


André Martins Ornelas1,2; Clarissa Brito Farias2; Isabelle Sousa Medeiros Torres Ferreira3; Flauberto de Sousa Marinho2
Funding: None
Conflicts of interest: None
Submitted on: 01/17/2025
Accepted on: 06/05/2025
How to cite this article: How to cite this article: Ornelas AM, Farias CB, Ferreira ISMT, Marinho FS. Atypical location of acquired digital fibrokeratoma. Surg Cosmet Dermatol. 2025;17:e20250435.
Acquired digital fibrokeratoma is a rare, benign, fibroepithelial tumor, which commonly presents as a finger-shaped normochromic nodule, typically located at the extremities. When affecting the nails, it usually emanates from the proximal nail fold, rarely arising from the matrix or nail bed. In this report, we describe an unusual case of acquired digital fibrokeratoma located under the nail plate of the right thumb. We describe the clinical, dermoscopic, and histopathological aspects of the lesion, as well as the surgical treatment used, and present a brief literature review on the subject.
Keywords: Nail Diseases; Fibroma; Nails; Skin Neoplasms
Acquired digital fibrokeratoma (ADFK) is an uncommon benign tumor, typically observed on the fingernails or toenails. Its etiology is not fully understood, with trauma considered a possible triggering factor. Clinically, it tends to present as a solitary, asymptomatic, finger-like or dome-shaped nodule, which may cause nail deformities and aesthetic impairment. The diagnosis is based on characteristic histopathological features, including acanthosis, hyperkeratosis, and abundant fibrous tissue. Since the tumor does not regress spontaneously, surgical treatment is usually indicated.
The objective of this report was to describe a case of ADFK originating from the nail matrix of the right thumb, an uncommon site compared to its usual occurrence at the proximal nail fold or nail bed. We present a detailed analysis of the clinical, dermoscopic, and histopathological aspects of the lesion, along with a description of the surgical treatment performed. We conclude with a brief literature review aimed at deepening the understanding of this condition. For this review, we selected articles indexed in the PubMed, SciELO, and Periódicos Capes databases, published between 2009 and 2025. The descriptors used were: "acquired digital fibrokeratoma," "digital fibrokeratoma," and "nail tumor," applying the Boolean operator "and" in the following combinations: "acquired digital fibrokeratoma and histopathology," "acquired digital fibrokeratoma and dermoscopy," and "acquired digital fibrokeratoma and surgery."
A 59-year-old man with a prior history of systemic hypertension and basal cell carcinoma on the face presented to the dermatology service with a complaint of a nail lesion on the right first finger, persisting for 10 years. The patient denied associated symptoms or previous treatments. There was no history of local trauma preceding the onset of the lesion.
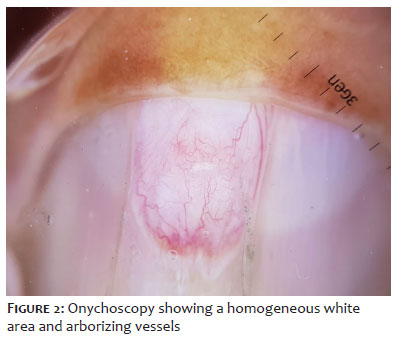
Physical examination revealed a nail plate with canaliform dystrophy and a subungual lesion located at the lunula (Figure 1). On onychoscopy, a homogeneous white area and arborizing vessels were observed (Figure 2). The diagnostic hypotheses considered were fibrokeratoma and superficial acral fibromyxoma.
After proximal digital block, the nail plate was distally elevated to expose the nail bed and matrix. A longitudinal incision was then made in the distal nail matrix, followed by separation and excision of the lesion. The surgical defect in the nail matrix was repaired using 4.0 polyglycolic acid sutures, and the nail plate was repositioned onto the nail bed.
