


Isabella Melo Pompei1; Célia Antônia Xavier de Moraes Alves1; Annamaria Piovezan Lorenção1; Bruna Mendes Almeida1; Juliana Arêas de Souza Lima Beltrame Ferreira1; Luciano Melo Pompei2
Research Ethics Committee approval protocol number: 68423723.1.0000.5412
Funding: None.
Conflict of interest: None.
Submitted on: 11/16/2024
Final decision: 06/05/2025
How to cite this article: Pompei IM, Alves CAXM, Lorenção AP, Almeida BM, Ferreira JASLB, Pompei LM. National Skin Cancer Prevention Campaign: analysis of the resolution rate of skin tumors diagnosed during the 2022 and 2023 Skin Cancer Awareness Month campaigns in Jundiaí, Brazil. Surg Cosmet Dermatol. 2025;17:e20250422.
INTRODUCTION: Cutaneous malignant tumors are preventable and have a high cure rate when diagnosed early, resulting in reduced morbidity and mortality. Early-stage cancer detection allows for timely treatment, leading to a better prognosis.
OBJECTIVE: To evaluate the effectiveness of the "Skin Cancer Awareness Month" campaign in identifying potential cases of skin cancer and its resolution rate based on the time required for lesion treatment.
METHOD: A retrospective analytical cross-sectional study with descriptive-quantitative characteristics.
RESULTS: In 2022, the time between biopsy and curative surgery ranged from 94 to 218 days, with a median of 153 days. In 2023, the time between biopsy and curative surgery ranged from 12 to 249 days, with a median of 129 days. A statistically significant difference (p=0.04) was observed between the years 2022 and 2023 in the median time from biopsy to surgery.
CONCLUSION: Improved efficiency in performing biopsies and surgeries, as well as enhanced patient adherence to treatment, was necessary.
Keywords: Carcinoma; Carcinoma, Squamous Cell; Skin Neoplasms; Health Promotion; Time-to-Treatment.
Malignant skin tumors, such as basal cell carcinomas (BCCs), squamous cell carcinomas (SCCs), and melanomas, account for a large share of all cancers in Brazil and worldwide. Among all malignant neoplasms, non-melanoma skin cancer is the most frequent type in both sexes.1 According to Brazil's National Cancer Institute, approximately 30% of all malignant tumors are skin neoplasms, and diagnosis of new cases is expected to increase in coming years to about 180 thousand new cases/year.2,3 The increase in annual incidence rates highlights the trend of increased prevalence of the condition, not only due to global increases in life expectancy but primarily due to the combination of improved diagnostic capacity and longer exposure to risk factors, such as exposure to ultraviolet radiation. The significant increase in the number of skin tumors should come as a warning to health care systems, as well as encourage the deployment of new measures for early screening and diagnosis of skin neoplasms.4,5,6
Overall, skin tumors are caused by the abnormal and uncontrolled proliferation of skin cells. Depending on the skin layers affected, tumors can be divided into several types. The three most common types of skin cancer are, in decreasing order of incidence, BCCs, SCCs, and melanomas.7 BCCs, originating from the basal cells of the skin and skin appendages, primarily affect the H-zone of the face, with 70% of all cases found on the face and head, but may also affect the trunk and limbs. They are characterized by slow growth and low risk of metastases, which gives them high cure rates when detected early.8 SCCs originate from the squamous cells and may be found in any part of the body, and are more common on the lips, ears, scalp, areas of chronic inflammation, scars, and burns.8 Melanomas, in turn, are a more aggressive and fatal form of tumor, although fortunately rarer than the other two. While its diagnosis is a source of patient anxiety, when made early and assertively, the condition has cure rates of over 90%.9,10 The risk factors for developing this form of cancer are well known, facilitating primary prevention and health promotion by raising awareness about risk behaviors, warning signs, and periodicity of prevention.
Therefore, skin neoplasms are a preventable disease when exposure to carcinogenic agents is reduced or eliminated, and when individual susceptibility to those agents is likewise limited.11 In addition, malignant skin tumors, when diagnosed early, are known to have high cure rates—approximately 90%—resulting in lower morbidity and mortality.9,10 They are also a preventable type of cancer, with exposure to ultraviolet radiation without the use of photoprotection the primary risk factor. Therefore, early-stage detection of a neoplasm allows for timely treatment, leading to a better prognosis. Meanwhile, one should pursue means of implementing primary prevention measures, encourage the use of educational programs in schools and communities, increase early detection campaigns, improve therapeutic management of diagnosed cases, and reduce morbidity and costs to the health care system through early screening and effective treatment of lesions.4
With regard to early treatment of skin cancer, it should be stressed that health awareness campaigns represent an advancement in patient care, encompassing both primary and secondary prevention. Primary prevention is performed before the disease—in other words, it is based on unspecific protective measures against risk and damage through reduced exposure of individuals to disease risk factors in order to lower its incidence.12 Secondary prevention, in turn, occurs when the disease is subclinical or in its early stages. Despite our inability to change genetic predisposition, this stage enables us to lower the exposure to the factors causing tumors.13
Accordingly, the relevance of skin cancer prevention campaigns deserves more attention. The National Skin Cancer Prevention Campaign (NSCPC), established by the Brazilian Society of Dermatology in 2014, aims at preventing skin neoplasms through health promotion by warning, informing, and raising awareness among the population, focusing on primary prevention. The campaign also has a secondary prevention component based on screening efforts for early diagnosis of potential malignant skin lesions. Thus, it enables rapid treatment, lower mortality, and increased survival for patients.5
Currently, there are few Brazilian and/or Latin American studies on the resolution rates of primary and/or secondary prevention measures adopted to fight and treat skin cancer. The paucity of recent studies requires better assessment of dermatology practitioners, justifying the need to assess the effectiveness of measures adopted after a skin neoplasm has been diagnosed, since the number of patients with skin tumors only tends to increase, as do the impact and the consequences of the disease on their lives.
