


Isabela Karina Vilas Boas; Maria Julia de Medeiros Pedroza; Milena Dias da Silva; Beatriz Bernaud Coelho; Magda Blessmann Weber
Funding: None.
Conflict of interest: None.
Submitted on: 06/22/2025
Final decision: 08/07/2025
How to cite this article: Vilas Boas IS, Pedroza MJM, Silva MD, Coelho BB, Weber MB. Diagnosis-to-treatment intervals for melanoma in Brazil: a matter of geography? Surg Cosmet Dermatol. 2025;17:e20250483.
INTRODUCTION: Melanoma is a type of skin cancer originating from melanocytes which may also affect mucous membranes, leptomeninges, and the uveal tract. Although less prevalent than other skin cancers, it has high lethality due to its aggressiveness, making it a significant public health problem in Brazil.
OBJECTIVE: The primary objective of this study was to assess the time elapsed between diagnosis and treatment initiation for patients with melanoma in different regions of the country in 2024. In addition, it sought to identify possible regional disparities in this interval, as well as to correlate this information with existing data in the literature.
METHODS: This cross-sectional study analyzed 4,405 cases of melanoma diagnosed in 2024, focusing on the diagnosis-to-treatment interval based on data from the Brazilian public health information systems (SISCAN, SIH, and SIA). The study assessed compliance with the 60-day legal maximum waiting time established by Law No. 12.732/2012 across the country's five macroregions.
RESULTS: Regional disparities were observed: the South Region had the best indicators (34.25% of cases treated within 30 days), while the North Region had the worst performance (22.41%). A high percentage of cases had no recorded treatment initiation dates (60.86% nationwide; 68.10% in the North), revealing weaknesses in health information systems and possibly in treatment delivery. Persistent delays and regional inequalities highlight structural deficiencies in the provision of oncology care.
CONCLUSION: The findings underscore the need to strengthen the regionalization of care, improve recordkeeping, and implement effective mechanisms to enforce legal time limits.
Keywords: Melanoma; Diagnosis; Brazil.
Melanoma is a malignant skin neoplasm originating from melanocytes. The cutaneous form is the most common, but melanoma can also originate from mucous membranes, leptomeninges, and the uveal tract of the eye.1 Although less frequent than nonmelanoma skin cancers (basal cell carcinoma and squamous cell carcinoma), which have the highest incidence rates according to the 2023 INCA estimate, melanoma has greater invasive and metastatic potential, as well as higher mortality rates. In Brazil, according to the same estimate, there were 1,923 deaths due to melanoma in 2020.2 Therefore, early diagnosis and timely access to treatment are essential to halt its invasive potential and ensure better prognosis for patients and therapeutic success.
In recent years, more widespread dissemination of knowledge about melanoma risk factors that are well established in the scientific literature, such as unprotected sun exposure, white skin, and aging, along with the promotion of protective measures, such as photoprotection, routine skin exams, and public awareness campaigns, has contributed to an increase in treatment rates for malignant skin cancer.2,3 However, an analysis of historical trends shows an alarming scenario for melanoma with regard to incidence rates, mortality rate, and—most importantly—the diagnosis-to-treatment interval.3 Therefore, melanoma represents an important public health problem, particularly because many deaths are primarily linked to delays between diagnosis and treatment (diagnosis-to-treatment intervals longer than 30 days).
