


Shaimaa Farouk; Eman Tarek; Dalia Hossam; Ahmed Sadek
Financial support: None.
Conflicts of interest: None.
Submitted on: 17/11/2024
Approved on: 16/01/2025
How to cite this article: Farouk S, Tarek E, Hossam D, Sadek A. Topical potassium hydroxide 40% versus trichloroacetic acid 40% in the treatment of plantar warts: a randomized controlled trial. Surg Cosmet Dermatol. 2025;17:e20250423.
INTRODUCTION: Warts are a viral skin condition caused by the human papillomavirus (HPV), which can lead to disfigurement, embarrassment, and frustration. No single treatment has been shown to guarantee complete eradication.
OBJECTIVE: To evaluate and compare the effectiveness of topical potassium hydroxide (KOH) 40% and trichloroacetic acid (TCA) 40% in the treatment of plantar warts, based on clinical and dermoscopic outcomes, as well as to assess side effects and patient satisfaction.
METHODS: An interventional comparative study was conducted involving 33 patients with plantar warts. Lesions were divided into two groups: Group A received topical TCA 40%, and Group B received topical KOH 40%. All patients were evaluated both clinically and through dermoscopy.
RESULTS: Both treatment groups showed statistically significant clinical and dermoscopic improvement (p < 0.001 for both). Complete dermoscopic clearance without recurrence over a 2-month follow-up period was more frequent in the KOH group (88.6%).
CONCLUSION: Topical TCA and KOH were similarly effective. KOH, in particular, proved to be both effective and safe, making it a promising adjunct treatment for plantar warts alongside destructive and immunotherapeutic methods.
Keywords: Papillomaviridae. Warts. Controlled Clinical Trial
Plantar warts are benign skin manifestations caused by human papillomavirus (HPV) infection, most commonly types 1, 4, 57, 60, 63, 65, and 66. The myrmecia-type wart appears as a smooth-surfaced, deep, often inflamed, and tender papule or plaque. These lesions typically develop on the palms or soles, but can also occur near or under the nails, and less frequently on the fingertips. They are characteristically dome-shaped and extend deeper beneath the surface than they appear clinically. Warts are transmitted either through direct person-to-person contact or indirectly via contaminated surfaces. Verruca vulgaris accounts for approximately 70% of all cutaneous warts and occurs primarily in children.1 Skin warts are estimated to affect up to 10% of children and young adults, with the highest incidence between 12 and 16 years of age. This prevalence increases by 50 to 100 times in immunocompromised individuals.2
Spontaneous clearance rates of warts are generally low and require extended periods of time, with reported rates of 23% at 2 months, 30% at 3 months, and 65%-78% after 2 years.3 Cutaneous warts are estimated to affect up to 10% of children and young adults, with the highest incidence between 12 and 16 years of age. This prevalence increases by 50 to 100 times in immunocompromised individuals.2
The primary goals of treatment are to remove the wart without scarring, prevent recurrence — particularly at the same site — and, if possible, induce long-term immunity. Because of the variability of treatment outcomes, multiple therapeutic options, including combination therapies, may be considered. Treatment selection should be based on the size, location, and morphological type of the wart.4 Destructive treatments, including chemical and surgical methods, function by damaging the epithelium and inducing infected cell death, which leads to antigen exposure and presentation,2 thereby potentially triggering an immune response.
Superficial viral destruction can be induced by a variety of agents; however, such treatments may not reach virus-infected cells in the deeper layers of the epidermis. Direct stimulation of the immune system at the site of the wart may enhance the likelihood of an effective immunological response against infected keratinocytes.5 Destructive procedures can be inconvenient, especially for large or multiple warts, as they may leave extensive areas of raw skin that require prolonged healing and carry an increased risk of secondary infection. Consequently, immunotherapy has emerged as a more favorable treatment option for resistant warts. Various agents have been utilized in immunotherapy, including systemic treatments such as H₂ receptor blockers, zinc, and interferons. Intralesional injections of the MMR (measles, mumps, rubella) vaccine, Candida antigen, purified protein derivative (PPD), and Trichophyton skin antigen have also been employed. Additional modalities include auto-implantation and the topical application of imiquimod.
