


Luiz Roberto Dal Bem Pires Júnior; Carlos Augusto Silva Bastos; Rafaella Castilho; Waleska Ramos Alvim Lescowicz; Karina Fernanda Bortoloto Predolin; Laurenlisiê Lourega Heitling Brittes
Funding: None.
Conflict of interest: None.
Submitted on: 11/05/2024
Final decision: 01/28/2025
How to cite this article: Pires Júnior LRDB, Bastos CAS, Castilho R, Lescowicz WRA, Predolin KFB, Brittes LLH. Reconstruction of the medial malar region and lower eyelid with a McGregor flap after resection of pigmented basal cell carcinoma. Surg Cosmet Dermatol. 2025;17:e20250420.
Basal cell carcinoma is the most common skin cancer, most often found in the head and neck region. We present the case of a 47-year-old male patient with pigmented basal cell carcinoma in the right medial malar region. After confirmatory biopsy, the lesion was excised with a 5 mm safety margin, extending to the lower eyelid. Reconstruction was performed using the McGregor flap, a technique that enables effective tissue advancement with minimal tension, minimizing the risk of complications. The patient had an uncomplicated recovery with satisfactory oncologic, aesthetic, and functional outcomes, demonstrating the technique's efficacy in complex periocular reconstructions.
Keywords: Carcinoma, Basal Cell; Surgical Flaps; Dermatology; Surgical Oncology; Face; Skin Neoplasms
Basal cell carcinoma (BCC) is the most common malignant neoplasm in the world, accounting for most cases of skin cancer.1 Nodular BCC has the highest prevalence, and is often found in the head and neck region.2 In addition, the incidence of BCC is increasing annually—in Brazil, according to estimates from the National Cancer Institute, for the 2023-2025 period, 101,920 new cases in males and 118,520 new cases females are expected.3 Although BCC has low metastasis potential (0.03%), it is locally invasive,3 which can compromise structures around the lesion. The pigmented form accounts for only approximately 6% of BCC cases,4 making differential diagnosis with other pigmented lesions, such as intradermal nevus, sebaceous hyperplasia, trichoepithelioma, and melanoma, even more important.5
The malar region is considered one of the most important for facial aesthetics, and is also one of the most affected by BCC. It can be divided into four anatomical subunits: medial, lateral, zygomatic, and buccal. Skin characteristics vary gradually among these subunits.6 The medial portion is limited by the lower eyelid, medial epicanthus, nasofacial sulcus, perialar area, and upper part of the nasogenian sulcus. Its proximity to areas at high risk of complications, such as the lower eyelid, makes surgical planning challenging, requiring techniques that ensure minimal tension, lead to discreet scars that respect the natural lines of the skin, and hide incisions efficiently in such a delicate and heterogeneous region.7
A 47-year-old male patient, with no comorbidities and no personal or family history of skin neoplasms, was referred from primary care due to a reportedly fast-growing pigmented papule measuring approximately 1 cm in the right upper medial malar region (Figure 1). Lesion dermoscopy revealed arborizing vessels, rainbow pattern, gray-blue ovoid nests, and blue globules, consistent with pigmented BCC (Figure 2), as confirmed by incisional biopsy.
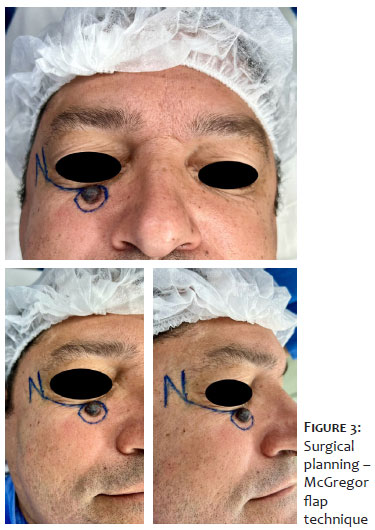
Surgical treatment was planned based on these findings. After lesion resection with a 5 mm safety margin, the surgical wound included the lower eyelid, leading to the choice of performing a McGregor flap reconstruction (Figure 3). The technique consists of a lateral incision following the curvature of the eyelid, which may extend to the area anterior to the preauricular hairline depending on the width of the defect to be covered. In the case of the patient in this report, extending the main incision was not necessary. The curvature of the incision is essential to provide adequate vertical length for the flap.
A Z-plasty was performed at the lateral end of the incision, with defect width corresponding to the central limb of the "'Z." The descending and ascending limbs were of equal length to the central limb and formed a 60-degree angle with it, facilitating flap mobilization. Dissection was performed in the subcutaneous plane, allowing advancement of the flap and its subsequent transposition in the Z-plasty, culminating in closure of the defect after compensation with a Burow's triangle perpendicular to the main incision line. The suture was performed with 5-0 Vicryl and 6-0 Nylon (Figure 4).