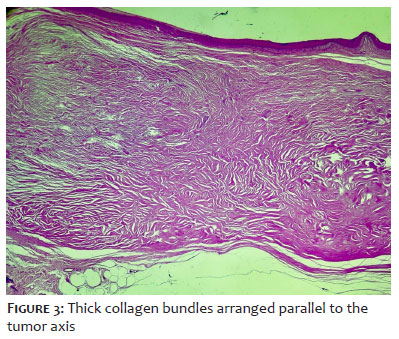
Histological analysis, performed with hematoxylin–eosin staining, demonstrated proliferation of fibroblastic cells and numerous thick, closely packed collagen bundles, regularly distributed within the dermis (Figure 3). These findings are consistent with the diagnosis of ADFK.
ADFK is a rare benign fibroepithelial tumor, first described by Bart in 1968.1 It is most commonly found on the fingers and toes, although cases have been reported in nondigital areas such as the hands, feet, knees, elbows, and forearms, among others. ADFK specifically located in the nail apparatus was designated by Cahn in 1977 as acquired ungual fibrokeratoma, classified into two variants: periungual fibrokeratoma and subungual fibrokeratoma, depending on the location of the tumor.2
ADFK occurs across all races, being more common in men between 12 and 70 years of age, with peak incidence in middle age.3 Its etiopathogenesis is not fully understood, although traumatic events have been suggested as potential contributors. However, a history of trauma is not always reported by patients.4 Local infections by Staphylococcus aureus may also act as triggering factors. Studies have demonstrated increased migration of fibroblasts incubated with S. aureus enterotoxin B.5,6 In addition, some researchers have observed an increased presence of factor XIIIa-positive dermal dendrocytes in ADFK, suggesting they may play a role in collagen synthesis and tumor formation.6
Qiao et al.7 reported the case of a transplant patient who developed concomitant gingival hyperplasia and ADFK while undergoing treatment with cyclosporine. The lesions regressed after discontinuation of the medication, suggesting that the drug may have triggered tumor development. However, no other cases associated with cyclosporine use were found in the literature, indicating that this association warrants further investigation.
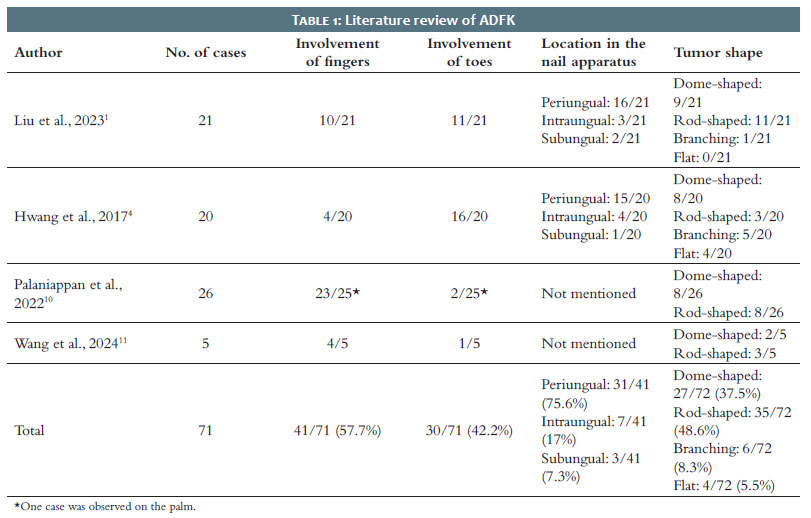
The diagnosis of ADFK is based on characteristic clinical and histological features. Nevertheless, it often represents a true diagnostic challenge, given its rarity and wide range of clinical presentations.2 ADFK generally presents as a solitary, normochromic tumor with a slightly hyperkeratotic tip,5 typically measuring less than 1 cm in diameter and asymptomatic, although there are reports of lesions larger than 1 cm and associated with pain.1 Morphologically, it may present as rod-shaped, dome-shaped, flat, or branching.2 In our literature review, we found that the rod-shaped (47.7%) and dome-shaped (37.3%) types are the most prevalent (Table 1).
ADFK usually arises from the proximal nail fold or, less commonly, from the nail matrix or bed. In a study involving 20 participants, subungual lesions were observed in only 1 patient.4 Another study, with 21 Chinese patients, identified subungual lesions in only 2 cases.1 When compiling three case series, we observed that 56% of patients presented with lesions on the fingers and 44% on the toes (Table 1).