To evaluate the effectiveness of NSCPC in identifying potential cases of skin cancer and its resolution rate based on the time required for lesion treatment. In addition, the study aimed at determining the epidemiological pattern found in the 2022 and 2023 NSCPCs.
This is a retrospective analytical cross-sectional study with descriptive-quantitative characteristics. It was conducted based on records collected during NSCPC at the Faculdade de Medicina de Jundiaí (FMJ) outpatient dermatology service in Jundiaí, São Paulo, Brazil. The sample size corresponded to the maximum number of participants the researchers were able to approach during the 2022 and 2023 NSCPCs and who fit the inclusion criteria, totaling 158 individuals. The survey included all patients aged 18 years and older, as well as those with suspected diagnosis of skin cancer as assessed by FMJ dermatologists. Participants who did not agree to sign an informed consent form were excluded. This study was submitted to the FMJ Research Ethics Committee (REC). Analysis of the data collected from NSCPC survey forms began once the REC gave its approval. The data were input in a Microsoft Excel® (Microsoft Corporation®, San Diego, USA) electronic spreadsheet. Statistical analysis was performed using the StatPlus® (AnalystSoft Inc.) plugin for Excel, with numerical data presented as mean (SD) or median (IQR). The Mann-Whitney U test was used to compare the years 2022 and 2023. The level of significance was set at 5%.
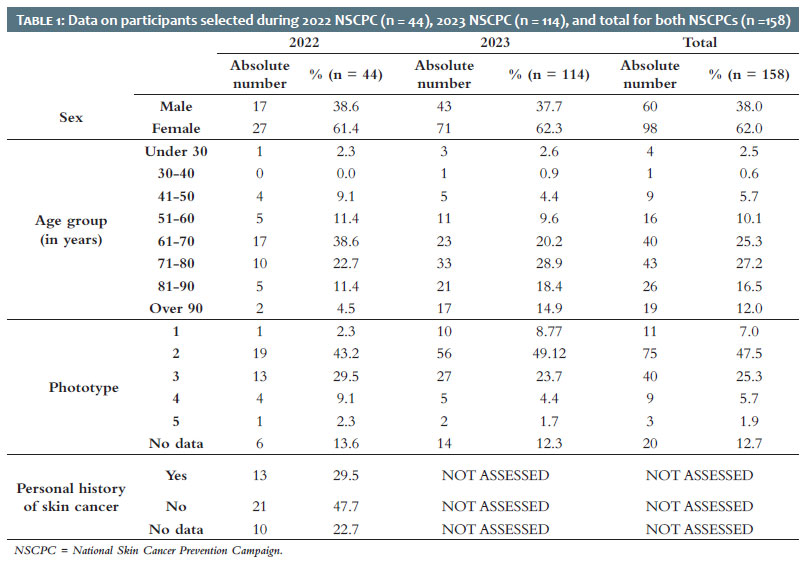
The total number of participants in the 2022 NSCPC who met the selection criteria for this study was 44, the majority of which consisted of 27 women (61.4%), compared to 17 men (38.6%). In 2023, 114 patients met the inclusion criteria and were referred for further investigation, with 71 women accounting for the majority of the sample (62.3%) and 43 men accounting for 37.7% of the total (Table 1).
In 2022, individuals aged 61-70 years had the highest rate of participation in the study, with 17 participants (38.6%), followed by those aged 71-80 years, with 10 participants (22.7%). Only two patients (4.5%) were older than 90 years, and the least represented age group consisted of individuals under 30 years of age, with a single individual (2.3%). There were no participants aged 30-40 years. In 2023, incidence rates were similar, differing only in the switch between the two dominant age groups: the largest group of participants was 71-80 years of age, with 33 individuals (28.9%), followed by the 61-70 years age group, with 23 individuals (20.1%). In addition, there was an increase in the total number of participants over 90 years of age, totaling 17 individuals (14.9%) (Table 1).