Potassium hydroxide (KOH) solution is a promising treatment for cutaneous warts due to its keratolytic effect and ability to deeply penetrate the skin, resulting in the destruction of virus-infected cells. Its irritant properties may also stimulate an inflammatory response, contributing to wart resolution. KOH is associated with minimal side effects and is inexpensive.6
Trichloroacetic acid (TCA) is a topical destructive agent that induces hydrolysis of cellular proteins, leading to cell death. When applied to the skin, it causes coagulative necrosis of epidermal cells, precipitates proteins, and leads to necrosis of collagen from the papillary to upper reticular dermis. Within a few days, unaffected adnexal structures regenerate the skin, and the necrotic tissue peels away. TCA produces results similar to those of cryotherapy and is effective in treating anal, genital, cervical, and common warts when used at concentrations of 70-80%.3 For common warts, lower concentrations (10-30%) are typically used. TCA offers the advantage of having no systemic toxicity, though local side effects such as burning, discomfort, hyperpigmentation, and, less commonly, scarring may occur.7
The aim of this study was to evaluate and compare the effectiveness of topical TCA 40% versus topical KOH 40% in the treatment of plantar warts, both clinically and dermoscopically, and to report on associated side effects and patient satisfaction.
This interventional comparative study included 33 patients aged over 10 years. Each patient had two plantar warts: one lesion was treated with KOH and the other with TCA. Patients were excluded if they had autoimmune diseases, symptoms suggestive of inflammation or infection, were receiving immunosuppressive therapy, were pregnant or lactating, or had received wart treatment in the preceding months.
Following approval by the Research Ethics Committee of the Central Directorate for Research and Health Development, Egyptian Ministry of Health (IORG0005704/IRB0000687; Com. No./Dec. No: 7-2023/31), the study was conducted in the outpatient procedures department of the Cairo Hospital of Dermatology and Venereology, from December 2022 to July 2023. Written informed consent was obtained from each participant or from a parent/guardian in cases involving minors under 18 years of age.
Patients underwent a complete medical history to document name, age, sex, address, contact information, duration of the warts, and any previous therapeutic attempts and their outcomes. This was followed by a thorough clinical examination of the warts4 to record their size, location, and surface characteristics. Each patient had two plantar warts: one lesion was treated with KOH and the other with TCA. The lesions were randomly assigned into two groups: Group A (33 lesions) received topical TCA 40%, and Group B (33 lesions) received topical KOH 40%. A piece of cotton soaked with the respective solution was gently applied to each wart and left in place for 1-2 hours. Both treatments were administered on the same day.
Treatment sessions were performed weekly until complete improvement or for a maximum of six sessions. All patients were evaluated through both clinical and dermoscopic assessments. Treatment efficacy was evaluated based on the following criteria:
Photographs were taken at baseline, after every two treatment sessions, and two months following the final treatment session. All images were evaluated by two dermatology consultants who were blinded to patient identity and treatment details. The improvement of plantar warts was assessed using a three-point scale: i) non-responder (0): <25% improvement; ii) mild improvement (1): 25-75% improvement; and iii) complete improvement (2): >75% improvement. Images were captured using a smartphone camera (Samsung A7), featuring a 24-megapixel primary sensor, an 8-megapixel wide-angle sensor, and a 5-megapixel depth sensor.
Dermoscopic findings included thrombosed blood vessels interrupting the cutaneous dermatoglyphics. A hand-held dermoscope (DermLite DL4, 3Gen, USA) was used for examination. Evaluations were performed at baseline, after every two treatment sessions, and 2 months after the final session. Two inde-pendent dermatologists, blinded to treatment details, assessed the images using the following three-point scale: i) non- responder (0); ii) mild improvement (1); and iii) complete improvement (2).
Patient satisfaction was evaluated after the final treatment session using a 6-point scale ranging from 0 (not satisfied) to 5 (very satisfied).
Adverse effects were monitored and included post-inflammatory hyperpigmentation, hypopigmentation, bullae, erythema, infection, and scarring. Patients who experienced adverse effects received detailed post-treatment wound care instructions and were prescribed a topical antiseptic solution and antibiotic cream as needed.
Data were collected, edited, coded, and entered using IBM SPSS Statistics for Windows, version 23 (IBM Corp., Armonk, N.Y., USA). Quantitative data were presented as the mean, standard deviation (SD), and range for parametric variables, or as the median and interquartile range (IQR) for non-parametric variables. Categorical variables were expressed as frequencies and percentages.