The lesion may exert pressure on the nail matrix, resulting in nail plate deformities such as longitudinal depression8 (as observed in the patient in the present case), thinning of the nail plate, abnormal growth, trachyonychia, onycholysis, subungual hyperkeratosis, and hemorrhagic crust.5 The presence of a collarette at the lesion base is an important clinical finding for differentiating ADFK from other nail tumors.9
Studies investigating in detail the dermoscopic features of ADFK are scarce. In general, onychoscopy demonstrates a central homogeneous light-yellow area surrounded by a hyperkeratotic scaly collarette, reflecting the acanthosis and hyperkeratosis frequently associated with this tumor. Some patients have light white cracks on the nail surface, which may present as punctate blood vessels.1,10 Homogeneous red lacunae have also been described, divided by white meshwork-like keratotic septi, which may correspond to the histologically retracted hyperkeratotic epidermis. This wide variability of dermoscopic findings may be related to the varying degree of vascular formations and collagen fiber accumulation observed in the tumor.6,10 None of these findings, however, provide diagnostic accuracy. In the present case, arborizing vessels were observed – which had not been previously described in the reviewed literature.
In the presence of a fibrous tumor located in the nail apparatus, particularly when elongated in shape, the diagnosis of ADFK should be strongly considered. Differential diagnoses include supernumerary digit, verruca vulgaris, cutaneous horn, Koenen's tumor, eccrine poroma, and superficial acral fibromyxoma.2,9 In a retrospective study, Wang et al.11 reported five cases of ADFK that had been misdiagnosed as eccrine poroma, verruca vulgaris, rudimentary polydactyly, pyogenic granuloma, and acral fibroma. Vance and Hohnadel12 documented the youngest patient with ADFK described to date: a 6-year-old child with a persistent 6-mm nodule on the right first digit, initially misdiagnosed as verruca vulgaris. The high rates of diagnostic error suggest that physicians may not be sufficiently familiar with ADFK.11
The histology of ADFK shows acanthotic epidermis, hyperkeratosis, and focal thickening of the granular layer. In the dermis, thick collagen bundles are observed, arranged irregularly or parallel to the tumor axis. Elastic fibers are generally thin and sparse, and the dermis is usually highly vascularized.1,9
Surgical treatment is recommended, particularly in the presence of pain or cosmetic impairment, since the tumor does not tend to regress spontaneously.4,5 Complete surgical excision is the treatment of choice, as partial removal is frequently associated with local recurrence.2,5 The lesion should be dissected back to its most proximal origin in the nail unit and excised at that site to prevent recurrence.8 To avoid further damage to the nail matrix and ensure complete tumor removal, Jahan et al.3 recommend careful elevation of the lesion and retraction of the proximal nail fold, which allows better visualization of the structures during surgery. Lesions located above the nail plate may also be removed by shaving followed by phenolization or CO2 laser vaporization.3,4 Electrosurgery and cryosurgery have also been reported as alternative treatment options by some authors.10,11
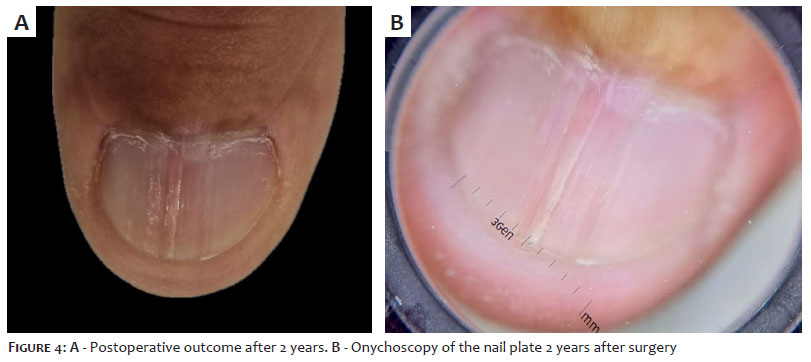
Figures 4A and B show the postoperative outcome 2 years after surgery. To date, no signs of tumor recurrence have been observed.
