


Nivin Mazen Said1; Denise Lima Sousa1; Airton Kenji Motizuki2; Emanuella Rosyane Duarte Cerqueira1; Franklin Sousa Rocha1
Funding: None
Conflict of interest: None
Submitted on: 03/04/2025
Final decision: 08/26/2025
How to cite this article: Said NM, Sousa DL, Motizuki AK, Cerqueira ERD, Rocha FS. Lipofilling in a patient with Parry-Romberg syndrome: from diagnosis to treatment. Surg Cosmet Dermatol. 2025;17:e20250447.
Parry-Romberg syndrome is a rare condition characterized by progressive unilateral facial atrophy, involving the skin, muscles, fat, and bones. Treatment aims to restore facial symmetry, with autologous fat grafting an effective option. This report describes the case of a 25-year-old woman who underwent three sessions of Coleman-type fat grafting using autologous abdominal fat. The procedure improved facial aesthetics and quality of life, with high patient satisfaction. Despite partial and unpredictable resorption of fat over the course of follow-up, this technique remains a viable alternative for correcting facial deformities.
Keywords: Transplantation, autologous; Facial Hemiatrophy; Abdominal Fat
Parry-Romberg syndrome, also known as Progressive Hemifacial Atrophy, is a rare dermatological condition characterized by progressive and asymmetric atrophy of the skin and underlying tissues on one side of the face.1,2 First described by Perry in 1825 and later detailed by Romberg in 1846, the syndrome primarily affects children and adolescents, with no predominance of either sex. In general, it begins in the first or second decade of life, progresses over a period of 2 to 20 years, and then becomes inactive.2,3
It is characterized by craniofacial atrophy that may affect part or all structures of the face, including skin, muscle, fat, bone tissue, the trigeminal nerve, and even brain parenchyma. These alterations often result in three-dimensional asymmetries associated with severe functional and psychological complications.2
Generally, treatment for the syndrome aims at improving facial aesthetics. There are various approaches for correcting facial defects, including autologous fat grafting, orthognathic surgery, local flaps, and solid or liquid silicone implants. In Brazil, the use of silicone implants for this syndrome is neither recommended nor authorized, given the availability of more effective treatments such as lipofilling.1,3 Moreover, there are reports in the literature regarding the limited effectiveness of heterologous fillers in patients with Parry-Romberg syndrome due to the higher risk of vascular, infectious, and inflammatory adverse events. Their use is only recommended in cases where autologous fat grafting do not yield unsatisfactory or long-lasting results.4 Adipose tissue is the most widely used option because it is fully biocompatible, abundant in the body, compatible with surrounding tissues, and capable of restoring deformed facial structures, thereby restoring three-dimensional appearance.1
This case report describes the use of lipofilling in the treatment of a 25-year-old woman diagnosed with Parry-Romberg syndrome. The report is supported by a literature review conducted in the PubMed and Scientific Electronic Library Online (SciELO) databases. In addition, the study followed the CARE checklist guidelines for case reports and case series.
The case was based on the patient’s medical records and complementary examinations, which helped guide her clinical and therapeutic follow-up. Data collection was conducted in February 2025, in accordance with all ethical principles, and was performed after obtaining the patient’s informed consent.
A 25-year-old woman from Marabá, state of Pará, and residing in Belém had been treated at the dermatology outpatient department since September 2018 after being diagnosed with Parry-Romberg syndrome with right hemifacial atrophy. She reported frequent headaches and a “sinking” sensation in the right parietal region.
Dermatological examination revealed a hypochromic atrophic plaque with areas of bony depression in the right parietal region, atrophy of the right mandibular area and chin, and a sclerotic brownish plaque in the right cervical region.
A cranial magnetic resonance imaging (MRI) scan performed in June 2021 showed the following findings: thinning and irregularity of the right frontotemporal skin and subcutaneous tissue, with apparent thinning of the frontal calvarium; normal cerebral parenchyma, as well as normal sulci, fissures, and other internal structures; normal flow in the major vertebrobasilar and carotid arteries; and a midline that remained centered.
In September 2021, the patient presented with active disease, and treatment with methotrexate 10 mg/week and folic acid 5 mg/week was initiated, along with follow-up by an ophthalmologist, a neurologist, and a dentist. She achieved clinical stability and disease inactivity by November 2021, with improvement of headaches, and was subsequently referred to a plastic surgeon for evaluation of surgical treatment.