Given the impact of increased diagnostic intervals on prognosis and, consequently, on patient mortality, Brazilians are legally entitled, under Law No. 12.732/2012, to begin undergoing treatment in the Brazilian Unified Health System (SUS, Sistema Único de Saúde) within 60 days of reported diagnosis. This first treatment may involve surgery, radiation therapy, or chemotherapy, depending on the case.4 The main objective of this study was to assess the time elapsed between diagnosis and initiation of treatment for patients with melanoma across different regions of Brazil in 2024. In addition, the study sought to identify potential regional disparities in this interval as well as to correlate the findings with data already reported in the literature.1
An analytical cross-sectional study was conducted using data from the Outpatient Information System (SIA, Sistema de Informação Ambulatorial), the Hospital Information System (SIH, Sistema de Informação Hospitalar), and the Cancer Information System (SISCAN, Sistema de Informações de Câncer), available from the IT Department of the Brazilian Unified Health System (DATASUS).3 Case definition was based on matching data from the National Health Card to the International Classification of Diseases (ICD) code reported. Cases were selected using ICD code "C43: Malignant melanoma of skin." The study included cases from January 2024 to December 2024, taking into account Brazil's five macroregions. The time in days between diagnostic examination and initiation of treatment was divided into up to 30 days, 31 to 60 days, more than 60 days, and no treatment information. Surgical procedures performed prior to diagnosis were included in the up to 30 days interval. The data extracted were tabulated in an Excel spreadsheet for detailed analysis.3 According to Brazilian National Health Council Resolution 510/2016, studies using public-domain data do not require review by a Research Ethics Committee.
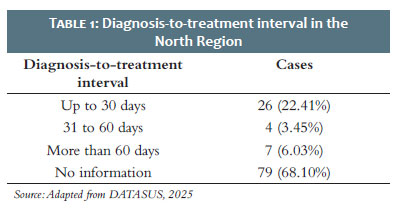
In the North Region of Brazil, 116 cases of malignant skin melanoma were recorded in 2024 (Table 1). An analysis of the interval between diagnosis and initiation of treatment showed a concerning scenario regarding the effectiveness of oncological lines of care in the region. Of the 116 cases, only 26 (22.41%) initiated treatment within 30 days after diagnosis, below the national average of 32.10%.3 This is particularly relevant given that early treatment is directly associated with improved clinical outcomes in melanoma, a neoplasm known for its high metastatic potential.5 In addition, only 4 patients (3.45%) began treatment within 31 to 60 days, a period still compliant with Brazilian legislation (as established by Law No. 12.732/2012). In contrast, 7 patients (6.03%) began treatment more than 60 days after diagnosis, representing severe delays that potentially compromises patient prognosis. The most alarming finding, however, was the lack of information on treatment initiation for 79 cases (68.10%). This number represents more than two-thirds of all cases in the North and is well above the national average of 60.86%.1,4 This gap may reflect both failures in recordkeeping and data monitoring and the absence of treatment delivery, suggesting a possible collapse in information and care systems in the region.6
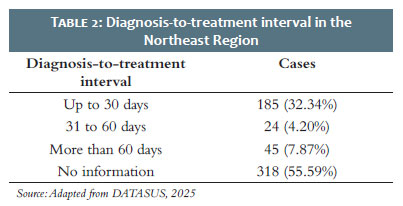
In the Northeast Region, according to DATASUS databases, 572 malignant skin melanoma cases were recorded in 2024 (Table 2). Analysis of diagnosis-to-treatment intervals found more favorable indicators compared to the North but still highlighted significant challenges in access to and the effectiveness of oncology care. Of the total, 185 patients (32.34%) began treatment within 30 days of diagnosis. This percentage is consistent with the national average (32.10%), indicating that approximately one-third of patients in the Northeast received treatment within the time period considered optimal in the scientific literature, consistently associated with higher survival and lower progression rates in melanoma.7-9 In addition, 24 patients (4.20%) began treatment within 31 to 60 days. Although initiation in these cases came after the optimal time period, they were still within the legal limit established by Law No. 12.732/2012, which sets a maximum of 60 days between diagnosis and initiation of treatment in SUS. However, 45 patients (7.87%) only began receiving treatment more than 60 days after diagnosis, the highest rate of severe delays among all regions analyzed so far. This is concerning, given that it suggests structural barriers directly affecting the health care system's resolution rates and response times in treating melanoma.6 Another important point is the large number of cases with no data on treatment initiation. The study found 318 cases (55.59%) with no data on treatment delivery, compromising the analysis of this line of care and the assessment of public policies. Although lower than the Northern average, this figure still represents more than half of all cases in the Northeast, reflecting potential weaknesses in recordkeeping, tracking, and monitoring systems for melanoma patients.6,7
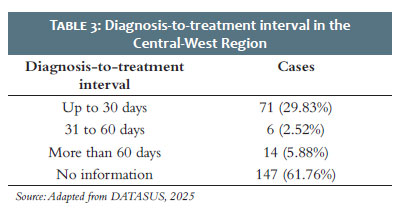
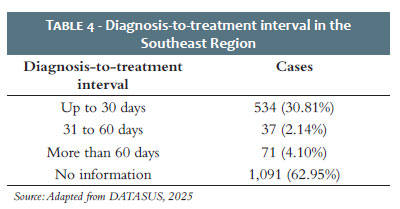