The phototype most affected by skin tumors, in both 2022 and 2023, was phototype 2, accounting for 19 (43.1%) and 56 participants (49.1%), respectively, followed by phototype 3, with 13 (29.5%) and 27 (23.6%). However, a great number of records were found to lack this piece of information: six records (13.6%) in 2022 and 14 records (12.2%) in 2023, which may hinder proper data analysis (Table 1). Regarding personal history of skin cancer, a high number of records were found to lack this piece of information, totaling 10 records (22.7%). From the data available, 21 patients (47.7%) were found to have no personal history of the disease. The 2023 data on personal history of neoplasms were not analyzed in this study.
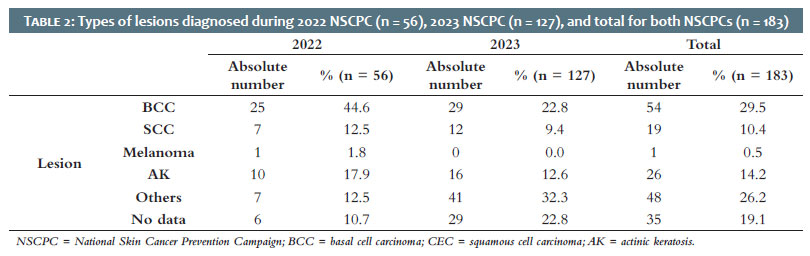
In terms of the type of skin lesion found by dermatological examination, in 2022 most lesions consisted of BCC, with 25 cases (44.6%), followed by actinic keratosis (AK), with 10 cases (17.8%), and SCC, with seven cases (12.5%). Pigmented lesions, suggestive of melanoma, accounted for one case (1.7%). It should be noted that lesions outnumber participants because some patients had more than one lesion. In 2023, the largest share consisted of non-neoplastic lesions, totaling 41 cases (32.3%), followed by BCC, with 29 lesions (22.8%), and SCC, with 12 cases (9.4%). That same year, no pigmented lesion suggestive of melanoma was diagnosed (Table 2).
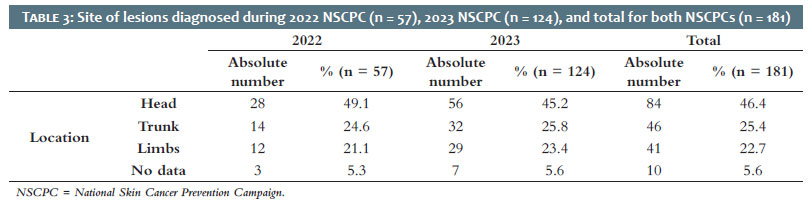
Regarding the site where the lesions were found, similar rates were observed in both 2022 and 2023. In the head and neck region, 28 cases (49.1%) were found in 2022 and 56 cases (45.1%) in 2023, totaling almost half of all lesions. In the trunk, 14 lesions (24.5%) were recorded in 2022 and 32 lesions (25.8%) in 2023. Percentages for lesions found on the limbs remained similar, with 12 lesions (21.1%) in 2022 and 29 lesions (23.3%) in 2023 (Table 3).
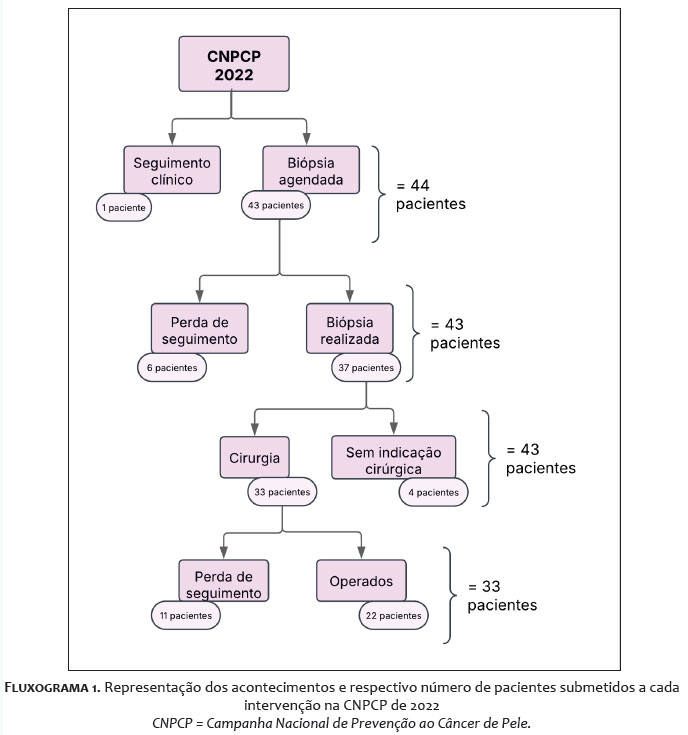
Cases assessed with possible outcomes of skin neoplasms were referred for biopsy in order to determine follow-up for each patient. In 2022, only one patient was directly referred for clinical follow-up with 5-fluorouracil (2.3%), while the remaining 43 (97.7%) were referred for biopsy. Out of these, six (14.0%) were lost to follow-up, 35 (81.3%) underwent punch biopsy, and only two (4.7%) underwent resection. After biopsy results, four patients (9.3%) had no surgical indication, six (14.0%) were lost to follow-up, and 33 (76.7%) had indication for surgical procedures and their procedures were scheduled (Flowchart 1).
