


Rogerio Nabor Kondo; Amanda Alencar dos Anjos; Karoline Rodrigues Crevelim; Marcos Vinicius Borges Martins
Funding: None
Conflict of interest: None
Submitted on: 03/22/2025
Final decision: 06/05/2025
How to cite this article: Kondo RN, Anjos AA, Crevelim KR, Martins MVB. Vermilionectomy: report of two cases comparing classical excision and W-plasty. Surg Cosmet Dermatol. 2025;17:e20250454.
Vermilionectomy is a surgical procedure for the partial or total removal of the vermilion border, used primarily for the treatment of actinic cheilitis. W-plasty has been considered superior to classic elliptical excision because it avoids linear scars and, therefore, lip retractions. However, the classic elliptical excision is still widely used. This article reports two cases treated with both techniques that achieved similar satisfactory aesthetic results.
Keywords: Keratosis, Actinic; Lip; Surgery, Oral
Actinic cheilitis (AC) is a premalignant lesion resulting from chronic sun exposure that affects the vermilion of the lower lip, characterized by erythema, atrophy, hyperkeratosis, and erosions.1 In treatment, it is essential to minimize the risk of malignant transformation while preserving local function and aesthetics.
Nonsurgical therapeutic options for AC include topical imiquimod, chemical cauterization with trichloroacetic acid (TCA), photodynamic therapy, topical diclofenac, and laser treatments, with variable efficacy.2
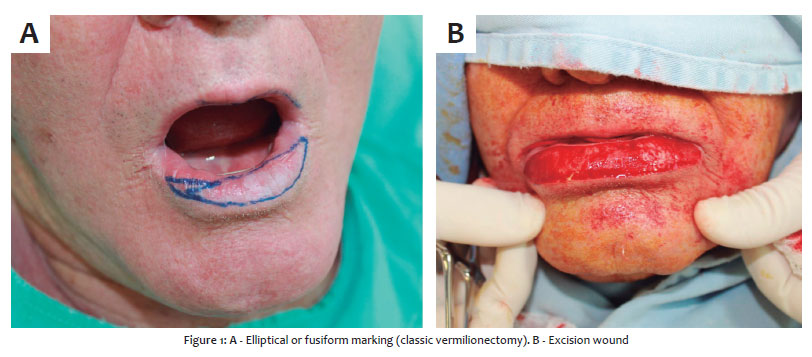
If clinical treatment of AC fails, one surgical option is vermilionectomy, which consists of partial or total removal of the lip vermilion. In the classic form of the procedure, the excision is elliptical or fusiform (spindle-shaped).3 In the W-plasty variant, the excision has a jagged outline.4
Some authors consider W-plasty superior to the classic technique because it avoids a linear scar and therefore lip retraction.4 However, the classic elliptical or fusiform excision remains widely used because it is technically easier to perform.3
This article reports two cases using both techniques (classic and W-plasty), with satisfactory aesthetic and functional outcomes and no recurrence of AC after 4 years of follow-up.
Two patients with AC underwent two sessions of 70% TCA without improvement and were subsequently selected for vermilionectomy. Both techniques were used, the classic approach and W-plasty. Histopathological examinations of the incisional and later excisional biopsies confirmed AC.
Patient 1: male, 69 years old, white, nonsmoker, presenting a scaly plaque with severe keratosis, erythema, and atrophy involving almost the entire lower lip (Figure 1).
• Patient in horizontal supine position;
• Preoperative marking with surgical pen in fusiform outline (Figure 1A);
• Antisepsis with topical 10% polyvinyl iodine;
• Placement of surgical drapes;
• Infiltrative anesthesia with 2% lidocaine and vasoconstrictor;
• Incision with no. 15 blade following the preoperative markings. En bloc resection of lesion down to the muscle layer;
• Hemostasis;
• Suturing with 5-0 polyglactin with simple stitches (Figure 2A);
• Cleaning with saline solution.
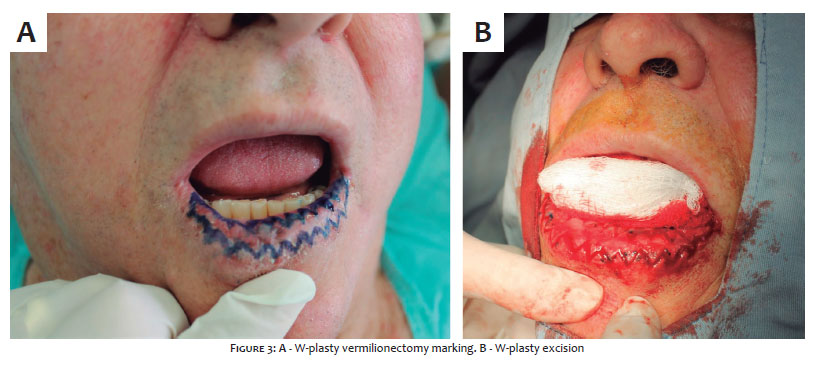
Patient 2: male, 73 years old, white, nonsmoker, presenting a scaly plaque with severe keratosis, erythema, atrophy, and ulcerated areas involving almost the entire lower lip (Figure 3).
• Patient in horizontal supine position;
• Preoperative marking with surgical pen in jagged outline, with “broken lines” (Figure 3A);
• Antisepsis with topical 10% polyvinyl iodine;
• Placement of surgical drapes;
• Infiltrative anesthesia with 2% lidocaine and vasoconstrictor;
• Incision with no. 15 blade following the preoperative markings. En bloc resection of lesion down to the muscle layer;
• Hemostasis;
• Suturing with 5-0 polyglactin with simple stitches (Figure 2A);
• Cleaning with saline solution.