The chi-square test was used to compare qualitative variables between groups. For quantitative data, the independent t-test was applied to compare two groups with parametric distribution, while the Mann-Whitney U test was used for non-parametric comparisons.
A margin of error of 5% was accepted, and 95% confidence interval. The following thresholds were used to interpret p-values:
Not significant: p > 0.05
Significant: p < 0.05
Highly significant: p < 0.01
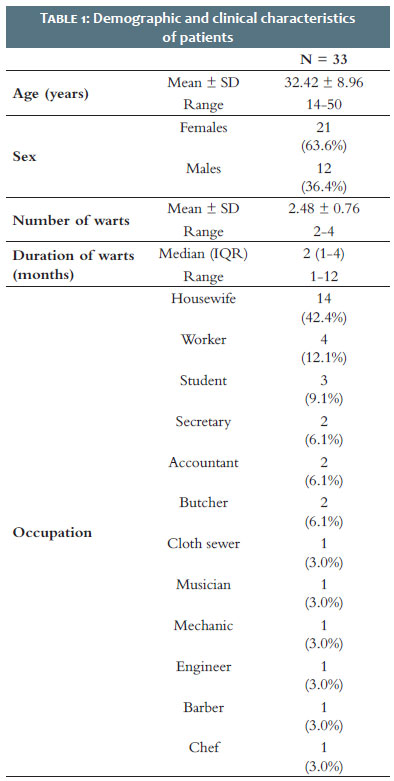
The study included 33 individuals: 12 men (36.4%) and 21 women (63.6%), all with multiple plantar warts. Participants' ages ranged from 14 to 50 years, with a mean age of 32.42 ± 8.96 years. The duration of warts ranged from 2 to 4 months, with a mean of 2.48 ± 0.76 months (Table 1).
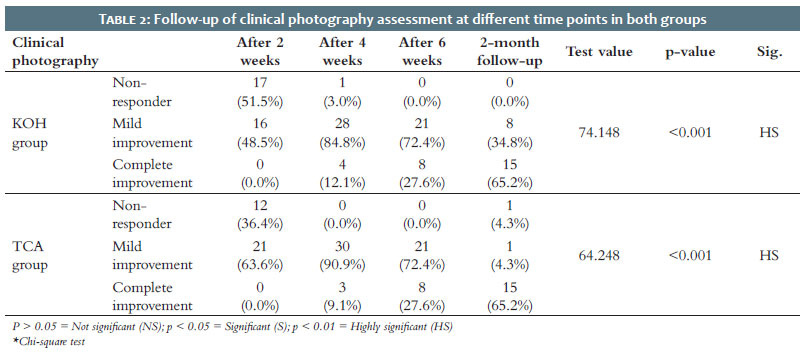
A statistically significant improvement in clinical photographic assessment was observed throughout the treatment sessions in both the KOH and TCA groups, with p-values < 0.001 and 0.001, respectively (Table 2).
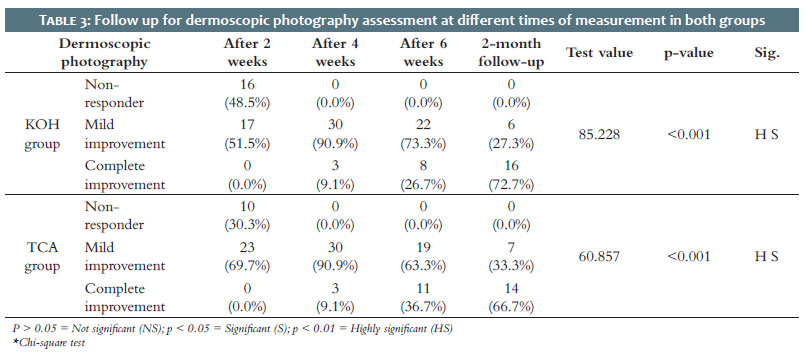
Dermoscopic photographic assessment also revealed statistically significant improvement during treatment in both groups, with p-values < 0.001 for each (Table 3).
Complete dermoscopic clearance of warts without recurrence during the 2-month follow-up period was achieved in 88.6% of the KOH group, compared to 66.7% of the TCA group.