In the Central-West Region, 238 malignant skin melanoma cases were recorded in 2024, according to data from DATASUS information systems (Table 3). The case distribution by diagnosis-to-treatment intervals shows an intermediate scenario compared to other regions of Brazil, with records predominantly lacking information on treatment initiation. Of the total, 71 patients (29.83%) began treatment within 30 days of diagnosis, slightly below the national average (32.10%). Although not the worst-performing region, this percentage indicates that fewer than one-third of patients began receiving treatment within the ideal time period set by clinical best practices, which recommends initiating treatment as soon as possible in order to increase the likelihood of controlling the disease.7-9 An additional 6 cases (2.52%), a very small number, started treatment within 31 to 60 days, an interval still allowed by current legislation (Law No. 12.732/2012). These data highlight that most patients do not initiate treatment within 30 days of diagnosis nor within the legal limit, which may suggest longer-lasting barriers in the patient care flow.4 In addition, 14 patients (5.88%) began treatment more than 60 days after diagnosis, after the legal limit and representing a critical delay, with potential negative consequences for their clinical prognosis.10-13 This is a significant rate, and similar to those found in other regions with greater structural problems, such as the North and the Northeast. The most significant datum, however, was the number of cases with no information on treatment initiation, totaling 147 records (61.76%). This rate is higher than the national average (60.86%) and ranks as the third-highest among the five regions, behind only the North and the Southeast. The absence of this information severely compromises analyses of care effectiveness and hinders the process of monitoring public cancer policies in the region. The Southeast Region accounted for the highest absolute number of malignant melanoma cases in 2024, totaling 1,733 records (Table 4). This substantial figure represents a significant share of the national sample included in this study, reflecting both the population density of the region and the greater capillarity of its reporting systems. In terms of diagnosis-to-treatment intervals, 534 patients (30.81%) initiated treatment within 30 days. Although slightly below the national average (32.10%), this rate demonstrates relatively efficient responsiveness for cases that do undergo treatment. However, when one considers the total number of patients, this percentage means that fewer than one-third initiated treatment within the optimal time period, showing timeliness is not universal even where there is greater service availability. Only 37 cases (2.14%) began treatment within 31 to 60 days, a much lower percentage than observed in other regions. This rate suggests that, in practice, cases not treated quickly tend to exceed the legal time limit or may not even be recorded as treated. In addition, 71 patients (4.10%) started treatment more than 60 days after diagnosis, after the time limit established by Law No. 12.732/2012. While this number is comparable to other regions, the absolute number is significant due to the large volume of cases in the Southeast. The most concerning finding, however, was the 1,091 records (62.95%) with no information on treatment initiation data. That figure is equivalent to nearly two-thirds of all cases in the region and is higher than the national average (60.86%), evidence of serious issues in tracking patient care.14 The magnitude of that number in one of Brazil's most structurally developed regions suggests that missing data may be associated with both failures in information systems and real gaps in access or continuity of care.14,15
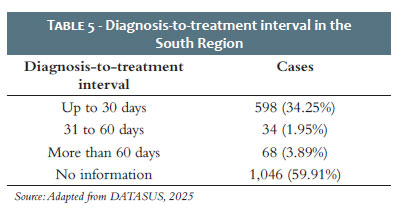
In the South Region, 1,746 cases of malignant skin melanoma were recorded in 2024, making it the second-highest absolute number among Brazil's five macroregions (Table 5). An analysis of diagnosis-to-treatment intervals shows slightly more efficient performance compared to the national average, especially regarding treatment initiation within the optimal period. Out of the total, 598 patients (34.25%) began treatment within 30 days of diagnosis. This is the highest rate among all regions, and above the national average (32.10%). This suggests that a higher proportion of patients in the South had timely access to treatment, possibly reflecting better organization of health care networks and greater capillarity of specialized services.16 Within the 31 to 60 days range, only 34 patients (1.95%) initiated treatment, the lowest percentage among all regions. Though still within the time limit established by Law No. 12.732/2012, the small number of cases in this interval may suggest a trend towards polarization: patients are either treated promptly or experience more severe delays.3,4 The share of patients initiating treatment more than 60 days after diagnosis was 3.89% (68 cases), similar to that found in other regions, such as the Southeast (4.10%). Although the two rates are similar, this indicator also shows a significant group of patients outside the legal time limit, which may directly compromise clinical outcomes in melanoma, a highly lethal neoplasm when treated late.4,10,13 Finally, 1,046 cases (59.91%) had no information on treatment initiation, a figure close to the national average (60.86%). Though the lowest rate among all regions, it still represents a substantial gap that hinders a full assessment of the effectiveness of health care networks. Information may be missing both due to recording failures and to actual lack of treatment initiation.