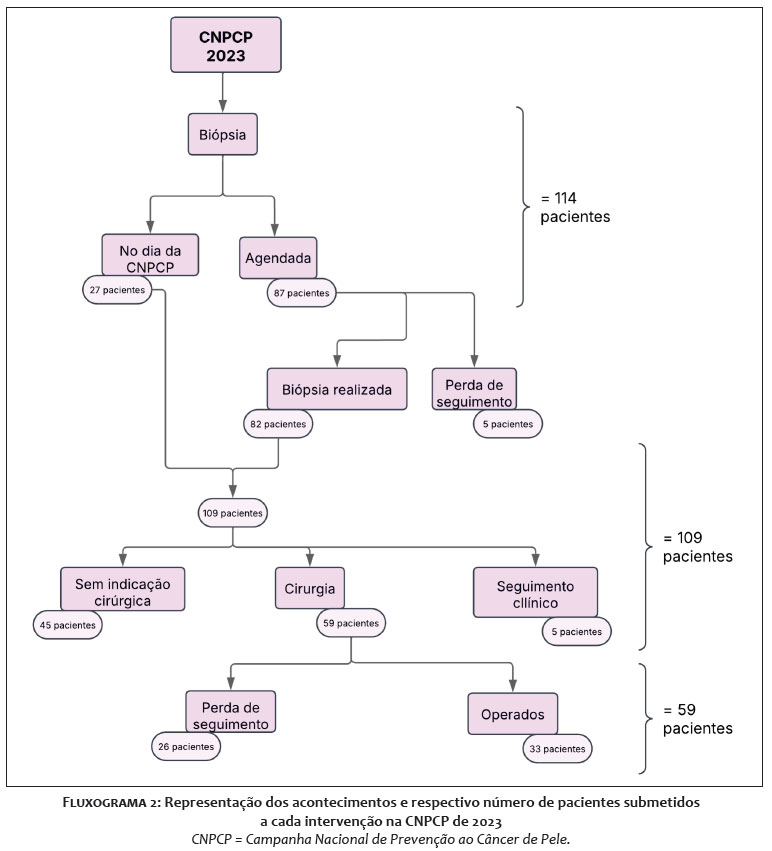
In 2023, out of 114 patients, only five (4.4%) failed to attend on the day of the biopsy. Among those who continued follow-up, 38 (34.9%) underwent resection and 71 (65.1%) underwent punch biopsy. After biopsy results, clinical follow-up was recommended for five patients (4.6%), there was no surgical indication for 45 patients (41.3%), and the remaining 59 (54.1%) were referred for surgical procedures (Flowchart 2).
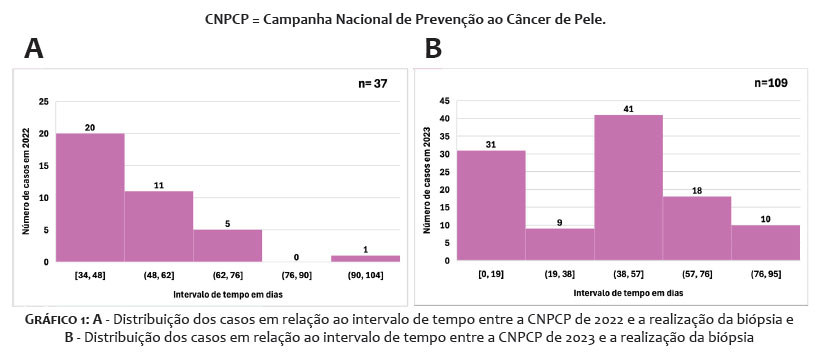
The time between the 2022 NSCPC and the biopsy of the lesions assessed on the screening day ranged from 34 to 100 days, with a mean (SD) of 49.8 (13.1) days between the two events and a median of 47.0 days (IQR 40-53). Out of 37 patients referred for biopsy, 20 (54.1%) waited between 34 and 48 days to complete this step. An additional 11 patients (29.7%) required from 49 to 62 days, and only one (2.7%) waited over 90 days (Graph 1A). In 2023, the time between the NSCPC and the biopsy of the lesions assessed during the event ranged from 0 to 86 days, with a mean (SD) of 39.2 (26.2) days between the two events and a median of 47.0 days (IQR 12-58). Out of 109 patients who showed up on the day scheduled for their biopsies, 31 (28.4%) underwent the procedure in less than 20 days. The majority, 41 (37.6%), waited between 39 and 57 days, and only 10 (9.2%) required 77 to 95 days to undergo biopsy (Graph 1B).