ADFK is a benign fibroepithelial tumor that usually presents as a solitary, painless nodule measuring less than 1 cm, and only rarely arises beneath the nail plate. The true incidence of ADFK may be underestimated, as it resembles several benign lesions that generally do not require routine histopathological examination. Early recognition and adequate treatment are essential to prevent nail deformities. The recommended therapeutic approach is surgical excision, which must be performed with caution to avoid damage to the nail matrix.
The diagnosis of nail tumors represents a true challenge in dermatologic practice, particularly when lesions occur beneath the nail plate. Biopsy is often required for diagnostic clarification, which entails high cost and the risk of permanent nail dystrophy. Therefore, in the presence of a fibrous nodule located at the nail fold, bed, or matrix –especially when dome-shaped or finger-like – ADFK should be considered as a differential diagnosis.
André Martins Ornelas
ORCID: 0009-0002-0393-7205
Study conception and design; manuscript drafting and writing; data collection, analysis, and interpretation; intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; critical review of the literature.
Clarissa Brito Farias
ORCID: 0009-0009-5395-045X
Manuscript drafting and writing; data collection, analysis, and interpretation; critical review of the manuscript.
Isabelle Sousa Medeiros Torres Ferreira
ORCID: 0000-0002-9597-3272
Data collection, analysis, and interpretation.
Flauberto de Sousa Marinho
ORCID: 0000-0002-9337-9931
Final approval of the manuscript; study conception and design; data collection, analysis, and interpretation; intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; critical review of the manuscript.
1. Liu Y, Zhu Y, Chen G, Xu H, Rao Y, Liu K. A retrospective study on the clinical features of skin lesions in Chinese acquired digital fibrokeratoma patients. J Cosmet Dermatol. 2023;23(1):172–8.
2. Sung KY, Lee S, Lee SY. An unusual presentation of acquired periungual fibrokeratoma: a mixed form of dome‐shaped and branching type. Clin Case Reports. 2020;8(11):2129–31.
3. Jahan N, Padubidri Kombettu Ashwini, S. Chethana, Jayadev Betkerur, Shastry
4. V. Horn on the nail: acquired ungual fibrokeratoma. J Cutan Aesth Surg. 2021;14(1):121–4.
5. Hwang S, Kim M, Baik Kee Cho, Hyun Jeong Park. Clinical characteristics of acquired ungual fibrokeratoma. Indian J Dermatol Venereol Leprol. 2017;83(3):337–7.
6. Ballan A, Zeinaty P, Tomb R, Kechichian E, El Hachem L, Nasr M, et al. Acquired ungual fibrokeratoma: a systematic review of the literature. Int Dermatol. 2020;60(5):533–9.
7. Shih S, Khachemoune A. Acquired digital fibrokeratoma: review of its clinical and dermoscopic features and differential diagnosis. Int Dermatol. 2018;58(2):151–8.
8. Qiao J, Liu YH, Fang K. Acquired digital fibrokeratoma associated with ciclosporin treatment. Clin Exp Dermatol. 2009;34(2):257–9.
9. Hare AQ, Rich P. Nail tumors. Dermatol Clin. 2021;39(2):281–92.
10. Pegas JR, Cade KV, Kiyomura MY, Soares A, Mayer L, Tebcherani AJ. Fibroqueratoma digital adquirido: a propósito de um caso clínico. Surg Cosmet Dermatol. 2012;4(4):357–9.
11. Palaniappan V, Sadhasivamohan A, Sankarapandian J, Karthikeyan K. Acquired fibrokeratoma: a retrospective study in a tertiary centre in South India. Indian J Dermatol. 2022;67(3):312.
12. Wang X, Zhang D, Lin Q, Niu C, Fan H, Zhang M, et al. Acquired digital fibrokeratoma: a report of five cases and review of the literature. Clin Cosmet Invest Dermatol. 2024;17:247–52.
13. Vance P, Hohnadel M. Acquired digital fibrokeratoma in a 6‐Year‐Old patient: the youngest reported case. Pediatr Dermatol. 2025;42(4):892-3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}