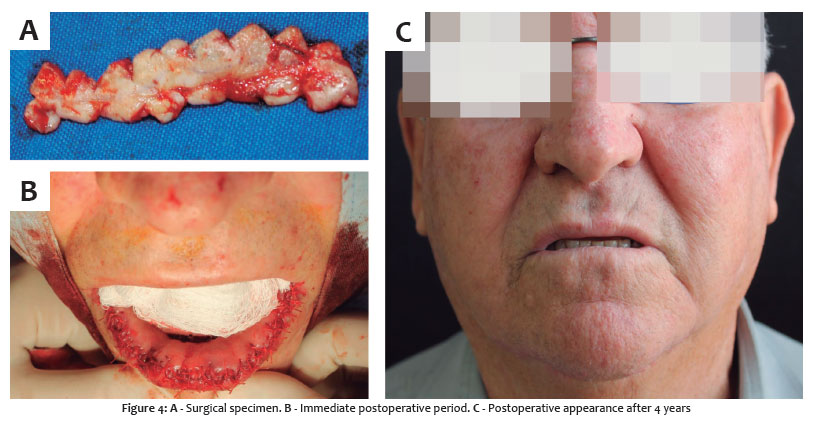
The patients had no intercurrences in the first postoperative days. There was good healing and satisfactory aesthetic outcomes in the late postoperative period (Figures 2B and 4C).
Resolution of AC is important to prevent malignant transformation, regardless of the method used. However, when choosing vermilionectomy as the surgical technique, it is essential to avoid complications such as retraction, commissure deviation, microstomia, and hypochromia.1-4
In 1956, Kwapis and Gibson described vermilionectomy as the partial or total excision of the lip vermilion, with mucosal advancement and its suture to the skin for closure of the defect.4 Elliptical or fusiform excision came to be known as the classic method (Figure 1A). In this technique, the scar is linear, increasing the risk of retraction.3,4
In 1989, Vozmediano described vermilionectomy using W-plasty.4 In this method, the excision has a jagged or serrated outline, and the resulting scar forms a broken line that distributes tension more evenly, reducing suture tension and lowering the likelihood of retraction (Figures 3A and 4B).
In 2011, Rossoe et al. compared 32 patients treated with the two vermilionectomy techniques (classic vs. W-plasty, 15 and 17 patients, respectively). In that study, W-plasty provided better aesthetic results.4
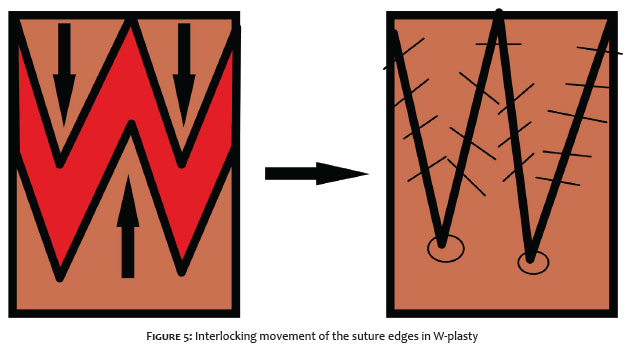
The advantage of the classic technique is that it is easier to perform. Primary linear closure reduces procedure time. In contrast, W-plasty requires interlocking the pointed projections with the corresponding recesses, which demands additional adjustments and extends the surgical time (Figure 5).3,4
The results of these techniques may depend on several factors, including age, comorbidities, smoking, postoperative care, and surgeon experience. It is important that dermatologic surgeons master both techniques so that they can be applied according to the needs of individual cases.4
In the two cases presented in this report, after 4 years of follow-up, similar results were observed, with no retraction, dyschromia, commissure deviation, or microstomia.
Both vermilionectomy techniques, the classic method and W-plasty, can provide similar aesthetic and functional results in the treatment of AC.
Rogerio Nabor Kondo
ORCID: 0000-0003-1848-3314
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Amanda Alencar dos Anjos
ORCID: 0000-0002-5819-7315
Approval of the final version of the manuscript, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Critical review of the literature, Critical revision of the manuscript.
Karoline Rodrigues Crevelim
ORCID: 0009-0006-6141-2633
Approval of the final version of the manuscript, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
Marcos Vinicius Borges Martins
ORCID: 0009-0003-2433-5083
Approval of the final version of the manuscript, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
REFERENCES:
1. Baltazar IL, Ferreira FR, Nascimento LFC, Mandelbaum SH. Tratamento da queilite actínica com terapia fotodinâmica com a luz do dia - avaliação clínica e histopatológica. Surg Cosmet Dermatol. 2019;11(4):295-8.
2. Lai M, Pampena R, Cornacchia L, Pellacani G, Peris K, Longo C. Treatments of actinic cheilitis: a systematic review of the literature. J Am Acad Dermatol. 2020;83(3):876-87.
3. Chang SH, Huang ZS, Chen WL, Zhou B, Zhong JL. Vermilionectomy followed by reconstruction of the vermilion mucosa using allograft dermal matrix in patients with actinic cheilitis of the lower lip. J Cosmet Dermatol. 2021;20(1):263-6.
4. Rossoe EW, Tebcherani AJ, Sittart JA, Pires MC. Actinic cheilitis: aesthetic and functional comparative evaluation of vermilionectomy using the classic and W- plasty techniques. An Bras Dermatol. 2011;86(1):65-73.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}