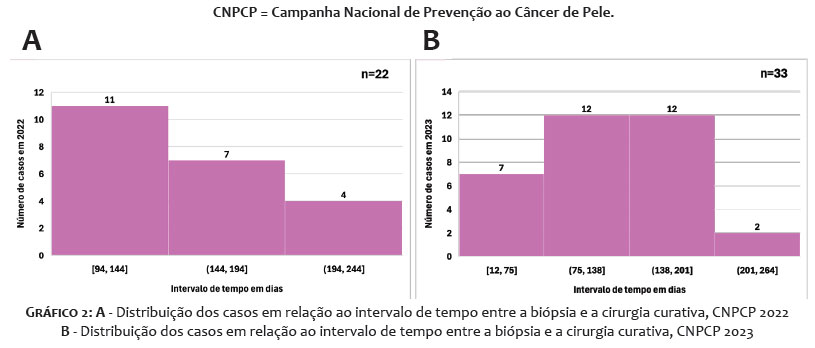
A major difference between the 2022 and 2023 NSCPCs was the performance of excisional biopsies and punch biopsies on the same date. In total, 27 patients (23.7%) underwent the procedure on the screening day, with 14 (48.3%) undergoing excisional biopsy and the other 15 (51.7%) undergoing punch biopsy. However, no statistically significant difference (p = 0.1) was observed between the years 2022 and 2023 in the median time from NSCPC to biopsy. The time between the biopsy of lesions identified during the 2022 NSCPC and the date of the surgical procedure for patients with formal indication for resection ranged from 94 to 218 days, with a mean (SD) of 152.8 (40.3) days and a median of 153.0 days (IQR 111.5-183.2). Out of 33 patients referred for surgical procedures, 11 (33.3%) were lost to follow-up and 22 (66.7%) underwent operations and were treated. Among surgical patients, 11 cases (50.0%) waited between 94 and 144 days to complete this stage, while four cases (18.9%) required over 194 days for resolution (Graph 2A). In 2023, however, the time ranged from 12 to 249 days, with a mean (SD) of 125.2 (57.9) days between the two events and a median of 129.0 days (IQR 91-172). A statistically significant difference (p = 0.04) was observed between 2022 and 2023 in the median time from biopsy to surgery. Out of 59 patients referred for surgical procedures, only 33 (55.9%) were operated on, while the remaining 26 (44.1%) were lost to follow-up. Among patients who underwent surgical procedures, seven (21.2%) were cured within 75 days, and for only two (6.1%) did resolution take more than 201 days (Graph 2B).
Data from the 2022 and 2023 NSCPCs were collected for this study to check whether there were any changes in resolution rate due to the application of different measures on each of the 2 years. Most malignant skin neoplasms are known to affect patients of advanced age, especially after the fifth decade of life.8,14 This corroborates the results from the present study, given that 88.6% of patients in the 2022 NSCPC and 92.1% in the 2023 NSCPC were older than 50 years. The largest age groups were 61-70 years (38.6%) in 2022 and 71-80 years (28.9%) in 2023.
Skin cancer is the result of accumulated mutations caused by photodamage, and so the number cellular changes increases for older age groups.15 This explains why the incidence of skin neoplasms is proportional to age.
Skin tumors have been described in the literature as more prevalent among men.6,8 However, more recent studies have shown an inversion of this prevalence, ie, more women are being diagnosed with BCC, SCC, or melanoma.3,14 In the present study, 61.4% of patients in 2022 and 62.3% in 2023 were women, in line with the epidemiology found in other recent studies. One hypothesis for this inversion in prevalence is that tanned skin has come to be valued aesthetically in recent decades, making it a standard of beauty sought after by women. This attitude has led to the dissemination of outdoor activities and to the exposure of larger areas of the skin to UV radiation.16,17 An additional factor that might explain this change in incidence is the greater resistance among men to seek health care services. Moreover, women generally pay more critical attention and worry more about their own health.18,19
In terms of patient phototype, most (75.0% in 2022 and 81.6% in 2023) had low Fitzpatrick phototypes (1 to 3). In 2022 and 2023, only 11.4% and 6.1%, respectively, were classified as Fitzpatrick 4 and 5. This finding is in line with expectations, given that the risk of developing skin carcinomas is 10 to 20 times higher for light skin compared to dark skin.20,21 This can be explained by the fact that a low phototype is a risk factor for developing skin cancer, given the lower amount of melanin (a pigment found in the epidermis), which in turn provides less protection against ultraviolet radiation, responsible for cancerous mutations.
In 2022, the most prevalent types of lesions among participants were skin neoplasms and their precursors. BCC accounted for 44.6% of lesions, followed by AK (17.8%) and SCC (12.5%). Melanoma accounted for less than 2.0% of cases. These findings are in line with epidemiological data from various regions of Brazil and other countries, in addition to reflecting the same profile observed in NSCPCs in other Brazilian cities.4,5,6,14 On the other hand, in 2023, most lesions (32.3%) diagnosed in pathological examination were non-neoplastic benign conditions. Meanwhile, several patients with suspected skin neoplasms had other benign conditions, leading to the discharge of 41.3% of patients who underwent biopsies. It should be noted that lesions outnumber participants because some patients had more than one lesion.
