal phalanges, increase fingertip sensitivity, facilitate pinching and scratching, and have an aesthetic role. Injuries to the nail apparatus are common. Crush trauma is the most common cause of fingernail injuries in children and young adults. These injuries may later present with nail deformities.1 Proper initial management is essential to prevent functional or aesthetic abnormalities.
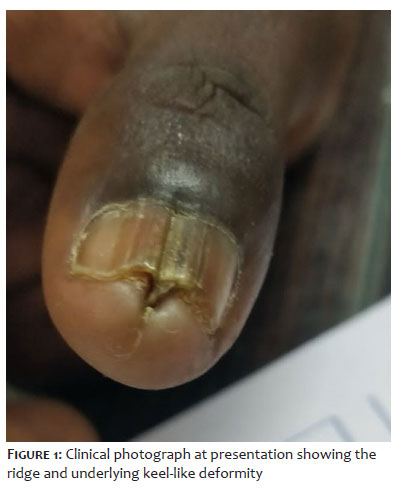
A 34-year-old male fisher presented with pain in the left thumbnail of 4 months’ duration. There was no discharge, itching, or swelling beneath the nail plate. The patient reported a cut injury 2 years prior. There was no history of animal handling or gardening. Other causes were ruled out. Dermatological examination revealed nail discoloration with a deep, T-shaped longitudinal ridge and thickening impinging on the nail bed at midline beneath the left thumbnail (Figure 1), resembling the keel of a ship (Figure 2). Total nail plate excision was planned to remove the painful ridge, along with the germinal matrix to prevent re-growth.
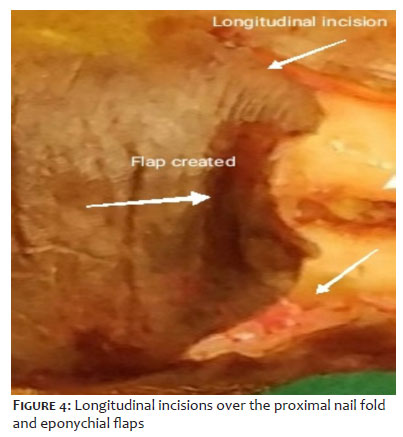
Preliminary investigations found no abnormalities. Clinical features were distinctive and imaging examinations were deemed unnecessary. A digital block was administered using plain xylocaine. A tourniquet was applied around the base of the finger. The entire nail plate with the longitudinal ridge was separated from the nail bed and removed (Figure 3). Two longitudinal incisions were made on either side of the proximal nail fold, and flaps were created to expose the germinal matrix (Figure 4).
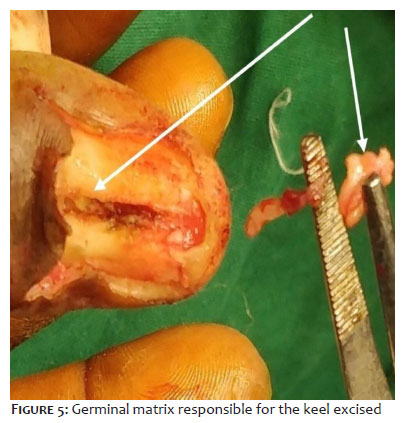
The length of the crater in the nail bed and germinal matrix causing this keel-like deformity (Figure 5) was excised. The wound in the nail bed was sutured with 4-0 Vicryl Rapide (Figure 6). Postoperative healing was satisfactory. Nail growth was complete in a few weeks as the two separate parts grew very close together (Figure 7) and the patient experienced complete pain relief.
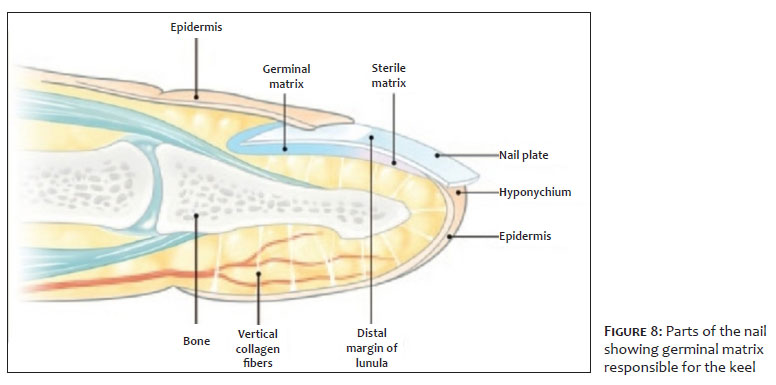
Nails are ectodermal appendages that cover the dorsal aspects of the digits. They provide protection and integrity to the fingertip, in addition to facilitating fine hand movements. Anatomical abnormalities of the nail unit may interfere with these functions.3 Nail injuries are common in both industrial and domestic settings and can result in acute and chronic nail deformities.4 Proper knowledge and understanding of nail anatomy (Figure 8) are essential for the treatment of nail injuries.
Nails begin to develop at around 10 weeks of intrauterine life from a keratinized plate on the dorsum of the finger. The perionychium includes the nail and its adjacent structures: hyponychium, nail bed, and nail folds. The eponychium is the proximal soft tissue on the dorsal aspect of the nail continuous with the dorsal skin. The white arc just distal to the eponychium is called the lunula. Beneath the nail plate lies the nail bed. The nail bed distal to the lunula is called the sterile matrix, and proximal to that is the germinal matrix. The distal attachment of the nail is the hyponychium, a pulp of keratinous mass rich in polymorphonuclear leukocytes and lymphocytes. The nail fold on either side is called the paronychium.
Approximately 90% of nail growth originates from the germinal matrix, while the sterile matrix contributes about 10% and provides adherence of the nail plate to the nail bed. Fingernails grow at a rate of 0.1 mm per day, faster than toenails.