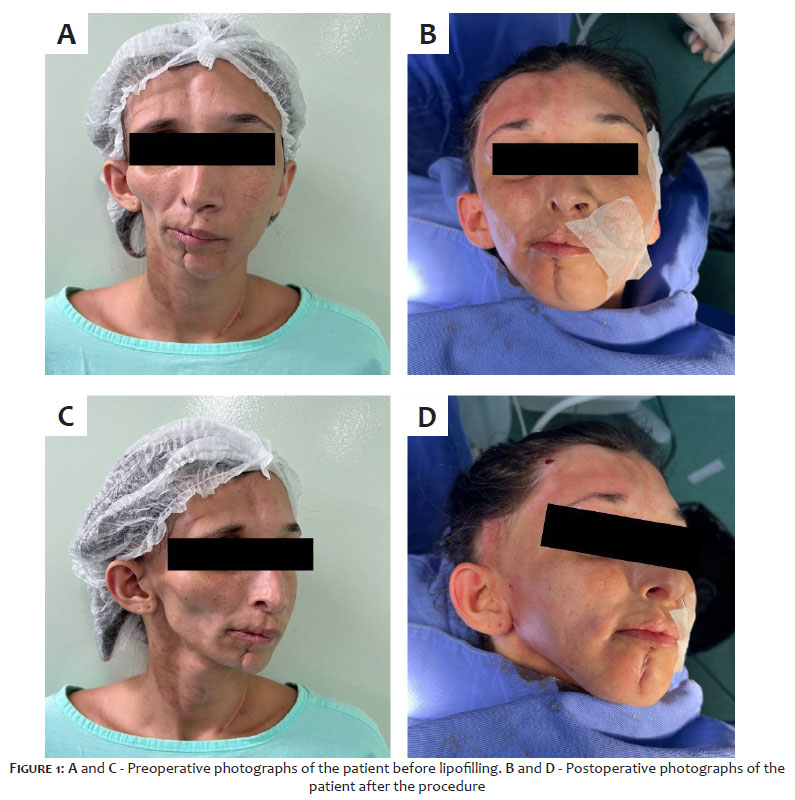
The patient underwent lipofilling using the Coleman technique, with abdominal fat harvesting performed under general anesthesia. For the surgical procedure, a 2-3 mm cannula connected to a 10-mL syringe with manual suction (negative pressure) was used to obtain 30 mL of adipose tissue from the abdomen. The harvested material was prepared by fat decantation and washing to remove blood and other components. After adequate preparation, the fat was transferred to 1-mL syringes and injected into the affected facial areas. All harvested material was used for the grafting. Three surgical procedures were performed, approximately one year apart, using the same technique in all procedures and injecting 30 mL of fat per session (Figure 1).
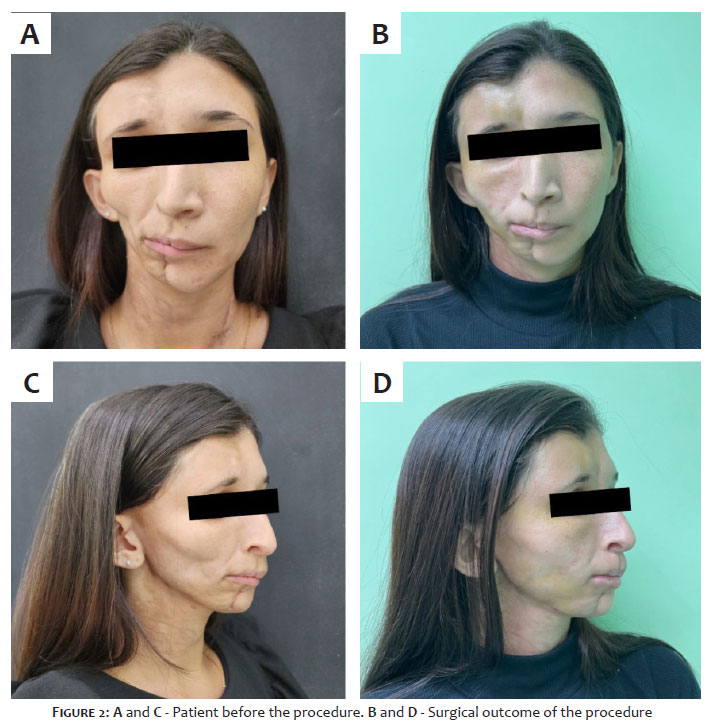
Surgical outcomes were assessed by comparing preoperative photographs with images obtained five months after the third procedure, as well as by the patient’s self-evaluation, who reported satisfaction with the results (Figure 2).