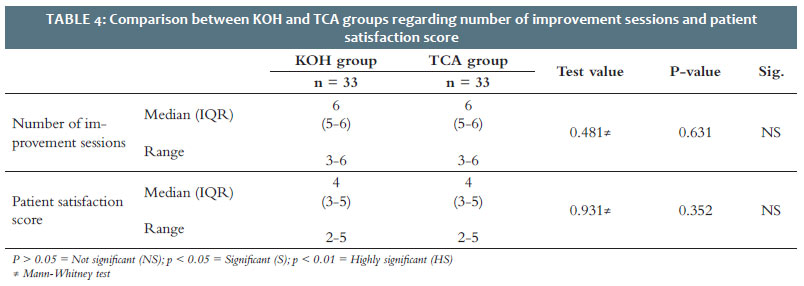
There was no statistically significant difference between the two groups in terms of the number of sessions required for improvement or patient satisfaction scores. Both groups had a median of 6 sessions (IQR 3-6) (Table 4).
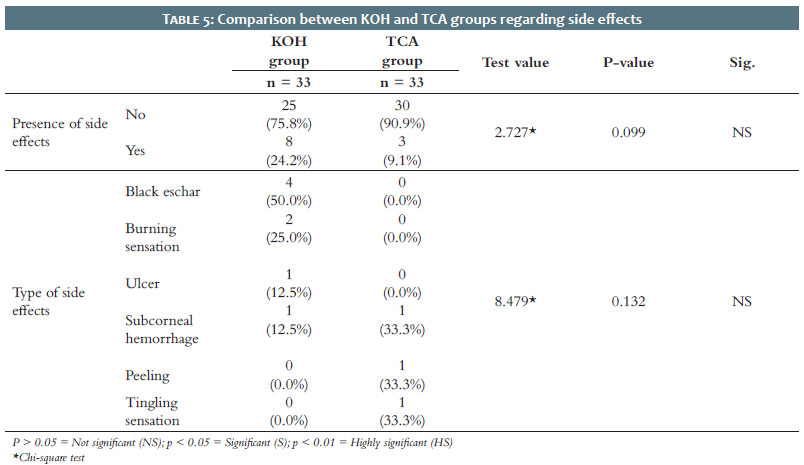
No statistically significant differences were found between the groups regarding the occurrence or types of side effects, with p-values of 0.099 and 0.132, respectively. Side effects were reported in 9.1% (3 patients) in each group. In the KOH group, the side effects included burning sensation (66.7%, 2 patients) and subcorneal hemorrhage (33.3%, 1 patient). In the TCA group, side effects included ulceration, subcorneal hemorrhage, and peeling—each reported in 33.3% of the affected patients (Table 5).
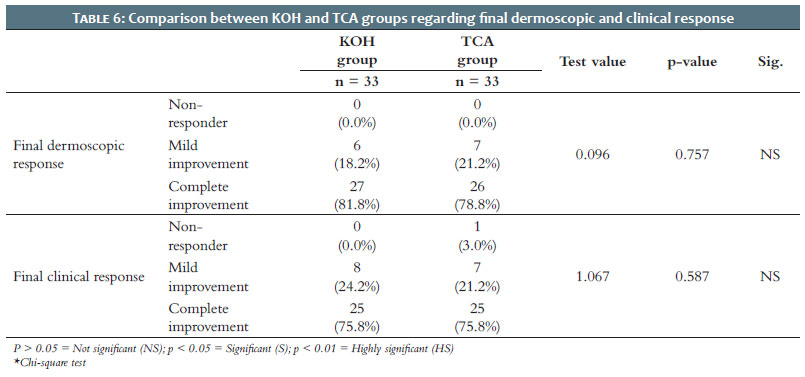
No statistically significant difference was found between the two groups regarding final dermoscopic and clinical responses. Both groups showed similar rates of mild clinical improvement: 24.2% in the KOH group and 21.2% in the TCA group. Regarding final dermoscopic response, complete improvement was observed in 81.8% of the KOH group and 78.8% of the TCA group (Table 6).
A highly statistically significant correlation was found between dermoscopic and clinical assessments in the KOH group (p = 0.007). A statistically significant correlation was also observed in the TCA group (p = 0.022).
