


Fernando Bulla-Alcala1; Claudia González2; Sara Cataño3; Juan Felipe Ochoa-Bermudez4
Funding: None
Conflict of interest: None
Submitted on: 12/28/2024
Final decision: 01/30/2025
How to cite this article: Bulla-Alcala F, González C, Cataño S, Ochoa-Bermudez JF. Ultrasound for a better surgical approach in hidradenitis suppurativa. Surg Cosmet Dermatol. 2025;17:e20250433.
Hidradenitis suppurativa (HS) is a chronic inflammatory disease affecting intertriginous areas of the body, characterized by painful nodules, abscesses, sinusoidal tracts, and fistulas. Surgery is crucial for treatment, being potentially curative and achieving high satisfaction levels. Pre-surgical evaluations are often limited by the difficulty of detecting fistulous tracts and deep nodules. Ultrasound has emerged as a staging, follow-up, treatment response evaluation, and preoperative management method for HS. It enables accurate localization of subclinical lesions and optimizes surgical results. This report presents two representative cases of pre-surgical ultrasound evaluation in HS.
Keywords: Hidradenitis Suppurativa; Ultrasonography, Doppler; Outpatient Surgical Procedures
Hidradenitis suppurativa (HS) is a chronic inflammatory disease characterized by painful nodules, abscesses, sinusoidal tracts, and fistulas, primarily affecting intertriginous regions such as the axillae and groin.1,2 Treatment is comprehensive, encompassing antibiotics, retinoids, biological therapies, and surgical interventions.3 Surgery remains crucial, as it is the only potentially curative option, achieving high satisfaction levels regardless of disease severity.4
Several classifications are used to assess HS severity. The most widely recognized is the Hurley system, which stages the disease into three levels.2 However, traditional classifications have limitations, including inaccurate assessment of inflammation.5,6 To address these, new scales have been developed. The Modified Hurley scale evaluates body surface area involvement, inflammation, and migratory lesions,7 while the IHS4 (International Hidradenitis Suppurativa Severity Score System) dynamically assesses nodules, abscesses, and fistulous tracts over time.5,6
Physical examination of HS patients has limitations, as fistulous tracts and deep nodules are often undetectable by palpation alone.7 This limitation may lead to inadequate medical and surgical treatment.7-11 Imaging addresses these challenges by clarifying lesion morphology and severity, tracking disease progression, and assisting in pre-surgical mapping.12 Imaging modalities include ultrasound and MRI.13-15 High-resolution ultrasound with Doppler analysis is particularly effective, providing safe, accurate detection of subclinical lesions and active inflammation. It is now considered the standard of care for diagnosis, staging, and preoperative localization of target lesions in HS.7,16-23
We present two cases of patients treated at a Dermatologic Surgery Center in Bogotá, Colombia. Both patients, diagnosed with HS and referred for surgical intervention, underwent high-frequency ultrasound for lesion localization and marking. Informed consent was obtained.
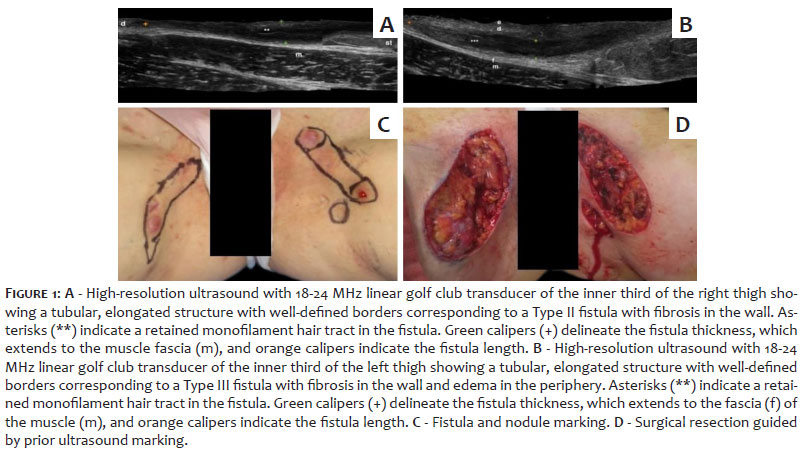
A 25-year-old woman with severe HS (Hurley stage III; IHS4: 19 points) was treated with combined medical management (oral antibiotics) and surgery. Preoperative ultrasound identified isolated dermal edema, follicular dilation, cystic nodules, and fistulas in the bilateral inguinal regions. A complex type II fistula extended from the distal right inguinal region to the proximal thigh, while a type III fistula was observed in the left inguinal region. Ultrasound-guided marking of target lesions facilitated surgical resection (Figure 1). Six months postoperatively, the patient showed adequate healing without recurrence.