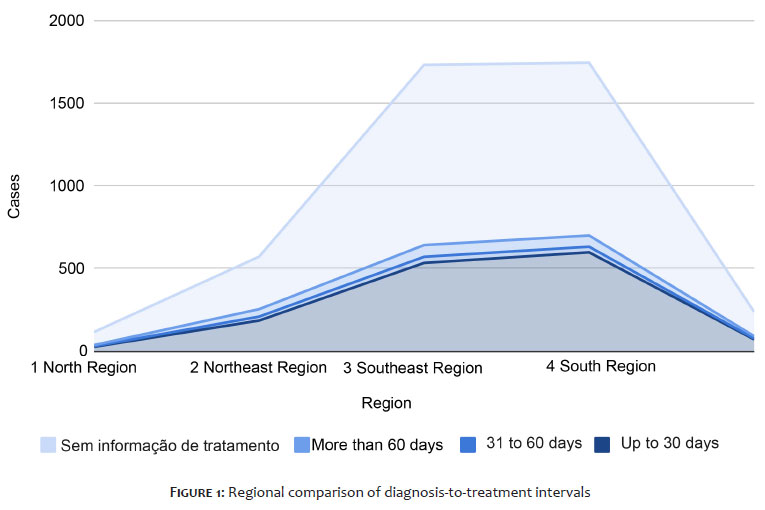
The data highlight a striking pattern of regional inequality in access to treatment for patients diagnosed with malignant skin melanoma in Brazil. When analyzing the percentage of patients who initiated treatment within 30 days of diagnosis—considered the optimal interval for better clinical outcomes—significant variations were observed among the country's macroregions.3 The South had the best performance, with 34.25% of cases treated within the ideal time period, followed by the Northeast (32.34%), Southeast (30.81%), Central-West (29.83%), and, finally, the North (22.41%), the most critical in this respect (Figure 1). These data reveal that while some regions can achieve rates close to or above the national average (32.10%), others, such as the North, face systemic challenges in ensuring timely treatment initiation, despite legislation guaranteeing this right (Law No. 12.732/2012). This asymmetry can be understood in light of historical and structural inequalities among Brazilian regions. The geographic distribution of specialized services, such as oncology and dermatology services, is clearly concentrated in the South and Southeast Regions, which have the highest number of high-complexity hospitals, specialized professionals, and logistical infrastructure. On the other hand, the North faces challenges related to a shortage of professionals, vast geographic distances, transportation limitations, and low density of specialized hospitals, directly compromising the diagnostic-therapeutic flow of oncology patients.4,6,16 The literature supports this scenario. Oliveira et al., in a study conducted in 2020, demonstrated that regions with lower human development indices have higher rates of late-stage diagnoses, a result directly associated with the scarcity of specialized services and the low resolution rate of primary care. This finding is in line with those for the North Region, where only 22.41% of cases began receiving treatment within 30 days, and nearly 68% had no record of treatment initiation. The weakness of the oncology network in the region manifests itself not only as limited access but also as an inability to record, monitor, and ensure continuity of care. Complementarily, the thesis of Oliveira et al. broadens this perspective by showing that socioeconomic inequalities and poor territorial distribution of health care resources are reflected not only in cancer mortality indicators, but also in the conditions under which patients access the system—often in advanced stages of the disease and without a clear prospect of prompt therapeutic referral.6 This scenario is reinforced by our findings for the Northeast and Central-West regions, where the rates of delays greater than 60 days, although variable, coexist with high rates of incomplete or missing records, hindering any evidence-based planning action.3
The central critique that emerges from these data and from theoretical analyses is the fragility of the principle of equity, one of the pillars of SUS. Although SUS was conceived as a universal and egalitarian system, in practice it operates in a highly unequal way, penalizing populations in peripheral and more vulnerable territories. The combination of physical, logistical, and institutional barriers generates a cumulative effect that delays diagnosis, hinders access to care, and ultimately compromises the survival of patients with melanoma and other types of cancer.1,17 Therefore, the results of this study reaffirm the existence of a deeply rooted pattern of regional inequality, which compromises equity in access to oncology care.6,7,17 Although melanoma is less prevalent than other types of skin cancer, its potential for invasiveness and mortality makes attention to the regional barriers that delay treatment even more urgent.7,10 Confronting these disparities must take into account the effective regionalization of oncology, the strengthening of infrastructure in remote areas, and the improvement of territorial planning for SUS, with the goal of guaranteeing timely and comprehensive access to health care for all Brazilians.
