


Sunil Kumar Gupta
Funding: None
Conflict of interest: None
Submitted on: 02/15/2025
Final decision: 05/04/2025
How to cite this article: Gupta SK. Localized tenosynovial giant cell tumor of the left index finger – a case report. Surg Cosmet Dermatol. 2025;17:e20250440.
Tenosynovial giant cell tumors (TGCTs) are rare, benign neoplasms of the tendon sheaths, usually affecting the hands. In this case report, a 52-year-old female presented with a painless enlarging mass on the left index finger. Histopathological examination revealed a nodular lesion with foamy histiocytes, multinucleated giant cells, and lymphocytes. Surgical excision led to full recovery with no recurrence. This case emphasizes the importance of considering TGCTs in differential diagnosis of finger masses and highlights surgical excision as an effective treatment.
Keywords: Soft Tissue Neoplasms; Giant Cell Tumors; Hand; Surgical Procedures
Tenosynovial giant cell tumors (TGCTs) are rare, locally aggressive but typically benign neoplasms of the joints, bursae, and tendon sheaths.1,2 TGCTs can affect all age groups but are more common in younger individuals and in females. They primarily present with pain, swelling, and stiffness. According to the 2013 World Health Organization reclassification, the term “localized TGCT” includes giant cell tumors of the tendon sheath and nodular tenosynovitis, whereas “diffuse TGCT” includes diffuse-type giant cell tumors and pigmented villonodular synovitis.1,2
A 52-year-old woman presented to the Dermatology outpatient service with discomfort in her left index finger and an enlarging mass for 3 years. On physical examination, there was a tender nodule 2 × 2 cm on size at the volar aspect of the left index finger involving the distal phalanx (Figure 1). The nodule was ill-defined from the surrounding tissue and not associated with paresthesia. Movement of the distal interphalangeal joint was mildly restricted. The patient had no history of smoking or alcohol abuse. Family history was also not relevant. X-ray imaging showed a soft-tissue mass without bone erosion (Figure 2).
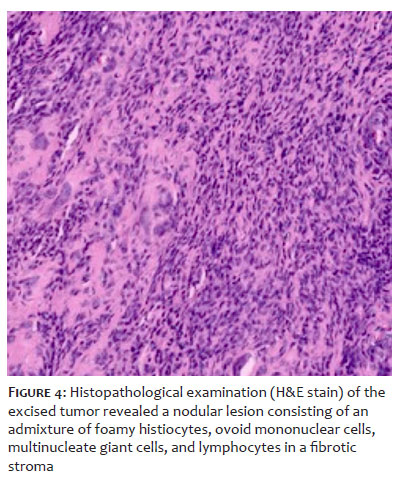
After discussing treatment options with the patient, surgical excision was planned. A linear incision was made over the mass under 2% lidocaine infiltration. The tumor was clearly exposed on the volar aspect of the left index finger up to the distal phalanx and completely excised (Figure 3). Primary closure of the surgical wound was performed. Histopathological examination of the excised tumor revealed a nodular lesion consisting of an admixture of foamy histiocytes, ovoid mononuclear cells, multinucleate giant cells, and lymphocytes in a fibrotic stroma. Numerous vessels of varying calibers were present. Scattered hemosiderin deposition was noted. Mitotic activity was readily observed (Figure 4).
Postoperative follow-up was performed one month after the procedure. The patient made a full recovery without movement restriction or substantial swelling (Figure 5). Flexion at the distal interphalangeal joint of the left index finger was normal. No clinical or radiologic signs of recurrence were observed at follow-up 3 months after the excision.
TGCTs are the second most common soft tissue tumor of the hand after ganglion cysts, with an incidence of 1.8 per million individuals per year and a prevalence of 8%-19% in hand joints.3 TGCTs primarily affect individuals aged 30 to 50 years, and are more frequent in females (M:F = 1:1.5).1,4
The WHO classification divides TGCTs into localized TGCT (L-TGCT) and diffuse TGCT (D-TGCT). L-TGCT is characterized as a well-circumscribed nodular lesion, most frequently affecting small joints. D-TGCTs present as an infiltrative and aggressive variant associated with a high rate of recurrence and joint destruction.4
TGCTs are driven by a translocation of the CSF1 gene on chromosome 1p13, leading to overexpression of colony-stimulating factor 1 (CSF1), which promotes neoplastic proliferation and recruitment of inflammatory monocytes via CSF1R activation.5 This process results in the accumulation of histiocyte-like cells, giant cells, hemosiderin-laden macrophages, and synovial fibrosis.5 Genomic studies have identified additional mutations contributing to TGCT pathogenesis, including the CSF1-COL6A3 fusion gene, implicated in tumor progression, and STAT6 alterations, potentially modulating tumor growth and immune evasion.6,7
Magnetic resonance imaging (MRI) remains the gold standard for diagnosing TGCT. L-TGCT appears as a well-defined, lobulated mass, whereas D-TGCT shows infiltrative, diffuse growth with hemosiderin deposition, leading to blooming artifacts on gradient-echo sequences.8 Emerging imaging techniques for TGCT diagnosis and monitoring include diffusion-weighted MRI (DWI-MRI) to assess tumor cellularity and response to systemic therapy and 18F-FDG PET-CT to differentiate active disease from fibrosis in recurrent TGCT.