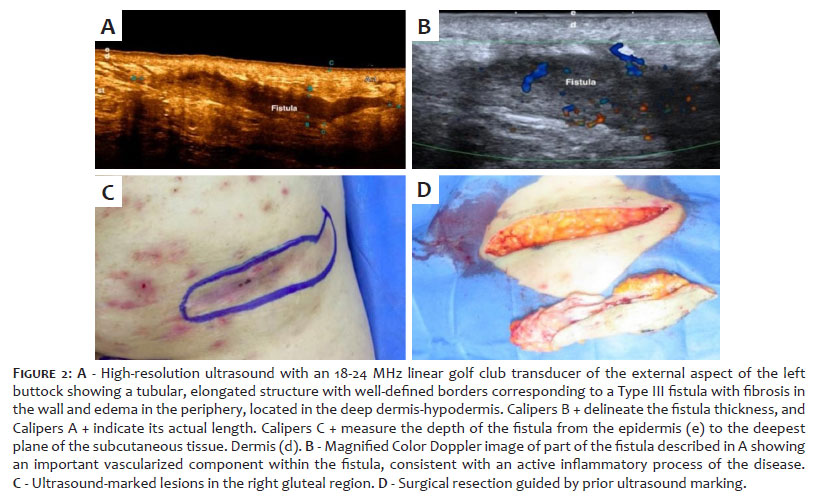
A 58-year-old woman with HS in the inguinal, intergluteal, and gluteal regions had a history of biological treatment and multiple surgical resections. Preoperative ultrasound identified a type III fistula with significant fibrosis in the proximal right buttock and a type II fistula with mild fibrosis and edema in the infragluteal fold. The marking of lesions ensured precise surgical resection (Figure 2). Postoperative outcomes were successful, with no complications or recurrence at one-year follow-up.
Satisfactory postoperative outcomes were achieved in both patients, showing the efficacy of ultrasound-guided surgical resection in improving surgical precision and reducing recurrence.
Pre-surgical planning based solely on clinical parameters often underestimates the extent and severity of HS lesions.22 Visual examination and palpation fail to identify deep or subclinical lesions, resulting in incomplete surgical margins and increased risk of recurrence.7,23 Imaging, particularly ultrasound, addresses these limitations by providing detailed information about lesion boundaries, subclinical activity, and severity.7,18 High-resolution ultrasound with Doppler analysis is especially useful for staging disease, monitoring treatment response, and guiding preoperative planning.7,18,24-26
The modified Sonographic Scoring of Hidradenitis Suppurativa (mSOS-HS) is a validated tool for staging HS based on ultrasound findings27:
Stage I includes one fluid collection and changes in the dermis, such as pseudocysts or follicular dilations.
Stage II involves two to four fluid collections or a fistulous tract with dermal changes affecting up to two body segments.
Stage IIIA includes five or more fluid collections or multiple fistulous tracts, while Stage IIIB involves extensive, bilateral, or interconnected fistulas.