One of the most concerning findings of this study is the high number of melanoma cases recorded without any information on treatment initiation.3 The national average, with 60.86% of records lacking data regarding therapeutic initiation, is alarming and compromises not only individual clinical care but also the formulation, evaluation, and oversight of oncology policy in Brazil. This lack of information affects all regions, especially the North, where 68.10% of cases have no record of treatment initiation, and the Southeast, where the highest absolute number of cases is concentrated and where this rate reaches 62.95%. Even the South Region, which had the best performance in terms of promptness of treatment initiation, had 59.91% incomplete records. These percentages show that the problem transcends regional inequalities and points to a systemic weakness in the processes of recording, reporting, and monitoring therapeutic actions.18
It is necessary, therefore, to reflect on whether this lack of information stems from a merely administrative failure—such as not filling mandatory fields in the SISCAN, SIH, or SIA systems—or whether it reveals an even more serious reality: the actual non-initiation of treatment for a significant portion of patients.6,16,18 Both hypotheses are cause for concern. In the first case, the failure compromises the reliability of the national health surveillance systems and prevents the correct assessment of the effectiveness of Law No. 12.732/2012, which mandates that cancer treatment initiate within 60 days after diagnosis.4 In the second case, it implies the very right to health care is being denied, constituting a large-scale legal and ethical violation. The invisibility of these data is even more impactful in contexts of greater social and geographic vulnerability. Patients living in regions distant from urban centers, with low educational levels and less access to information and to justice, tend to be the most affected by this neglect toward recordkeeping and health care. As discussed by Oliveira et al. in 2020, this statistical invisibility is not neutral: it acts as an instrument of exclusion by erasing realities that would require urgent state action.6
The absence of data produces a false sense of control and effectiveness, masking inequalities and perpetuating institutional inaction. Furthermore, the lack of recorded data on treatment directly affects planning capacity and the evaluation of public managers. Without accurate data, measuring the effectiveness of the national cancer control policy, identifying logistical bottlenecks, prioritizing investments, and articulating health care networks that guarantee comprehensiveness and continuity of care become unfeasible.18 Therefore, addressing this gap should not be understood merely as a technical issue of improving information systems, but as an essential strategy of equity and health care justice. The qualification of records, systems integration, continuing training and education of professionals responsible for notifications, and the use of technology to automate and cross-check data are possible paths to make SUS more transparent, responsive, and committed to the lives of its users.14,17
Law No. 12.732/2012, enacted with the aim of ensuring that patients diagnosed with cancer begin treatment within a maximum of 60 days, represents an important regulatory landmark in the struggle for equitable access to oncology care in Brazil.4 However, the data from this study show that, despite the existence of this legislation, there is still a significant share of patients whose rights are not enforced.3,6 In 2024, between 4.10% (Southeast) and 7.87% (Northeast) of recorded cases initiated treatment more than 60 days after diagnosis, exceeding the legal limit. While these percentages may seem modest at first, they are highly significant for patients with malignant melanoma, an aggressive subtype of skin cancer characterized by high metastatic potential and rapid progression.1,11 In such cases, delayed treatment initiation may mean the difference between a favorable prognosis and fatal progression.7,10,13 The persistence of these delays raises serious questions about the actual effectiveness of Law No. 12.732/2012.4