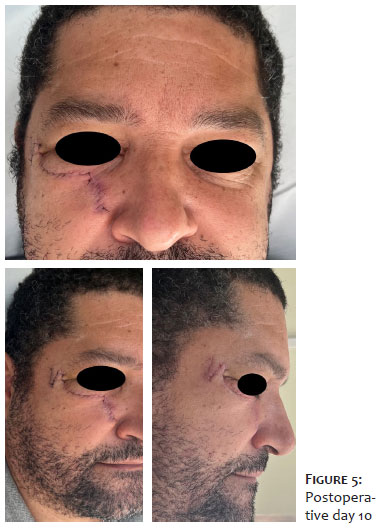
The patient had an uncomplicated recovery with satisfactory functional, oncologic, and aesthetic outcomes (Figures 5 and 6).
In high-risk BCC cases, a category which includes the present case due to its location, the primary treatment options are surgical, with radiation therapy reserved for patients unable to undergo surgical procedures. Standard resection, with surgical margins evaluated by histopathological examination, is a common practice in Brazil. In these procedures, 4 to 6 mm margins, but which can be as wide as 8 mm, are drawn around the visible tumor, with pathologic examination performed subsequently.8
The surgical procedure should follow the principles of oncology, with complete removal of the tumor as its primary goal. However, when planning periocular interventions, considering the preservation of function in order to optimize oncologic, functional, and aesthetic outcomes is key.9
In lower eyelid reconstruction, rotation flaps are traditionally effective given their horizontal vector, which minimizes the risk of postoperative ectropion and canthal distortion.10 Since the lateral rotation skin flap technique for the malar region proposed by Mustardé in 1966, several others have been developed based on medially advancing lateral skin to correct lower eyelid defects. In general, there is skin laxity in the lateral facial region, and this advancement is limited; without measures to reduce flap tension, it tends to return to its original position in the postoperative period.11
In 1973, McGregor introduced a technique to correct lower eyelid defects involving lateral periorbital Z-plasty, enabling medial advancement of the tissues and relieving tension on the advancement flap. This approach represents an excellent alternative within the reconstructive arsenal for complex lower eyelid defects. It was originally indicated for the reconstruction of V-shaped defects involving up to two-thirds of the eyelid width and is applicable to both the lower and upper eyelids. After 15 years applying this technique, McGregor reported favorable surgical outcomes, with high-quality scars and preservation of the natural appearance of the lateral canthus.12 In the present case, this technique was successfully used in the reconstruction of the lower eyelid and medial malar region, resulting in a satisfactory outcome and establishing itself as a valuable option within the surgical arsenal.
Luiz Roberto Dal Bem Pires Júnior
ORCID: 0009-0001-6728-420X
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Carlos Augusto Silva Bastos
ORCID: 0000-0003-0255-2696
Conception and design of the study
Rafaella Castilho
ORCID: 0009-0003-1437-2024
Critical review of the literature; Critical revision of the manuscript
Waleska Ramos Alvim Lescowicz
ORCID: 0000-0002-0106-1097
Critical review of the literature
Karina Fernanda Bortoloto Predolin
ORCID: 0009-0003-2745-7481
Critical revision of the manuscript
Laurenlisiê Lourega Heitling Brittes
ORCID: 0009-0004-9918-087X
Critical review of the literature
1. Kim JYS, Kozlow JH, Mittal B, Moyer J, Olencki T, Rodgers P. Guideline of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540-59.
2. Basset-Seguin N, Herms F. Update in the management of basal cell carcinoma. Acta Derm Venereol. 2020;100(11):adv00140.
3. Instituto Nacional de Câncer (INCA). Estimativa de câncer no Brasil 2023-2025 [Internet]. Disponível em: https://www.gov.br/inca/pt-br/assuntos/cancer/numeros/estimativa/estado-capital/brasil.
4. Cameron MC, Lee E, Hibler BP, Barker CA, Mori S, Cordova M, et al. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol. 2019;80(2):303-17.
5. Kim DP, Kus KJB, Ruiz E. Basal cell carcinoma review. Hematol Oncol Clin North Am. 2019;33(1):13–24.
6. Sanchez FLE. Manejo dos tumores perioculares com cirurgia micrográfica de Mohs. Surg Cosmet Dermatol. 2014;6(4):226-32.
7. Patel BCK. Surgical Eyelid and Periorbital Anatomy. Semin Ophthalmol. 1996;11(2):118-37.
8. National Comprehensive Cancer Network® (NCCN®). Guidelines Version 2.2022; 24 de março de 2022.
9. Cerci FB, Fantini BC. Retalhos e enxertos em cirurgia micrográfica de Mohs. São Paulo: Editora Atheneu; 2022.
10. Harris J, Perez N. Anchored flaps in post-Mohs reconstruction of the lower eyelid, cheek, and lateral canthus: avoiding eyelid distortion. Ophthalmic Plast Reconstr Surg. 2003;19(1):5 - 13.
11. Mustardé JC. The use of flaps in the orbital region. Plast Reconstr Surg. 1970;45(2):146-50.
12. McGregor IA. Eyelid reconstruction following subtotal resection of upper or lower lid. Br J Plast Surg. 1973;26(4):346-54.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}