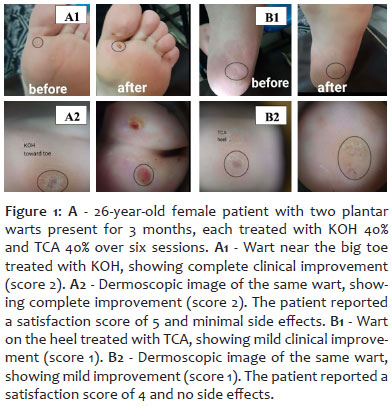
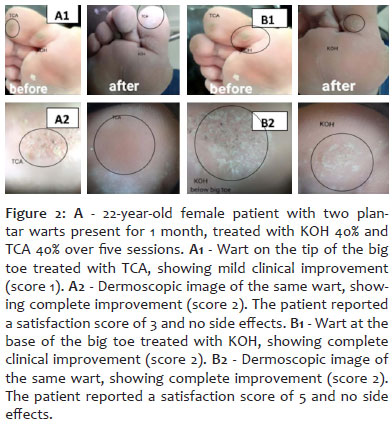
Final dermoscopic and clinical outcomes are illustrated in Figure 1 and Figure 2.
HPV is the primary cause of common warts, which often affect children and immunocompromised individuals. Warts can be disfiguring, leading to embarrassment and frustration, which motivates most patients to seek treatment.8
Although various treatment options are available — including topical medications, cryotherapy, laser therapy, photodynamic therapy, surgical excision, and immunotherapy — no single method guarantees complete eradication or prevention of recurrence.9
Due to their destructive nature, many of these treatments can leave scars. Less invasive approaches, while minimizing scarring, may produce suboptimal responses or increase the likelihood of recurrence, particularly in patients with large or multiple lesions. For these reasons, immunotherapy has gained increasing attention and popularity.10
KOH has been investigated for its efficacy and tolerability in wart treatment. It has been shown to be a safe and effective option for treating plane warts. Its keratolytic properties promote the destruction of virus-infected cells, facilitating wart resolution.11
TCA is a topical destructive agent that induces cell death through the hydrolysis of cellular proteins. When applied to the skin, TCA causes protein precipitation, coagulative necrosis of epidermal cells, and collagen necrosis extending from the papillary to the upper reticular dermis. Within a few days, the epidermis regenerates from adnexal structures that were unaffected by the chemical injury, and the necrotic layers peel off. At various concentrations, TCA has been shown to be effective in treating anal, genital, cervical, and common warts, with response rates comparable to those achieved with cryotherapy.11
The aim of this study was to evaluate and compare the effectiveness of topical TCA 40% and KOH 40% in the treatment of plantar warts, using both clinical and dermoscopic assessments, while also documenting any side effects and levels of patient satisfaction.
This interventional comparative study included 33 patients over the age of 10 with multiple plantar warts. Exclusion criteria included autoimmune disease, signs of active inflammation or infection, use of immunosuppressive therapy, pregnancy or lactation, and receipt of wart treatment in the preceding months.
Patients underwent a complete medical history, including documentation of name, age, sex, address, contact information, duration of warts, and any previous therapeutic attempts and their outcomes. A thorough clinical examination of the warts was then performed to assess their size, location, surface characteristics, and number. Each patient's lesions were randomly divided into two groups: Group A received topical TCA 40%, and Group B received topical KOH 40%. The topical solutions were applied using a cotton swab and left in place for 1-2 hours. Both treatments were administered on the same day.
Treatment sessions were conducted weekly until complete improvement or for a maximum of six sessions. All patients were evaluated through clinical and dermoscopic assessments. Dermoscopic findings included the presence of thrombosed blood vessels interrupting the cutaneous dermatoglyphics.
Assessments were performed at baseline, after every two sessions, and two months after the final treatment session, using a three-point scale: i) non-responder (0); ii) mild improvement (1); and iii) complete improvement (2).
Among the studied patients with plantar warts, 63.6% were female and 36.4% were male.
Similarly, gender distribution in a study conducted by Hanif et al. (2022) showed that 48.65% of participants were male and 51.35% were female, all presenting with plantar warts.11 In our study, participant age ranged from 14 to 50 years, with a mean ± SD of 32.42 ± 8.96 years. This was comparable to the findings of Al Mokadem et al. (2022), who reported an age range of 18 to 50 years in their study.12
No statistically significant difference was observed between the two groups regarding final dermoscopic and clinical responses. Based on final dermoscopic evaluation, complete improvement was recorded in 81.8% of the KOH group and 78.8% of the TCA group.