The absence of systematic oversight mechanisms, institutional accountability, and real-time monitoring means that, in practice, the law depends on the organizational capacity of health care services rather than its binding legal authority.17,18 This weakness enables the standards to be generally ignored, with no formal consequences for the health care managers and institutions involved. In addition, the fragmentation of oncology networks, health care gaps in certain regions, and poor integration between primary, specialized, and hospital care make compliance with legal time limits difficult, especially in areas where centralized services force patients into long travel and waiting times. The Northeast, with the highest share of delays exceeding the legal limit (7.87%), exemplifies how a combination of structural, socioeconomic, and geographic factors negatively impacts the enforcement of current legislation.16,17
It should be emphasized that the biological nature of melanoma requires an immediate therapeutic response. Studies show that delays of eight weeks or more in treatment initiation are associated with increase mortality and onset of metastasis, particularly in thick or ulcerated melanomas.11,14 Thus, cases exceeding 60 days often represent irreversible losses of therapeutic opportunity. Therefore, a critical analysis of the data indicates that legislation by itself has been insufficient to ensure timely access to care. Without a strong surveillance system, institutional accountability, and active care flow management, the law runs the risk of becoming dead letter.18 It is crucial that the state take a more proactive role in expanding this right, investing in expanding oncology capacity, particularly in vulnerable regions, and promoting integrated systems that enable real-time tracking of diagnostic-treatment intervals.
This study has important implications for clinical practice, health care planning, and policymaking, particularly for SUS. The analysis of diagnosis-to-treatment intervals for melanoma found not only marked regional disparities but also systemic weaknesses in mechanisms involving regulation, monitoring, and access to oncology care in Brazil.6,16,17 The high rate of patients without treatment information—over 60% across all regions—must be understood as a warning sign of institutional inefficiency. This statistical invisibility not only distorts the reality of actual health care practices but also hinders evidence-based decision-making.
The absence of reliable data compromises territorial planning for the oncology network, resource allocation, policy effectiveness evaluation, and prioritization of investments in vulnerable regions.18 The data indicate the urgent need for targeted interventions, prioritizing regions such as the North and Central-West, where rates of compliance with legal time limits for treatment initiation are lowest and incomplete records highest. These regions should be the focus of public policy that combine expanding installed capacity, training and retaining specialists, strengthening primary care, and improving health information systems such as SISCAN.16,17 In addition, the results underline the importance of regionalizing oncology care equitably, promoting access to specialized services outside major urban centers. Strategies such as teledermatology, mobile early-diagnosis centers, and integrated lines of care may be effective alternatives to reduce delays, especially in remote areas. Clinical practice should also be reassessed in light of these findings. Primary and specialized care professionals must be trained not only for early melanoma diagnosis but also to ensure immediate referral and proper recording of treatment.
Strengthening integration across primary, medium, and high-complexity care is essential to ensure continuity and comprehensiveness, core principles of SUS.17 Finally, these findings highlight the need to revise the implementation strategies of Law No. 12.732/2012, especially in terms of establishing active monitoring and institutional accountability systems. Enforcing legal time limits should be a high-priority task for health care managers, not a secondary one.4 This study contributes to the consideration of melanoma as a marker of the Brazilian health care system's responsiveness and reinforces the urgency of more robust, region-sensitive, and data-driven public policy, aiming at more equitable access to effective therapies.