Parry-Romberg syndrome has an unknown etiology, although genetic, autoimmune, and environmental factors are believed to contribute to its development. The severity of the condition is classified according to the extent of atrophy of the skin, subcutaneous tissue, bone tissue, and involvement of the branches of the trigeminal nerve.3,2
Because the condition manifests as three-dimensional craniofacial deformities, complete restoration of facial symmetry is often difficult.2 In general, treatment aims at improving facial function and aesthetics.3 In such cases, once clinical inactivity of the disease is observed, reconstructive surgical treatments should be considered.2
Autologous grafts are preferred for replacing tissue lost due to atrophy due to their lower risk of tissue rejection, leading, therefore, to less local and systemic inflammatory response that could otherwise lead to graft loss. Because adipose tissue is moldable, readily available, and easy to harvest, lipofilling is the most frequently used technique.1
Structured lipofilling in Parry-Romberg syndrome provides a simple, reproducible method with satisfactory results that contribute to treatment success, with low morbidity and the possibility of additional interventions for further corrections.5 Coleman6,7 and other authors8,9,10 hypothesize that structural fat transplantation presents both advantages and disadvantages for correcting soft-tissue defects, such as low graft-survival rates due to early resorption, probably because of the lack of a well-vascularized graft bed. In addition, various methods have been proposed to increase fat-graft survival, but there are no definitive treatment protocols for clinical practice, and long-term maintenance of grafts is required because of the unpredictable resorption of fat by the body.9
Robby et al. systematically described the predominance of the Coleman technique in lipofilling and that the abdomen is the most common donor site used in surgical procedures for Parry-Romberg syndrome. The authors argue that this technique, associated with choosing the abdomen as the donor site, offers a minimally invasive approach capable of achieving aesthetic results with lower risk and fewer complications, and provides more advantages to the patient compared with flap techniques.11
Moreover, it has been documented that the main complication of this procedure is early fat resorption. The aesthetic benefits include improved skin quality and more natural facial contours and expressions, which corroborates the postoperative outcomes described in this case report and the patient’s high level of satisfaction.11
In conclusion, autologous fat grafting can mitigate severe anatomical impairment in patients affected by Parry-Romberg syndrome, in addition to showing a high degree of effectiveness and aesthetic satisfaction, as measured by the patient’s self-assessment. l
Nivin Mazen Said
ORCID: 0000-0002-0611-5672
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Denise Lima Sousa
ORCID: 0009-0004-8632-8230
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Airton Kenji Motizuki
ORCID: 0009-0002-7188-0984
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
Emanuella Rosyane Duarte Cerqueira
ORCID: 0009-0004-9545-8125
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Franklin Sousa Rocha
ORCID: 0000-0002-7386-1616
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. Alencar JCG, Andrade SHC, Pessoa SGP, Dias IS. Lipoenxertia autóloga no tratamento da atrofia hemifacial progressiva (síndrome de Parry-Romberg): relato de caso e revisão da literatura. An Bras Dermatol. 2011;86(4 suppl 1):85-8.
2. Amaral CER, Denadai R, Buzzo CL, Amaral CAR. Abordagem terapêutica da síndrome de Parry-Romberg baseada em um sistema de classificação de gravidade. Rev Bras Cir Plást. 2014;29(1):57-65.
3. Leite LA, Oliveira Júnior CJLA, Souza IFL, Angelim CL, Lins MEE, Bivar GCC, et al. Síndrome de Parry-Romberg: avaliação clínica e cirúrgica no tratamento da atrofia hemifacial progressiva. Rev Contemp. 2024;4(6):e4830.
4. Vasconcelos‐Berg R, Varella Maire B, Navarini AA. Treating Parry‐Romberg syndrome with hyaluronic acid: insights after 2.5 years of successive treatments. An Bras Dermatol. 2025;100(3):606–8.
5. Cedrola JPV, Castro CC, Aboudib JH, Turini T, Castro M, Serra F, et al. Análise do tratamento da Síndrome de Parry-Romberg por lipoenxertia estruturada no Hospital Universitário Pedro Ernesto-HUPE-UERJ. Rev Bras Cir Plást. 2011;26(3 Suppl.1):28.
6. Coleman SR. Facial recontouring with lipostructure. Clin Plast Surg. 1997;24(2):347-67.
7. Coleman SR. Structural fat grafts: the ideal filler? Clin Plast Surg. 2001;28(1):111-9.
8. Guerrerosantos J. Long-term outcome of autologous fat transplantation in aesthetic facial recontouring: sixteen years of experience with 1936 cases. Clin Plast Surg. 2000;27(4):515-43.
9. Chang Q, Li J, Dong Z, Liu L, Lu F. Quantitative volumetric analysis of progressive hemifacial atrophy corrected using stromal vascular fraction-supplemented autologous fat grafts. Dermatol Surg. 2013;39(10):1465-73.
10. Arif T, Fatima R, Sami M. Parry-Romberg syndrome: a mini review. Acta Dermatovenerol Alp Pannonica Adriat. 2020;29(4):193-9.
11. Rodby KA, Kaptein YE, Roring J, Jacobs RJ, Kang V, Quinn KP, et al. Evaluating autologous lipofilling for Parry-Romberg syndrome-associated defects: a systematic literature review and case report. Cleft Palate Craniofac J. 2016;53(3):339-50.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}