


Luiz Roberto Dal Bem Pires Júnior1; Fernanda Nomoto Fujii1; Rafaella Castilho1; Waleska Ramos Alvim Lescowicz1; Rodolfo Barros Leite1; Anna Victoria Valiente Engelhorn2
Funding: None.
Conflict of interest: None.
Submitted on: 11/04/2024
Final decision: 02/13/2025
How to cite this article: Pires Júnior LRDB, Fujii FN, Castilho R, Lescowicz WRA, Leite RB, Engelhorn AVV. Bilateral lobuloplasty with inverted "snail" technique for correction of lobes deformed by prolonged use of gauges. Surg Cosmet Dermatol. 2025;17:e20250418.
Earlobe stretching dates back to various ancient cultures, symbolizing social status, cultural identity, and spirituality. Since the 1970s, it has gained popularity in the West as a form of self-expression. However, the use of gauges can lead to deformities requiring surgical correction. Numerous techniques have been developed over the past century to address this issue. This case report describes the use of the inverted "snail" technique, which employs two flaps, folding the medial flap into a spiral, and allows for a harmonious and symmetrical adjustment. It can be a viable alternative for correcting extensive deformities and asymmetries.
Keywords: Body modification, non-therapeutic; Ear deformities, acquired; Esthetics; Plastic surgery procedures.
Earlobe stretching dates back to various ancient cultures. In Ancient Egypt, for instance, Pharaoh Tutankhamun wore ear gauges, a common practice among elites symbolizing status and power.1 In Africa, tribes such as the Maasai in Kenya and the Mursi in Ethiopia practice earlobe stretching to this day, with gauge size associated with age, wisdom, and how respected an individual is in their community. Earlobe stretching also has spiritual significance among some tribes in South America and indigenous peoples of Asia, who believe the practice opens "gateways" or "connections" with the spirit world.2 In the modern Western world, gauges rose in popularity in the 1970s and 1980s as part of counterculture movements, and became consolidated as a form of self-expression associated with alternative groups and subcultures during the 1990s and 2000s. Earlobe stretching came to be seen as a form of body modification connected to individuality and self-expression, untethered from tradition and part of the modern urban context.3 Although gauges have historically been used in many cultures to symbolize social status, cultural identity, and spirituality, prolonged use can cause earlobe deformities, which may in turn require surgical correction. The search for approaches that ensure aesthetic and functional results while preserving natural earlobe anatomy and promoting discreet scars has encouraged the development of new repair techniques. In this case report, we describe the use of the inverted "snail" technique for the reconstruction of bilateral earlobes deformed by prolonged use of gauges. It differs from the technique as previously described in terms of the transection site of the enlarged branch of the lobe.4
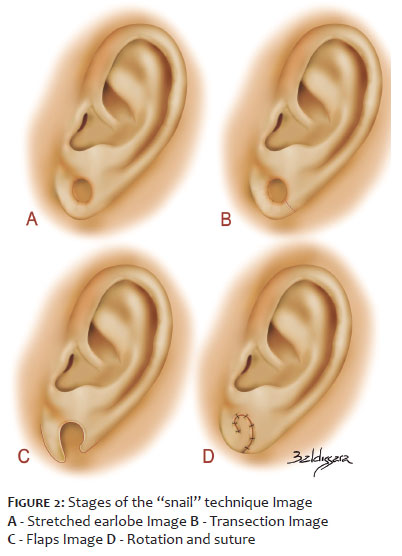
The patient, a 29-year old male with no comorbidities, sought specialized care in order to correct deformities in both earlobes caused by prolonged use of gauges, with gradual increase in size since adolescence. Clinical presentation included earlobes with large-diameter orifices and irregular margins, as well as bilateral asymmetry, making repair an aesthetic challenge (Figure 1). After careful assessment, bilateral lobuloplasty using the innovative inverted "snail" technique was indicated. The technique was chosen due to its capacity to recreate the natural contour of the earlobe, minimizing visible scars and restoring symmetry. In an outpatient setting, the procedure began with marking the skin around the circumference of the stretched branch of the earlobe (Figure 2A), with specific points on the medial and lateral regions. After asepsis and antisepsis, local infiltration using a modified Klein solution was performed, providing adequate anesthesia and vasoconstriction. Next, the stretched branch was sectioned at its lateral portion (Figure 2B), resulting in a longer medial flap and a shorter lateral flap (Figure 2C). To ensure harmonization of the new earlobes, scarification was carried out on the inner surface of the whole lateral flap and on the outer surface of the medial flap, preserving part of the outer surface of the lateral flap to form the lower border of the new lobe. The medial flap was then folded over its own axis, taking on a spiral shape—the "snail"—and joined to the raw areas of both flaps. Stabilization was achieved with simple stitches using 4-0 Vicryl sutures between the scarified areas, followed by a continuous 5-0 nylon suture along the entire length for skin closure (Figure 2D). In the postoperative period, the patient progressed favorably, with no complications, pain, or signs of infection (Figure 3). Proper healing was observed, along with a satisfactory aesthetic outcome, featuring symmetrical earlobes and a harmonious contour, in contrast to the asymmetries and deformities observed previously (Figure 4).