In 2023, the largest share of lesions consisted of non-neoplastic conditions, totaling 41 cases (32.2%), followed by BCC, with 29 lesions (22.8%), and SCC, with 12 cases (9.4%). That same year, no pigmented lesion suggestive of melanoma was diagnosed. In terms of lesion topography, the head region was the most affected (49.1% in 2022 and 45.2% in 2023), followed by the limbs (24.6% in 2022 and 25.8% in 2023), and finally the trunk (21.1% in 2022 and 23.4% in 2023). This may be explained by the fact that the face is less well-protected and more photoexposed, while the trunk often remains covered by clothing most of the time, blocking UV radiation.14,22
In terms of previous personal history of skin cancer, considering only the year 2022, 47.7% of participants denied any personal history of skin neoplasms. However, it should be noted that the field "personal history" was left blank in a significant number of records (22.7%), indicating the item is often ignored or forgotten by health care professionals. In other studies, the variable was also hard to analyze due to improperly filled survey forms.23 Given these facts, the correlation between personal history of skin cancer and outcomes could not be properly assessed. In the comparative analysis between the 2022 and 2023 NSCPCs, there was an increase in indications for continued investigation of suspected lesions (clinical follow-up or biopsy), with an added 70 patients (159.1%) referred for continued examinations.
In the 2024 study by Grana et al., the annual average linear increase in cases was higher than expected from the 2022 data, indicating an accelerated growth in incidence.6 It is worth questioning the cause for that increase. Possible causes include the population acquiring better information on the issue, leading to more individuals seeking care, or more comprehensive follow-up criteria to prevent any lesion, no matter how low the degree of suspicion, from going unnoticed.
Biopsy is known to be the only method capable of providing a definitive diagnosis of skin cancer.9,10,24 Therefore, cases of suspected neoplasms identified during NSCPC were referred for biopsy in order to confirm the diagnosis and establish the proper management for each case.25
In terms of procedures performed, most patients underwent punch biopsy (81.3% in 2022 and 65.1% in 2023). Excisional biopsy ensures the lesion is fully removed and, when margins are found to be free, patient treatment is considered complete. If melanoma is suspected, excisional biopsy should be performed whenever possible.26 On the other hand, because of their site or size, some lesions must be subjected primarily to punch biopsy, given their potential effects on staging and prognosis.26,27
In the present study, it was also possible to assess rates of patient adherence to outpatient follow-up. A large number of participants were lost to follow-up, either for failing to visit outpatient services or for not reporting to the services to which they had been referred. Biopsies from lesions examined during the 2022 NSCPC began to be performed in January 2023, and were given high priority compared to new referrals to the FMJ outpatient dermatology service. Even so, 14.0% of patients were lost to follow-up at the first stage of the investigation and failed to attend their scheduled biopsies.
During the 2023 NSCPC, new measures were implemented in an attempt to shorten the time between suspicion and resolution. Unlike what happened 1 year earlier, the choice was made to begin performing biopsies on the same day as the NSCPC, which likely contributed to the significant reduction in absences on the day of the biopsy, with that number falling to just 4.4% of patients. In addition, in order to shorten the interval between biopsy and curative surgery, other medical specialties (minor surgery, head and neck surgery, thoracic surgery, and plastic surgery) as well as the medical staff at FMJ helped perform the procedures, consequently contributing to the shorter time to cure.
Regarding time between NSCPC and lesion biopsy, in 2022, the mean interval between events was approximately 50 days, and in 2023 that average fell to approximately 40 days. However, the medians were the same, indicating there was no statistically significant difference between the 2 years. Out of all patients with formal indication for surgical procedures, 33.3% did not attend their scheduled procedure in 2022, as did 44.1% in 2023. As well as showing poor adherence to the treatment plan, these data reveal one of the difficulties faced in the present study.
The mean time between biopsy and curative surgery, in 2022, was approximately 153 days, falling to approximately 123 days in 2023, indicating an improvement over the previous year. Although the maximum time was higher in 2023 (249 days) than in 2022 (218 days), the 24-day reduction in median time between the two events was statistically significant, indicating the new method adopted for the 2023 NSCPC was more effective. The literature does not provide a set period between cancer detection and performance of curative procedures. However, several studies highlight the importance of speedy resolution in order to halt disease progress, prevent metastases, avoid deformities, and lower treatment costs.5,9,10,28 The progression time of in situ BCC and SCC to their invasive form is, on average, 2 to 5 years. However, the tumor may present with a more rapid and aggressive growth,28,29 and it may also not be possible to determine exactly when the lesion first started. Therefore, it is indicated that curative therapy begin as soon as possible.