Complete dermoscopic clearance of warts without recurrence during the 2-month follow-up period was achieved in 88.6% of patients in the KOH group, compared to 66.7% in the TCA group.
Both groups showed statistically significant improvement in clinical and dermoscopic assessments across successive treatment sessions, with p-values of <0.001 for the KOH group and 0.001 for the TCA group.
The time required for complete wart resolution ranged from 3 to 6 weeks. Patient satisfaction scores ranged from 2 to 5, with a median of 4 in both the KOH and TCA groups.
No statistically significant difference was observed between the KOH and TCA groups regarding the incidence and type of side effects, with p-values of 0.099 and 0.132, respectively.
Since there were no significant differences between the KOH- and TCA-treated groups in terms of treatment response, number of sessions required for clearance, or patient satisfaction, these findings suggest that KOH has a therapeutic effect comparable to that of TCA. Both agents appear capable of achieving similar clinical outcomes.
Similarly, Khan et al. (2017) enrolled 100 patients with palmoplantar warts and treated them with 10% topical KOH applied once daily at night. The efficacy was comparable for both palmar and plantar warts (p = 0.85). Notably, a significantly better outcome (p = 0.04) was observed in patients with a single lesion, with 90.91% (20 out of 22) showing complete clearance. The study concluded that 10% KOH is highly effective for the treatment of palmoplantar warts, especially in cases involving a single lesion.13
Likewise, Bodar et al. (2020) reported that TCA needling was an effective technique for treating palmoplantar warts in a study involving patients aged 4 to 50 years. After obtaining informed consent, participants received weekly applications of 100% TCA followed by needling using an insulin syringe. Total wart clearance was achieved within a minimum of three weeks and a maximum of eight weeks.11,14
In contrast, Hanif et al. (2022) compared 148 cases of palmoplantar warts in patients of both sexes, aged 3 to 12 years. The participants were divided into two groups of 74 each: Group A received topical TCA 35%, and Group B received topical KOH 10%. Efficacy was observed in 28 cases (37.84%) in Group A and 57 cases (77.03%) in Group B. Group B demonstrated significantly superior results compared to Group A (p = 0.0001).11 According to their findings, 10% KOH was substantially more effective than 35% TCA, even after accounting for confounding variables such as age, site, size, and duration of the warts. These results suggest that higher concentrations of TCA may be required to achieve clearance of plantar warts, whereas lower concentrations of KOH can be equally effective.
Similarly, Attia et al. (2020) reported that both KOH 30% and TCA 30% were equally effective in the treatment of plane warts, with no statistically significant differences between the groups at the end of the treatment period or during follow-up. The study included 60 patients with plane warts, divided into two groups: Group A (TCA) and Group B (KOH). Complete clearance was observed in seven patients (23.3%) in each group. After 12 weeks, partial improvement was achieved in 15 patients (50%) in Group A and 16 patients (53.3%) in Group B. Non-response was noted in eight patients (27.6%) in Group A and seven patients (23.3%) in Group B.15
In contrast, Al-Hamdi et al. (2012) reported that topical KOH at lower concentrations (5% and 10%) provided a safe, effective treatment for plane warts, with minimal adverse effects. The study involved 250 patients with plane warts, divided into two equal groups based on age and sex. Group A received topical KOH 5% once nightly, while Group B received KOH 10% once nightly. By the end of the second week, complete wart clearance was observed in 9.3% of patients in Group A and 66.3% in Group B. At the end of the fourth week, complete response was achieved in 82.1% of Group B and 80.3% of Group A. Reported side effects included itching, burning sensation, erythema, and transient dyspigmentation, affecting 77.6% of patients in Group A and 90.5% in Group B. During the 3-month follow-up, recurrence rates were low in both groups: 5.8% in Group A and 5.1% in Group B.16
Patient-related variables such as age, gender, occupation, and wart location did not significantly influence treatment response in any of the study groups. However, larger-scale studies are warranted to confirm these findings.
In our study, side effects were minimal. Burning sensation was the most frequently reported adverse effect in the KOH group, consistent with findings by Attia et al. (2020).15
The limitations of this study include the small sample size, the lack of long-term post-treatment follow-up, and the absence of correlation between long-term response and treatment outcome.