Earlobe deformity caused by prolonged ear gauge use has driven the search for surgical techniques that enable effective aesthetic and functional repair, given that individuals with earlobe defects caused by piercings are more likely to suffer negative image effects.5 Repairing these deformities demands special care due to the anatomic complexity and aesthetic requirements involved, including preserving the natural contour of the earlobe and minimizing visible scarring. Given existing surgical options, the technique chosen is generally that which makes the lobe more similar to the original, with a rounded shape and no notches or level differences.6,7 Throughout history, several techniques have been developed, from Miller's simple wedge excision in 1925 to more complex techniques, such as Hamilton and La Rossa's Z-plasty in 1975. The evolution in lobuloplasty techniques reflects the ongoing effort to improve both aesthetic and functional outcomes for patients.6,8 Techniques such as Pardue's, which aims to preserve the lobe orifice, may lead to level differences in the lower border,8 while methods such as Kalimuthu's "V"-shaped flap and Fatah and Fearon's "L"-shaped flap do not preserve the lobe orifice.9-11 Despite these variations, the satisfaction rate for lobuloplasty outcomes is approximately 92% to 100%,12,13 and the rate of postoperative complications is low, ranging from 0% to 33.3%. Reported complications include hypertrophic, depressed, or wide scars, recurrence of clefts, and surgical wound infections.14,15 In the present case, the "snail" technique proved effective by folding the medial flap into a spiral to form the new earlobe margin, enabling the lobe to regain a harmonious and symmetrical contour. The creation of flaps of different sizes, with selective scarification, contributes to a more precise fit between the medial and lateral flaps. The procedure enables the correction of asymmetries, preserves vascularization, ensures a smooth contour, and promotes healing without excessive tension, minimizing the formation of unsightly scars. This makes the technique an alternative for patients with significant deformities caused by prolonged use of large-diameter gauges. This case report contributes to the literature by introducing a technique that provides an aesthetically adequate outcome, widening treatment options to correct extensive deformities with high aesthetic demand.
Luiz Roberto Dal Bem Pires Júnior
ORCID: 0009-0001-6728-420X
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Fernanda Nomoto Fujii
ORCID: 0000-0001-5421-5865
Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied
Rafaella Castilho
ORCID: 0009-0003-1437-2024
Critical revision of the manuscript
Waleska Ramos Alvim Lescowicz
ORCID: 0000-0002-0106-1097
Critical revision of the manuscript
Rodolfo Barros Leite
ORCID: 0009-0008-0854-3030
Critical revision of the manuscript
Anna Victoria Valiente Engelhorn
ORCID: 0000-0002-9427-6459
Critical review of the literature, Critical revision of the manuscript
1. Tarlow S, Stutz LN, editors. The Oxford handbook of the archaeology of death and burial. Oxford: Oxford University Press; 2013.
2. Krutak L. Spiritual skin: magical tattoos and scarification. Edition Reuss; 2012.
3. Pitts V. In the flesh: the cultural politics of body modification. New York: Palgrave Macmillan; 2003.
4. Loureiro RS, Caropreso CA, Barboza Junior LCM, Ciancio IHL, Silva JLR, Sin SY. Snail Technique: Correção de Lóbulo Pós-Alargador.
5. Fung N, Hallock G, Kuzon W, Munshi J, Morrison C, Zins J, et al. Stretched earlobe piercings negatively impact casual observer perceptions. Facial Plast Surg. 2019;35(3):299-305.
6. Arasaratnam RBS, Halliday LA, Carr JS, Parkin I, Zoysa N. Repair of large holes in stretched earlobes. Clin Otolaryngol. 2011;36(6):588-98.
7. Maiolini VM, Sbroglio LL, Marques RB, Silva RT, D'Elia MLN. Proposal of a new surgical technique to repair gauge earlobe defect. Surg Cosmet Dermatol. 2020;12(4):374-81.
8. Patrocínio LG, Morais RM, Pereira JE, Patrocínio JA. Earlobe cleft reconstructive surgery. Rev Bras Otorrinolaringol. 2006;72(4):447-51.
9. Kalimuthu R, Larson BJ, Lewis N. Earlobe repair: a new technique. Plast Reconstr Surg. 1984;74(2):299-300.
10. Fatah MF. L-plasty technique in the repair of split earlobe. Br J Plast Surg. 1985;38(3):410-4.
11. Fearon J, Cuadros CL. Cleft earlobe repair. Ann Plast Surg. 1990;24(3):252-7.
12. Miller TR, Eisbach KJ. Repair of enlarged pierced-ear openings. Ear Nose Throat J. 2005;84(5):276-7.
13. Reiter D, Alford EL. Torn earlobe: a new approach to management with a review of 68 cases. Ann Otol Rhinol Laryngol. 1994;103(11):879-84.
14. Ribeiro AA, Lourenço L, Matsuda TMHB, Ferrari NM. Split earlobe repair: literature review and new technique proposal. Surg Cosmet Dermatol. 2009;1(3):141-4.
15. Sharma R, Krishna S, Kumar S, Verma M. Rotation flap lobuloplasty: technique and experience with 24 partially torn earlobes. Int J Oral Maxillofac Surg. 2014;43(10):1206-10.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}