When assessing total loss to follow-up between the 2022 (38.6%) and 2023 NSCPCs (27.2%), we find that despite the rate remaining high, there was an 11.4% decrease, showing higher rates of patient adherence to treatment plans. Based on other studies, hypotheses that might justify absences include lack of transportation due to impaired mobility or poor financial conditions, forgotten appointments, and the long wait period to problem resolution. These situations deserve attention and the development of social services policies, given that absenteeism leads to delayed and postponed diagnosis and treatment.30
While surgery is the first-line therapy for definitive treatment of skin tumors because of its lower rate of recurrence, there are other therapeutic resources for surface BCC in low-risk areas.8-10,12,24,31 Ablative surgical methods and topical therapies (imiquimod or 5-fluorouracil) may be used, either combined or in sequence.32,33 However, between 25% and 75% of patients treated with these alternative methods require retreatment within 12 months due to field cancerization and the onset of new lesions. Therefore, surgical treatment should be adopted whenever possible.33 Given these facts, and to ensure the needs of each individual patient would be met, during the 2022 NSCPC, clinical follow-up with topical therapy (5-fluorouracil) was chosen for a single patient, given their advanced age, multiple comorbidities, and consequent short life expectancy. In 2023, the same treatment plan was adopted for five patients, again for these reasons.
This research is subject to at least two limitations. The first is that the study data do not include a sample representative of all Brazilian cities and states, comprising only participants from the city of Jundiaí during the 2022 and 2023 NSCPCs. This means the data cannot be generalized. However, the epidemiological data obtained during the events are in line with the studies found in the references. Second, despite attempts to contact patients lost to follow-up, it was not possible to determine precisely why treatment was abandoned, which might interfere with the accuracy of the outcome analysis. Although the exact reason for participant withdrawal remains unknown, it can be observed that with the changes implemented in the 2023 NSCPC, enabling faster biopsies and subsequent curative surgeries, the absenteeism rate was lowered efficiently.
Regardless of their limitations, the data from this study allow us to conclude that, although NSCPC is a valuable initiative for the identification of lesions suspected to be early-stage neoplastic lesions and skin neoplasms, its impact on reducing morbidity and mortality has yet to reach its full potential. For various reasons, time between diagnosis and case resolution is noticeably longer than the timelines recommended in the literature. Therefore, enhanced efficiency in performing biopsies and surgical procedures, alongside greater patient adherence to treatment, is needed. It should be noted that the improvements implemented in the 2023 NSCPC led to reduced time to cure and more rigorous and successful patient follow-up. Although the NSCPC methodology for combating skin cancer remains distant from an optimal standard, the pattern changes observed in this study and similar studies allow us to consider additional measures that may bring NSCPC closer to achieving excellence.
Isabella Melo Pompei
ORCID: 0000-0001-9438-1163
Statistical analysis; Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature; Critical revision of the manuscript
Célia Antônia Xavier de Moraes Alves
ORCID: 0000-0002-8421-8837
Approval of the final version of the manuscript; Conception and design of the study; Effective participation in the conduct of the study; Critical review of the literature; Critical revision of the manuscript
Annamaria Piovezan Lorenção
ORCID: 0009-0001-6094-8595
Statistical analysis; Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical revision of the manuscript
Bruna Mendes Almeida
ORCID: 0000-0002-0804-5401
Approval of the final version of the manuscript; Conception and design of the study; Critical review of the literature; Critical revision of the manuscript
Juliana Arêas de Souza Lima Beltrame Ferreira
ORCID: 0000-0001-7338-3442
Approval of the final version of the manuscript; Conception and design of the study; Effective participation in the conduct of the study; Critical revision of the manuscript
Luciano Melo Pompei
ORCID: 0000-0001-7084-037X
Statistical analysis; Acquisition, analysis and interpretation of data; Critical revision of the manuscript
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424.
2. Instituto Nacional de Câncer. Estimativa 2020: incidência de câncer no Brasil. Rio de Janeiro: Instituto Nacional de Câncer; 2019.
3. Instituto Nacional de Câncer. Estimativa 2023: incidência de câncer no Brasil. Rio de Janeiro: Instituto Nacional de Câncer; 2022.
4. Pessoa DL, Ferreira LP, Silva RS, Teixeira FFN, Abreu CB, Silva EHO, et al. Analysis of the epidemiological profile of non-melanoma skin cancer in the state of Roraima in the period from 2008 to 2014. Braz J Hea Rev. 2020;3(6):18577-90.
5. Sociedade Brasileira de Dermatologia. Data analysis of the Brazilian Society of Dermatology skin cancer prevention campaign, 1999 to 2005. An Bras Dermatol. 2006;81(6):533-9.
6. Grana AG, Gonçalves HS, Barcaui CB, Talhari C, Miot HA. Trends on detecting malignant skin neoplasms during the national campaigns of skin cancer prevention (2000-2023). An Bras Dermatol. 2024;99(6):946-50.
7. Eufrásio LS, Lucena BCM, Almeida DKFH, Lima ESG, Souza KWDD, Silva APS, et al. Educação em saúde com campanhas nacionais de conscientização: porque toda informação importa! Julho a dezembro. Santa Cruz (RN): FACISA; 2022.