Both TCA and KOH demonstrated comparable effectiveness in the treatment of plantar warts. Notably, patients with a wart duration of less than 6 months showed a better therapeutic response.13 Burning sensation was more frequently reported in the KOH group, along with pain and black eschar formation. Overall, topical TCA 40% and KOH 40% are effective and moderately safe options for the treatment of plantar warts and may be considered viable therapeutic alternatives.
Further prospective studies with larger sample sizes are recommended to validate the findings.
Additional investigations using different concentrations of both TCA and KOH are needed to assess their impact on clinical response in patients with plantar warts.
Future studies should include detailed documentation of side effects after each individual treatment session.
Shaimaa Farouk
Approval of the final version of the manuscript, conception and design of the study, preparation and writing of the manuscript, effective participation in the conduct of the study, intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied.
Eman Tarek
Statistical analysis, acquisition, analysis and interpretation of data; intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied.
Dalia Hossam
Approval of the final version of the manuscript, conception and design of the study, critical review of the literature.
Ahmed Sadek
Approval of the final version of the manuscript, intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, critical revision of the manuscript.
1. Leto MGP, Porro AM, Santos Júnior GF, Tomimori J. Human papillomavirus infection: etiopathogenesis, molecular biology and clinical manifestations. An Bras Dermatol 2011;86(2):306–17.
2. Kaur GJ, Brar BK, Kumar S, Brar SK, Singh B. Evaluation of the efficacy and safety of oral isotretinoin versus topical isotretinoin in the treatment of plane warts: a randomized open trial. Int J Dermatol. 2017;56(12):1352–8.
3. Hsu VM, Aldahan AS, Tsatalis JP, Perper M, Nouri K. Efficacy of Nd: YAG laser therapy for the treatment of verrucae: a literature review. Lasers Med Sci 2017;32(5):1207–11.
4. Al Aboud AM, Nigam PK. Wart. Treasure Island (FL): StatPearls Publishing; 2017.
5. Sterling JC, Gibbs S, Haque Hussain SS. British Association of Dermatologists' guidelines for the management of cutaneous warts 2014. Brit J Dermatol. 2014;171(4):696–712.
6. Kandil A, Farag F, Nassar A, Amer RF. Evaluation of topical potassium hydroxide in the treatment of nongenital warts. Journal of the Egyptian Women's Dermatologic Society 2016;13:159–64.
7. Pezeshkpoor F, Banihashemi M, Yazdanpanah MJ. Comparative study of topical 80% trichloroacetic acid with 35% trichloroacetic acid in the treatment of the common wart. J Drugs Dermatol 2012;11(11):e66-9.
8. Kaur S, Kumar S, Brar B. Study of socio-demographic details of verruca vulgaris patients-an institutional based study. J of Adv Medical Dental Sci Res. 2017;5(3):36-9.
9. Graham S, Faizo AA. Control of human papillomavirus gene expression by alternative splicing. Virus Res. 2017;231:83-95.
10. Mitra A, MacIntyre DA, Lee YS. Cervical intraepithelial neoplasia disease progression is associated with increased vaginal microbiome diversity. Sci Rep. 2015;5:1–11.
11. Hanif N, Tahir R, Hassan T. Comparing Efficacy of 35% Trichloroactetic acid versus 10% potassium hydroxide in topical treatment of palmoplantar warts in patients upto 12 years of age. Pak J Medical Health Sci. 2022;16:261.
12. Al Mokadem SMAEF, Elfazani SEA, Khater MH. Intralesional methotrexate versus curettage and application of 100% trichloroacetic acid in planter warts. Egypt J Hosp Med 2022;89:5345–9.
13. Khan S, Zeeshan H. Efficacy of 10% KOH in palmoplantar warts. Pak J Medical Health Sci. 2017;11(2):553-5.
14. Bodar P, Agarwal P, Saikia S. Evaluating the efficacy of 100% trichloroacetic acid needling in the treatment of palmoplantar warts. Indian J Drugs Dermatol. 2020;6(1):13.
15. Attia A, Alawady AA, Abdo HM. Evaluation of topical 30% potassium hydroxide versus 30% trichloroacetic acid in the treatment of plane warts. Al-Azhar Med J. 2020;49(4):2053–64.
16. Al-Hamdi K. Evaluation of topical potassium hydroxide solution for treatment of plane warts. Indian J Dermatol. 2012;57(1):38-41.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}