Ultrasound also categorizes fistulas based on fibrosis and edema into three types25:
1. Type I: Minimal fibrosis and low edema.
2. Type II: Moderate fibrosis and low edema.
3. Type III: Severe fibrosis and significant edema.
Detecting fibrosis is particularly important, as fibrotic lesions are less likely to respond to medical therapy.25,28 These cases often require combined medical and surgical management.18 By delineating subclinical lesions and determining fistula depth, ultrasound significantly improves surgical precision.7,17,18,24-27
Certain patient factors increase the likelihood of inadequate surgical margins, including obesity, male gender, Hurley stage II disease, and elevated IHS4 scores.23 These patients benefit most from preoperative ultrasound examination, as it improves lesion localization, reduces recurrence rates, and optimizes surgical outcomes.7,18,24-26 Studies have shown that ultrasound-guided surgical procedures improve margin delineation and decrease recurrence within 24 weeks postoperatively.23
In the cases presented, wide local resections guided by ultrasound ensured complete lesion removal and successful postoperative healing. Ultrasound provided detailed preoperative insights, detecting subclinical lesions and guiding precise resection, ultimately minimizing recurrence and enhancing outcomes.
HS is a chronic disease with significant demands on the treating physician due to its complex management. Surgery is critical, being the only potentially curative intervention. High-frequency ultrasound plays an invaluable role in preoperative planning, enabling the detection of subclinical lesions, precise lesion mapping, and improved surgical outcomes. Incorporating ultrasound into the standard management of HS enhances treatment efficacy, reduces recurrence, and ensures better patient care.
Fernando Bulla-Alcala
ORCID: 0000-0001-6013-8608
Author's contribution: Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Claudia González
ORCID: 0000-0003-2618-308X
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Sara Cataño
ORCID: 0000-0001-5183-6973
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Juan Felipe Ochoa-Bermudez
ORCID: 0000-0003-0038-4692
Approval of the final version of the manuscript, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
1. Lyons A, Zubair R, Kohli I, Hamzavi I. Preoperative ultrasound for evaluation of hidradenitis suppurativa. Dermatol Surg. 2019;45(2):294–6.
2. Goldburg SR, Strober BE, Payette MJ. Hidradenitis suppurativa: epidemiology, clinical presentation, and pathogenesis. J Am Acad Dermatol. 2020;82(5):1045–58.
3. Martorell A, García FJ, Jiménez-Gallo D, Pascual JC, Pereyra-Rodríguez J, Salgado L, et al. Update on hidradenitis suppurative (Part II): treatment. Actas Dermosifiliogr. 2015;106(9):716–24.
4. Fertitta L, Hotz C, Wolkenstein P, Méningaud JP, Sawan D, Hersant B, et al. Efficacy and satisfaction of surgical treatment for hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34(4):839–45.
5. Zouboulis CC, Tzellos T, Kyrgidis A, Jemec GBE, Bechara FG, Giamarellos- Bourboulis EJ, et al. Development and validation of the International Hidradenitis Suppurativa Severity Score System (IHS4), a novel dynamic scoring system to assess HS severity. Br J Dermatol 2017;177(5):1401–9.
6. Horváth B, Janse IC, Blok JL, Driessen RJB, Boer J, Mekkes JR, et al. Hurley staging refined: a proposal by the Dutch hidradenitis suppurativa expert group. Acta Derm Venereol 2017;97(3):412–3.
7. Martorell A, Alfageme Roldán F, Vilarrasa Rull E, Ruiz-Villaverde R, Romaní De Gabriel J, García Martínez F, et al. Ultrasound as a diagnostic and management tool in hidradenitis suppurativa patients: a multicentre study. J Eur Acad Dermatol Venereol. 2019;33(11):2137–42.
8. Wortsman X, Castro A, Figueroa A. Color Doppler ultrasound assessment of morphology and types of fistulous tracts in hidradenitis suppurativa (HS). J Am Acad Dermatol 2016;75(4):760–7.
9. Napolitano M, Calzavara-Pinton PG, Zanca A, Bianchi L, Caposiena Caro RD, Offidani AM, et al. Comparison of clinical and ultrasound scores in patients with hidradenitis suppurativa: results from an Italian ultrasound working group. J Eur Acad Dermatol Venereol. 2019;33(2):e84–7.
10. Gutfilen-Schlesinger G, Lopes De Souza SA, Gutfilen B. Should we scan hidradenitis suppurativa patients? A systematic review of radiologic findings. Adv Skin Wound Care. 2021;34(7):1–10.