8. Rivitti EA. Dermatologia de Sampaio e Rivitti. 4th ed. São Paulo: Grupo a Educação; 2018. 1648 p.
9. National Comprehensive Cancer Network. Squamous cell skin cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®); 2022.
10. National Comprehensive Cancer Network. Basal cell skin cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®); 2022.
11. Cestari MEW, Zago MMF. Cancer prevention and health promotion: a challenge for the 21st century. Rev Bras Enferm. 2005;58(2):218-21.
12. Rojas KD, Perez ME, Marchetti MA, Nichols AJ, Penedo FJ, Jaimes N. Skin cancer: primary, secondary, and tertiary prevention. Part II. J Am Acad Dermatol. 2022;87(2):271-88.
13. Gill PS, Tattersall, MHN. Rastreamento e detecção precoce. In: Love RR, Editor. Manual de oncologia clínica. 6th ed. São Paulo: Fundação Oncocentro; 1999. p.117-38.
14. Oliveira TP, Andrade HD, Pegas JR, Bechara CS. Prevalence of pathological diagnoses and epidemiological profile of patients with non-melanoma skin cancer suspicious lesions. Surg Cosmet Dermatol. 2021;13:e20210031.
15. Wright CY, du Preez DJ, Millar DA, Norval M. The epidemiology of skin cancer and public health strategies for its prevention in southern Africa. Int J Environ Res Public Health. 2020;17(3):1017.
16. Keesling B, Friedman HS. Psychosocial factors in sunbathing and sunscreen use. Health Psychol. 1987;6(5):477-93.
17. Arthey S, Clarke VA. Suntanning and sun protection: a review of the psychological literature. Soc Sci Med. 1995;40(2):265-74.
18. Levorato CD, Mello LM, Silva AS, Nunes AA. Factors associated with the demand for health services from a gender-relational perspective. Cien Saude Colet. 2014;19(4):1263-74.
19. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa nacional de saúde: 2019: informações sobre domicílios, acesso e utilização dos serviços de saúde: Brasil, grandes regiões e unidades da federação / IBGE, Coordenação de Trabalho e Rendimento. Rio de Janeiro: IBGE; 2020. 85p.
20. Roewert-Huber J, Lange-Asschenfeldt B, Stockfleth E, Kerl H. Epidemiology and aetiology of basal cell carcinoma. Br J Dermatol. 2007;157(Suppl 2):47–51.
21. Lear W, Dahlke E, Murray CA. Basal cell carcinoma: review of epidemiology, pathogenesis, and associated risk factors. J Cutan Med Surg. 2007;11(1):19–30.
22. Souza CFD, Menegotto PF, Shibue JRT, Thomé EP, Schmitt JV, Tarlé RG. Topography of basal cell carcinoma and their correlations with gender, age and histologic pattern: a retrospective study of 1042 lesions. An Bras Dermatol. 2011;86(2):272-7.
23. Teixeira MA, McManus C, Pinheiro AMC, Abbud CBB, Fernandes AGO, Santos LRS, et al. Social epidemiological profile of patients with suspected skin cancer in the Federal District, Brazil. Rev Enferm Atual Derme. 2023;97: e023110.
24. Lim JL, Asgari M. Cutaneous squamous cell carcinoma (cSCC): clinical features and diagnosis. UptoDate; 2023.
25. Alguire PCA, Mathes BM. Skin biopsy techniques. UptoDate; 2023.
26. Blakeman JM. The skin punch biopsy. Can Fam Physician. 1983;29:971-4.
27. Pickett H. Shave and Punch Biopsy for Skin Lesions. Am Fam Physician. 2011;84(9):995-1002.
28. John SM, Trakatelli M, Gehring R, Finlay K, Fionda C, Wittlich M, et al. Consensus report: recognizing non- melanoma skin cancer, including actinic keratosis, as an occupational disease - a call to action. J Eur Acad Dermatol Venereol. 2016;30(Suppl 3):38-45.
29. Rigel DS, Stein Gold LF. The importance of early diagnosis and treatment of actinic keratosis. J Am Acad Dermatol. 2013;68(1 Suppl 1):S20-7.
30. Bittar OJNV, Magalhães A, Martines CM, Felizola NBG, Falcão LHB. Absenteeism in outpatient care specialties in São Paulo. Boletim Epidemiológico Paulista. 2016;13(152):19-32.
31. Urun YG, Can N, Bagış M, Solak AA, Urun M. Adequacy of surgical margins, re-excision, and evaluation of factors associated with recurrence: a retrospective study of 769 basal cell carcinomas. An Bras Dermatol. 2023;98(4):449-59.
32. Work Group; Invited Reviewers; Kim JYS, Kozlow JH, Mittal B, Moyer J, et al. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540-59.
33. Smit JV, Sévaux RGL, Blokx WAM, Van De Kerkhof PCM, Hoitsma AJ, Jong EMGJ. Acitretin treatment in (pre) malignant skin disorders of renal transplant recipients: histologic and immunohistochemical effects. J Am Acad Dermatol. 2004;50(2):189-96.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}