Histologically, TGCTs consist of mononuclear histiocyte-like cells expressing CSF1, CD163, and CD68; multinucleated giant cells; hemosiderin-laden macrophages; and foamy macrophages, along with chronic inflammatory infiltrates.2,3 High mitotic activity and focal necrosis are observed in aggressive or recurrent cases.
Recent advances in biomarker research suggest that soluble CSF1 levels in plasma may serve as a diagnostic and prognostic marker, correlating with tumor burden and response to CSF1R inhibitors.9
Surgical excision remains the first-line treatment for L-TGCT, with a 9% recurrence rate, whereas D-TGCT has a recurrence rate of up to 23% due to incomplete resection and infiltrative growth.10
Recent studies support arthroscopic synovectomy for intra-articular L-TGCT, as it reduces the risk of recurrence. Open resection for D-TGCT often requires multiple interventions.
Given the high recurrence rate and surgical morbidity associated with D-TGCT, recent therapeutic advances have focused on targeting the CSF1/CSF1R pathway. Pexidartinib (PLX3397), a tyrosine kinase inhibitor (TKI) that selectively inhibits CSF1R, was approved by the U.S. FDA in 2019 for unresectable TGCT .11 Emactuzumab, a monoclonal antibody targeting CSF1R, has shown promising results and fewer hepatic adverse effects compared with pexidartinib.10 Vimseltinib, a next-generation CSF1R inhibitor currently in Phase 2 trials, has demonstrated higher efficacy and improved safety profiles.12
This case underscores the importance of early diagnosis and complete surgical excision in L-TGCTs while recognizing the therapeutic challenges posed by D-TGCTs due to its infiltrative nature and high recurrence rates. The advent of CSF1R inhibitors, immune checkpoint blockade, and gene therapy offers new hope for the management of advanced TGCTs, highlighting the need for a multidisciplinary approach that integrates surgery, targeted treatment, and personalized strategies.
Sunil Kumar Gupta
ORCID: 0000-0001-9033-4394
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. de Saint Aubain Somerhausen N, van de Rijn M. Tenosynovial giant cell tumour, localized type. In: Fletcher CDM, Bridge JA, Hogendoorn P, Mertens F. WHO Classification of Tumours of Soft Tissue and Bone, ed 4; Lyon, France: International Agency for Research on Cancer (IARC); 2013. P. 100-1.
2. Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: current treatment concepts and future perspectives. Eur J Cancer 2016;63:34-40.
3. Mastboom MJL, Verspoor FGM, Verschoor AJ, Uittenbogaard D, Nemeth B, Mastboom WJB, et al. Higher incidence rates than previously known in tenosynovial giant cell tumors. Acta Orthop. 2017;88(6):688-94.
4. Somerhausen ND, van de Rijn M. Tenosynovial giant cell tumor. In: WHO classification of tumors editorial board, editor. 5th World Health Organization classification of tumors of soft tissue and bone.
5. West RB, Rubin BP, Miller MA, Subramanian S, Kaygusuz G, Montgomery K, et al. A landscape effect in tenosynovial giant-cell tumor from activation of CSF1 expression by a translocation in a minority of tumor cells. Proceedings of the National Academy of Sciences. 2006;17;103(3):690-5.
6. Tap WD, Gelderblom H, Palmerini E, Desai J, Bauer S, Blay JY, et al. Pexidartinib versus placebo for advanced tenosynovial giant cell tumour (ENLIVEN): a randomised phase 3 trial. The Lancet. 2019;394(10197):478-87.
7. Ricketts TD, Prieto-Dominguez N, Gowda PS, Ubil E. Mechanisms of macrophage plasticity in the tumor environment: manipulating activation state to improve outcomes. Frontiers in immunology. 2021;12:642285.
8. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis: radiologic-pathologic correlation. Radiographics. 2008;28(5):1493-518.
9. Cassier PA, Italiano A, Gomez-Roca C, Le Tourneau C, Toulmonde M, D'Angelo SP, et al. Long-term clinical activity, safety and patient-reported quality of life for emactuzumab- treated patients with diffuse-type tenosynovial giant-cell tumour. Eur J Cancer. 2020;141:162-70.
10. Siegel M, Bode L, Südkamp N, Kühle J, Zwingmann J, Schmal H, et al. Treatment, recurrence rates and follow-up of Tenosynovial Giant Cell Tumor (TGCT) of the foot and ankle-A systematic review and meta-analysis. PLoS One. 2021;16(12):e0260795.
11. Tap WD, Singh AS, Anthony SP, Sterba M, Zhang C, Healey JH, et al. Results from phase I extension study assessing pexidartinib treatment in six cohorts with solid tumors including TGCT, and abnormal CSF1 transcripts in TGCT. Clin Cancer Res. 2022;28(2):298-307.
12. Blay JY, Gelderblom H, Rutkowski P, Wagner A, van de Sande M, Gonzalez AF, et al. 1509P Efficacy and safety of vimseltinib in tenosynovial giant cell tumour (TGCT): Phase II expansion. Ann Oncol. 2022;33:S1236-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}