11. Lyons AB, Narla S, Kohli I, Zubair R, Nahhas AF, Braunberger TL, et al. Assessment of inter-rater reliability of clinical hidradenitis suppurativa outcome measures using ultrasonography. Clin Exp Dermatol. 2022;47(2):319–24.
12. Mendes-Bastos P, Martorell A, Bettoli V, Matos AP, Muscianisi E, Wortsman X. The use of ultrasound and magnetic resonance imaging in the management of hidradenitis suppurativa: a narrative review. Br J Dermatol 2023;188(5):591–600.
13. Lopes AA, Moraes GN, De Lima Dias BMM, De Souza GD, De Souza LQ. Preoperative imaging assessment of hidradenitis suppurativa. Rev Bras Cir Plast. 2019;34(2):264–7.
14. Wortsman X, Jemec GBE. A 3D ultrasound study of sinus tract formation in hidradenitis suppurativa. Dermatol Online J. 2013;19(6):18564.
15. Elkin K, Daveluy S, Avanaki K. Hidradenitis suppurativa: current understanding, diagnostic and surgical challenges, and developments in ultrasound application. Skin Res Technol 2020;26(1):11–9.
16. Marasca C, Marasca D, Megna M, Annunziata M, Fabbrocini G. Ultrasound: an indispensable tool to evaluate the outcome of surgical approaches in patients affected by hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34(8):413–4.
17. Martorell A, Wortsman X, Alfageme F, Roustan G, Arias-Santiago S, Catalano O, et al. Ultrasound evaluation as a complementary test in Hidradenitis Suppurativa: proposal of a standarized report. Dermatol Surg. 2017;43(8):1065–73.
18. Wortsman X. Color Doppler ultrasound: a standard of care in hidradenitis suppurativa. J Eur Acad Dermatol Venereol 2020;34(10):e616–7.
19. Lacarrubba F, Dini V, Napolitano M, Venturini M, Caposiena Caro DR, Molinelli E, et al. Ultrasonography in the pathway to an optimal standard of care of hidradenitis suppurativa: the Italian Ultrasound Working Group experience. J Eur Acad Dermatol Venereol. 2019;33(Suppl 6):10–4.
20. Wortsman X, Moreno C, Soto R, Arellano J, Pezo C, Wortsman J. Ultrasound in-depth characterization and staging of hidradenitis suppurativa. Dermatol Surg. 2013;39(12):1835–42.
21. Wortsman X, Rodriguez C, Lobos C, Eguiguren G, Molina MT. Ultrasound diagnosis and staging in pediatric hidradenitis suppurativa. Pediatr Dermatol. 2016;33(4):e260–4.
22. Wortsman X. Imaging of Hidradenitis Suppurativa. Dermatol Clin. 2016;34(1):59–68.
23. Cuenca-Barrales C, Salvador-Rodríguez L, Arias-Santiago S, Molina-Leyva A. Pre- operative ultrasound planning in the surgical management of patients with hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34(10):2362–7.
24. Wortsman X, Calderon P, Castro A. Seventy-MHz Ultrasound detection of early signs linked to the severity, patterns of keratin fragmentation, and mechanisms of generation of collections and tunnels in Hidradenitis Suppurativa. J Ultrasound Med. 2020;39(5):845–57.
25. Reyes-Baraona F, Isabel Herane M, Wortsman X, Figueroa A, García-huidobro I, Giesen L, et al. Guía clínica chilena para el estudio y tratamiento de hidradenitis supurativa. Rev Med Chile. 2021;149(artículo especial):1620-35.
26. Wortsman X. Strong validation of ultrasound as an imaging biomarker in hidradenitis suppurativa. Br J Dermatol. 2021;184(4):591–2.
27. Wortsman X. Update on ultrasound diagnostic criteria and new ultrasound severity and activity scorings of Hidradenitis Suppurativa. J Ultrasound Med. 2024;43(1):207–13.
28. Andersen RK, Jemec GB. Treatments for hidradenitis suppurativa. Clin Dermatol. 2017;35(2):218-24.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}