


Ana Paula Dornelles Manzoni; Fabiane Kumagai Lorenzini; Taisa de Boni Gauer; Bruna Bonamigo Thomé; Renan Rangel Bonamigo
Funding: None
Conflict of interest: None
Submitted on: 05/12/2025
Final decision: 08/26/2025
How to cite this article: Manzoni APD, Lorenzini FK, Gauer TB, Thomé BB, Bonamigo RR. Non-surgical management of ectropion using hyaluronic acid gel with cannula injection. Surg Cosmet Dermatol. 2025;17:e20250470.
The treatment of eyelid ectropion remains challenging. Surgical approaches are more widely used, but techniques using hyaluronic acid have shown increasing promise. This article describes a novel technique for hyaluronic acid injection through a cannula to correct severe cicatricial ectropion secondary to lamellar ichthyosis. Despite the need for further studies, the procedure proved to be safe and easily reproducible.
Keywords: Ectropion; Hyaluronic Acid; Cannula
Ectropion is an eyelid malposition with exposure of the ocular surface. It primarily affects the lower eyelid and can lead to several ocular complications.1 In cicatricial ectropion (CE), contracture of the skin and subcutaneous tissue shortens the anterior lamella, resulting in eyelid eversion.2,3 When left untreated, ectropion may cause permanent corneal damage and potentially lead to blindness.4,5 Currently, in addition to surgical correction, there has been a trend toward minimally invasive approaches, such as the use of hyaluronic acid (HA) fillers.
The present case describes a patient with lamellar ichthyosis and bilateral ectropion, with one eye already affected by secondary corneal ulcer and amaurosis.6 In an attempt to improve the ectropion and prevent progression to complete blindness, HA was injected using a cannula. This novel technique has never been described in the literature before.
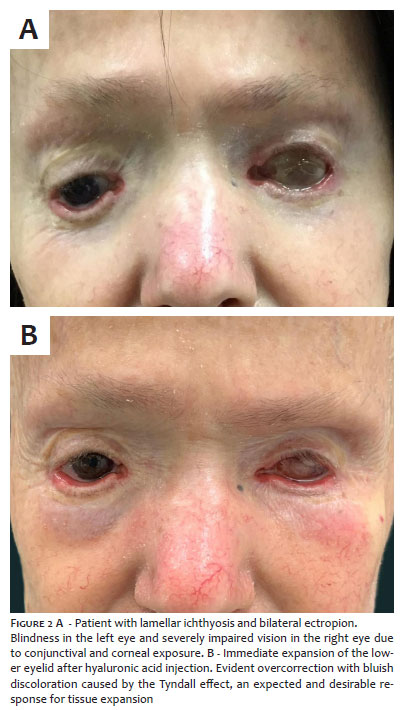
A 67-year-old woman had lamellar ichthyosis, bilateral ectropion, a left ocular prosthesis, and severely impaired vision in the right eye due to conjunctival and corneal exposure.
The goal was to use HA for tissue expansion to elevate the inferior tarsal border and facilitate eyelid closure, thereby minimizing ocular sequelae. For safety and to ensure a more homogeneous distribution of the acid, a cannula was preferred over a needle.
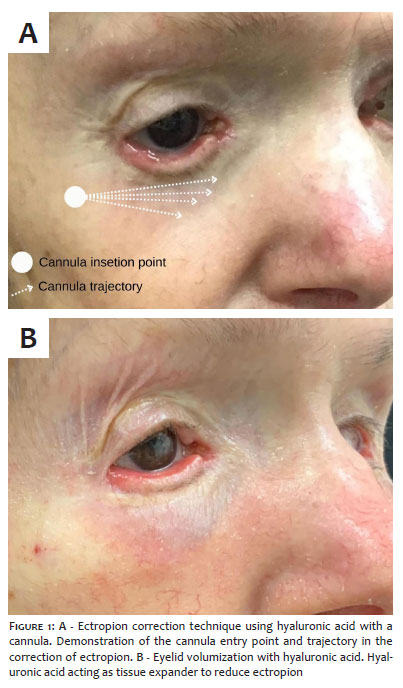
The procedure consisted of introducing a 22G rigid cannula into the plane between the skin and orbicularis oculi muscle, followed by retrograde injection of 1 mL of medium G prime HA filler (20 mg/mL) into the anterior lamella along the lower eyelid (Figure 1). The cannula advanced easily within the supramuscular plane, causing minimal discomfort, and no bleeding or ecchymosis was observed. Immediate expansion of the lower eyelid was evident, characterized as overcorrection with a bluish discoloration caused by the Tyndall effect—an expected and desirable response for achieving tissue expansion (Figure 2).
The primary goal of this procedure is not simply aesthetic improvement, but rather to prevent the progression of corneal ulcers secondary to ectropion. Therefore, intentional overcorrection is part of the therapeutic strategy. The patient has undergone annual HA injections using a cannula for 5 years, with no recurrence of corneal ulcers during follow-up.
Surgical correction remains the most common treatment for CE; however, HA injection techniques have proven to be a viable alternative, capable of expanding the anterior lamellar region, stimulating neocollagenesis, and improving eyelid apposition.1 Moreover, HA injection is minimally invasive and has a low complication risk.2 Patient satisfaction with aesthetic outcomes is similar to that of surgical correction.2,3
Potential complications of HA injection include hematoma, edema, uneven filler distribution, overcorrection, and vascular occlusion.4 The use of a 22G cannula reduces the risk of arterial and venous ischemia, particularly relevant given the vascular anatomy of the lower eyelid—a region at increased risk for ischemic complications.4 Cannulas require a single entry point, decreasing the likelihood of hematoma, ecchymosis, and discomfort.
The use of a cannula to correct CE with HA injections has proven to be a safe, simple, and effective technique. Nevertheless, further prospective comparative studies are required to validate its widespread application.
Ana Paula Dornelles Manzoni
ORCID: 0000-0001-6184-4440
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Fabiane Kumagai Lorenzini
ORCID: 0000-0001-6365-8705
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Taisa de Boni Gauer
ORCID: 0000-0002-7815-6107
Conception and design of the study.
Bruna Bonamigo Thomé
ORCID: 0000-0002-3445-9480
Conception and design of the study.
Renan Rangel Bonamigo
ORCID: 0000-0003-4792-8466
Critical review of the literature.
1. Mitchell DA, Lyons AB, Moy RL. Correction of cicatricial and involutional lower eyelid ectropion with hyaluronic acid. JAAD Case Rep. 2018;4:628-30.
2. Worley B, Huang JW, Macdonald J. Approach to treatment of cicatricial ectropion: a systematic review and meta-analysis comparing surgical and minimally invasive options. Arch Dermatol Res. 2020;312:165-72.
3. Enghelberg M, Michaelos L, Lonescu C, Stingu T, Georgescu D. Volumizing hyaluronic acid filler as a temporary tissue expander in lower eyelid cicatricial ectropion. Pan-Am J Ophthalmol. 2017;16:52–4.
4. Bravo BSF, Totti J, Gelpi BEA, Bianco de Souza S, Bravo LG. Use of hyaluronic acid fillers to correct scleral show: a review of technique. J Clin Aesthet Dermatol. 2018;11:38-40.
5. Veloso LK, Ferreira G, Marques JP, Meneghim RLF, Galindo AF, Padovani CR, Schellini SA. Short-term qualitative and quantitative analyses of preseptal injection of hyaluronic acid on the treatment of acquired lower eyelid cicatricial ectropion. Arq Bras Oftalmol. 2023;87(5):e20220245.
6. Byrd LB, Gurnani B, Martin N. Corneal Ulcer. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}