Nail growth ceases for approximately 21 days after trauma. An increase in growth is seen for the next 50 days, then a decrease for the following 30 days. Normal nail growth usually resumes 100 days after trauma. Permanent loss or deformity may occur when the germinal matrix, which is responsible for nail growth, is lost or damaged.2 Complete regrowth of an avulsed fingernail or toenail takes 4-5 months and 10-12 months, respectively.3
Nail injuries include being crushed by machinery, road traffic accidents, sports injuries, iatrogenic causes, self-inflicted injuries such as nail biting, insertion of artificial nails, improper manicure, and direct damage to the nail matrix or nail bed, such as crushing, cutting, or avulsion.
The pathophysiology of traumatic ridged nails involves disruption in normal nail growth. The traumatic event directly injures the germinal matrix and nail bed, temporarily slowing or halting of nail growth. This can cause the formation of scar tissue, altering nail growth rates and creating ridges and lumps, as well as potentially complete nail loss or separation from the nail bed. Damage to nail matrix and nail fold can result in characteristic post-traumatic defects such as split nails, nonadherent nails, or dull streaks.5
In the present case, an old trauma may have driven the germinal matrix into the subungual tissue. This embedded matrix, along with the normal matrix, may have continued to grow. The embedded matrix would then have formed a nail plate structure beneath the nail, causing pain. A longitudinal ridge ran the whole length of the nail, extending from its deep aspect, akin to the keel of ship (Figure 2).
Traumatic nail bed injuries can be classified into two types, closed and open injuries. Depending on the nature and anatomic location of the injury, they are divided into simple or complex lacerations, avulsion injuries, amputations, injuries involving the paronychium, or fractures.
Avulsion injuries result from crush or grinding mechanisms. Sharp lacerations occur when objects penetrate the nail plate with sufficient force. Mild crush injuries to the distal phalanx or fingertip can produce a subungual hematoma. Open injuries may occur with or without nail bed loss.2
Left untreated, these nail injuries can result in various deformities, including eponychial loss, onycholysis, ridged nails, split nails, pincer nails, and bony irregularities.2 They can also cause functional and aesthetic abnormalities.1 Phalangeal fractures are present in 50% of fingernail injuries.
Longitudinal ridges may also have other non-traumatic causes, including peripheral vascular disease, myxoid cyst, median nail dystrophy, habit-tic nail deformity, Darier’s disease, lichen planus, or may even be seen in otherwise normal nails. Median canaliform dystrophy typically affect thumbnails, producing a longitudinal depression with transverse ridges, creating a “washboard” or “fir tree” pattern.6 Longitudinal ridges with V-shaped nicks at the free end are found in Darier’s disease.
Trachyonychia, which produces a rough surface affecting the entire nail plate, is often associated with longitudinal ridging. It can be idiopathic or related to alopecia areata, psoriasis, lichen planus, and ichthyosis vulgaris.7
In surgical management of nail injuries, closed injuries with subungual hematoma may be treated with trephination. For open injuries, the nail plate is partially or completely avulsed to assess the nail bed for lacerations or fractures. If present, nail bed lacerations are repaired using 6-0/7-0 chromic catgut. Replacement of nail plate is indicated in cases of lacerations of the nail bed or eponychial fold to prevent synechiae formation. Further nail bed loss can be managed with split-thickness nail bed grafts harvested from an adjacent nail bed or the great toe, or with a local V-Y advancement flap. In cases of complete nail bed loss with scarring, vascularized nail bed grafts may be used. Phalangeal fractures require protective splinting with a volar slab or finger splint for three weeks, while distal fractures may require K-wire fixation and splinting of the nail plate.2
In the case presented, the patient’s initial nail injury may not have been adequately treated, resulting in a painful ridged nail with a keel-like deformity. This type of deformity has not been previously reported in literature. Surgical management provided pain relief. However, since the matrix in the deformed area was excised, the regrown nail plate was divided into two juxtaposed halves. A partial germinal matrix graft might have yielded a better outcome.
Monika Sekar
ORCID: 0009-0004-1909-5166
Approval of the final version of the manuscript, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Sankararaman Balasubramanian
ORCID: 0000-0002-1990-964X
Approval of the final version of the manuscript, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Srivenkateswaran Kothandapany
ORCID: 0000-0002-3855-1858
Approval of the final version of the manuscript, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Vinitha Kumari
ORCID: 0009-0009-5179-7535
Approval of the final version of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Jayamaliga Vijayananth
ORCID: 0009-0008-8683-6779
Approval of the final version of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. Tos P, Titolo P, Chirila NL, Catalano F, Artiaco S. Surgical treatment of acute fingernail injuries. J Orthop Traumatol. 2012;13(2):57-62.
2. Bharathi RR, Bajantri B. Nail bed injuries and deformities of nail. Indian J Plast Surg. 2011;44(2):197-202.
3. Pandhi D, Verma P. Nail avulsion: indications and methods (surgical nail avulsion). Indian J Dermatol Venereol Leprol 2012;78:299-308.
4. Karthi Sundar V. Surgical management of fingertip injuries. Int J Res Orthop. 2017;3(1):19-22.
5. Khodaee M, Kelley N, Newman S. Median nail dystrophy. CMAJ. 2020;192(50):E1810.
6. Pradhan S; Debopriya P; Shahid R. Trachyonychia in children: a comprehensive review with recent updates. Ind J Paed Dermatol. 2024;25(2):88-93.
7. Keel. Encyclopædia Britannica. Chicago: Encyclopædia Britannica. 1911.
8. Acuña Pinzon C, Nieves Condoy J, Rivera Marquez D A. Nail Cancer: Review of the two main types of an underestimated disease. Cureus. 2022;14(4):e23856.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}