This study has some important limitations, especially regarding the source and nature of the data. The analysis was based on secondary data from SUS's public information systems (SISCAN, SIH, SIA), which, though widely used in health research, are susceptible to inconsistencies, underreporting, and delayed input. This is reflected, for instance, in the high rate of cases without information on treatment initiation, which makes it difficult to accurately assess public policy effectiveness. Another relevant limitation is the absence of data on tumor staging at diagnosis, which prevents an analysis of diagnosis-to-treatment intervals as a function of clinical severity. This is particularly important for melanoma, where aggressiveness varies by lesion depth and extension. The absence of this information hinders the capacity of this study to correlate therapeutic delays to objective clinical outcomes. In addition, part of the data input into information systems may be self-reported or inconsistently entered across health care units, compromising uniformity and comparability between regions. This calls for caution in interpreting results and highlights the need to improve health records.6,16,18
Based on the limitations and findings above, future studies could further explore the effects of treatment delays on melanoma, especially in terms of the impact of diagnosis and delayed initiation of therapy on survival and disease progression. Longitudinal studies tracking patients over time would be particularly useful in identifying high-risk profiles and in assessing the effectiveness of interventions.17 In addition, qualitative analyses of the experiences of patients and health care professionals involved in oncology care are recommended. Considering the lived experience, perceived barriers, and coping strategies could reveal subjective and contextual dimensions not captured by quantitative data, further enriching our understanding of these phenomena.6 Finally, further studies could explore predictive models based on territorial and socioeconomic data in order to identify priority areas for interventions as well as to assess the impact of local programs and public policies aimed at improving melanoma care in Brazil.16,18
The results of this study reaffirm the existence of significant regional inequalities and structural weaknesses in access to oncology care in Brazil, particularly regarding treatment for malignant skin melanoma. Analyzing the interval between diagnosis and initiation of treatment revealed not only frequent delays and noncompliance with current legislation but also alarming information gaps in national databases, undermining the effectiveness of public policies and of health governance itself. Inequality of access, marked by geographic, socioeconomic, and structural disparities, systematically disadvantages the populations of vulnerable regions, such as the North and Central-West, perpetuating a state of health inequity. In addition to representing an administrative failure, the high percentage of cases without information on treatment also serves as an indicator of invisibility to care, especially in historically neglected territories.
Persistent delays beyond the legal limit established by Law No. 12.732/2012 underline the need to revise mechanisms of implementation, monitoring, and accountability, since the existence of legislation has not, by itself, ensured an effective right to timely treatment. Given this situation, it is crucial that SUS improve its information system, regionalize oncology services equitably, and integrate various care levels more efficiently. Strategies such as strengthening primary care, expanding diagnostic and treatment centers in remote areas, and using technologies such as telemedicine may contribute to overcoming these barriers.
Finally, this study highlights the importance of high-quality data, attuned to the regional and social specificities of Brazil, in driving public policy. The aggressiveness and rapid progression of melanoma make it a relevant indicator of responsiveness in the Brazilian health care system, and addressing the inequalities discussed in this study is essential to ensuring the universal right to health care and guaranteeing comprehensive oncology care in Brazil.
Isabela Karina Vilas Boas
ORCID: 0009-0007-9895-4687
Preparation and writing of the manuscript; acquisition, analysis and interpretation of data; intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; critical review of the literature.
Maria Julia de Medeiros Pedroza
ORCID: 0009-0009-6410-3870
Preparation and writing of the manuscript; acquisition, analysis and interpretation of data; intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied.
Milena Dias da Silva
ORCID: 0009-0006-4147-1644
Acquisition, analysis and interpretation of data.
Beatriz Bernaud Coelho
ORCID: 0009-0004-2604-7672
Preparation and writing of the manuscript.
Magda Blessmann Weber
ORCID: 0000-0001-5885-5851
Effective participation in the conduct of the study.
1. Garbe C; Becker JC. Melanoma. In: Bolognia JL; Jorizzo JL; Schaffer JV. (Ed.). Dermatologia. Tradução de Adriana de Carvalho Corrêa et al.; coordenação da edição brasileira Célia Luiza Petersen Vitello Kalil. 3. ed. Rio de Janeiro: Elsevier; 2015. p.1883–910.
2. Instituto Nacional de Câncer José Alencar Gomes da Silva (INCA). Estimativa 2023: incidência de câncer no Brasil [recurso eletrônico]. Rio de Janeiro: INCA; 2022. Disponível em: https://www.inca.gov.br/publicacoes/livros/estimativa-2023-incidencia-de-cancer-no-brasil. Acesso em: 1 maio 2025.
3. Brasil. Ministério da Saúde. DATASUS. Tabnet. Brasília, DF: Ministério da Saúde; 2022. Disponível em: https://datasus.saude.gov.br/informacoes-de-saude-tabnet/. Acesso em: 3 ago. 2022.
4. Brasil. Lei nº 12.732, de 22 de novembro de 2012. Dispõe sobre o primeiro tratamento de paciente com neoplasia maligna comprovada e estabelece prazo para seu início. Diário Oficial da União: seção 1, Brasília, DF, 23 nov. 2012. Disponível em: https://www.planalto.gov.br/ccivil_03/_ato2011-2014/2012/lei/l12732.htm. Acesso em: 1 maio 2025.
5. Santos CAD; Souza DLB. Melanoma mortality in Brazil: trends and projections (1998-2032). Ciência & Saúde Coletiva. 2019;24(4):1551–61.
6. Oliveira MM; Andrade SSCA; Oliveira PP; Silva GA; Malta DC. Desigualdades sociais no diagnóstico do câncer do colo do útero no Brasil: um estudo de base hospitalar. Ciência & Saúde Coletiva. 2020;25(3):1003–14.
7. Conic RZ, Cabrera CI, Khorana AA, Gastman BR. Determination of the impact of melanoma surgical timing on survival using the National Cancer Database. J Am Acad Dermatol. 2018;78(1):40-6.
8. Davis LE, Shalin SC, Tackett AJ. Current state of melanoma diagnosis and treatment. Cancer Biol Ther. 2019;20(11):1366–79.
9. Dixon AJ, Sladden M, Zouboulis CC, et al. Primary cutaneous melanoma – management in 2024. J Clin Med. 2024;13(6):1607.
10. Xiong DD, Barriera-silvestrini P, Knackstedt TJ. Delays in the surgical treatment of melanoma are associated with worsened overall and melanoma- specific mortality: a population-based analysis. J Am Acad Dermatol. 2022;87(4):807-14.
11. Zhang MZ, Hines AS, Demer AM, Brewer JD. The impact of surgical delay in primary cutaneous melanoma: a systematic review. Dermatol Surg. 2024;50(6):501-6.
12. Stålhammar G. Delays between uveal melanoma diagnosis and treatment increase the risk of metastatic death. Ophthalmology. 2024;131(9):1094-104.
13. Conic RZ, Cabrera CI, Khorana AA, Gastman BR. Determination of the impact of melanoma surgical timing on survival using the National Cancer Database. J Am Acad Dermatol. 2018;78(1):40-6.
14. Pereira Shimada GD, Mota AA, Souza MC, Bernardes SS. Time-to-treatment initiation for cutaneous melanoma reflects disparities in healthcare access in Brazil: a retrospective study. Public Health. 2022;210:1-7.
15. Johansson M, Brodersen J, Gøtzsche PC, Jørgensen KJ. Screening for reducing morbidity and mortality in malignant melanoma. Cochrane Database Syst Rev. 2019;6(6):CD012352.
16. Puntel L. Acesso universal à saúde: um comparativo entre as cinco grandes regiões brasileiras. 2019. 56 f. Trabalho de Conclusão de Curso (Graduação em Ciências Econômicas) – Universidade Federal do Rio Grande do Sul, Porto Alegre, 2019. Disponível em: https://lume.ufrgs.br/handle/10183/201826. Acesso em: 2 maio 2025.
17. Campos, GWS. Reflexões temáticas sobre eqüidade e saúde: o caso do SUS. Saúde e Sociedade. 2006;15(2):23-33.
18. Teixeira SV, Pimentel TRO, Costa NR. Sistema de vigilância em saúde no brasil: avanços e desafios. Saúde em Debate. 2015;39(104):255-67.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}