


Cinthia Trisóglio1; Silvia Maria de Souza Quaggio2
Funding source: None.
Conflict of interest: None.
Submission date: 10/25/2024
Final decision: 01/30/2025
How to cite this article: Trisóglio C, Quaggio SMS. Secondary correction of prominent ears with closed otoplasty. Surg Cosmet Dermatol. 2025;17:e20250416.
Prominent ears are a common congenital deformity, affecting around 5% of the population, in addition to harming self-esteem and psychological well-being. To report a case of closed otoplasty in a 37-year-old patient who was dissatisfied with the results of an open otoplasty performed in childhood, with recurrence and erasure of the antihelix. The closed, incisionless technique was performed with local anesthesia and Mustardé percutaneous sutures, creating the antihelix with no need for incisions. The procedure was performed in an outpatient setting, with sutures buried under the skin and no apparent stitches, followed by the use of an immobilization bandage at night for 2 months. The surgery was completed in approximately 30 minutes per ear, with no complications. The patient reported mild to moderate pain in the first few days, which was relieved with analgesics. No complications, such as hematomas or keloids, were observed at the 2- and 24-month follow-up visits. The patient was highly satisfied with the aesthetic result and modeling of the antihelix. Closed otoplasty proved to be an effective and safe alternative for correcting prominent ears, with significant aesthetic and psychological benefits. It is suitable for cases of mild to moderate deformity.
Keywords: Surgery, Plastic; Anesthesia; Minor Surgical Procedures.
Prominent ears are the most common congenital deformity of the outer ear, affecting approximately 5% of the general population. A harmonious face goes far beyond skin care alone. Correcting prominent ears to their ideal anatomy makes all the difference in improving the appearance of the face, in addition to alleviating psychological issues, boosting self-esteem, and increasing self-confidence. Several authors have described techniques for treating prominent ears. Prominent ears are mainly caused by the absence of an antihelix and/or conchal hypertrophy and anterior rotation of the lobe. More than 200 techniques have been suggested to surgically correct prominent ears. The existence of so many approaches highlights that no single technique can correct all cases and that new techniques and modifications will continue to be developed. There are 3 main groups of surgical techniques used to correct prominent ears: cartilage-cutting techniques (CCT), cartilage-sparing techniques (CST), and incisionless or closed techniques. Mustardé1 and Furnas2 were pioneers in the use of concha-scapha and concha-mastoid sutures with little or no cartilage incision, forming the basis for incisionless otoplasty, which inspired Fritsch3 and Peled4 to describe the incisionless otoplasty technique, in which permanent sutures are used to recreate the antihelix, placed percutaneously and buried through the needle holes along the way, making surgical treatment more versatile, simpler, and safer. In recent years, there have been increasing requests for minimally invasive methods to perform otoplasty. The reasons behind this development are the search for methods to minimize invasive surgical techniques and, on the other hand, to reduce postoperative risks, including hematoma and increased scarring. Peled4 published the idea of knifeless otoplasty and Fritsch3 described incisionless otoplasty in 1995. Fritsch applied his technique to prominent ears, a suture-only technique, creating a new antihelix fold with horizontal mattress sutures placed percutaneously and subcutaneously. A modification of this technique is described by Peled as "incisionless otoplasty," combining a suture technique similar to Fritsch's with blind puncture of the anterior antihelix through a small skin incision in the anterior tail area of the antihelix. Serdev5 stated that "Serdev Suture® transcutaneous closed approach lifts encompass the main concept of suspension and/or suture repositioning." Nikolay uses a Deschamps aneurysm needle (30G), which is more traumatic than the custom curved syringe needle (28G) used in the reported technique. Both needles could be used to pass sutures and score the cartilage. Merck6 adopted Peled's method with modification of the guide wire, dorsal placement of the knots, and no cartilage processing, but this technique, 4 in 1 mattress suture to fold the poorly defined antihelix, did not correct other ear deformities such as conchal hypertrophy or concha-mastoid angle. The choice of surgical technique should be customized for each patient according to a meticulous preoperative evaluation. Therefore, we report the case of a 37-year-old female patient who had previously undergone open otoplasty at the age of 7. Even so, she was still dissatisfied, as the open surgery did not provide complete correction of the prominent ear. We opted for a secondary approach using the closed otoplasty technique to treat the antihelix.
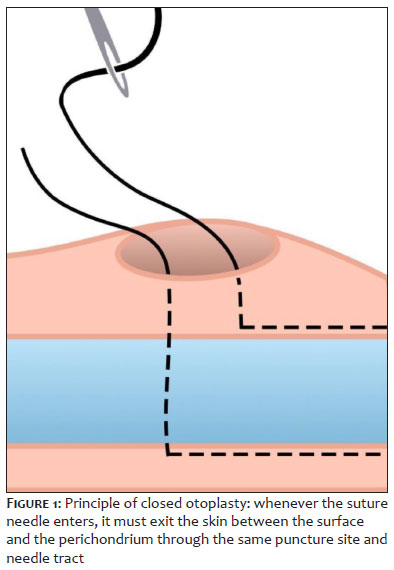
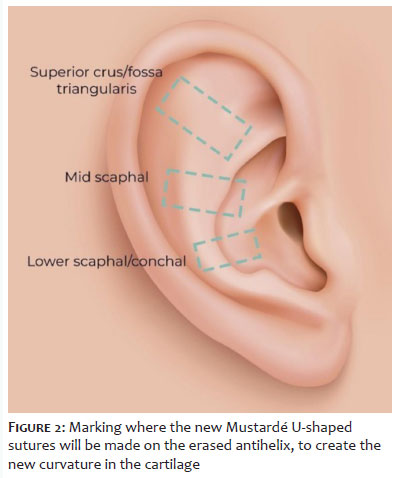
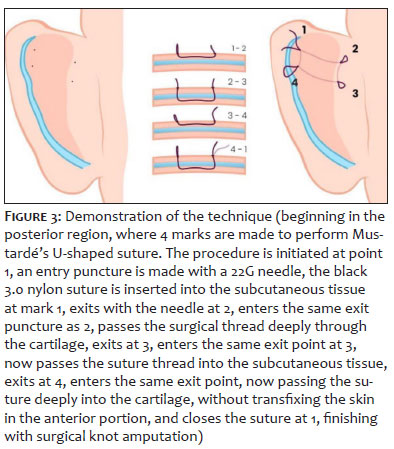
The closed otoplasty technique consists of a closed surgical approach to correct prominent ears. We perform tumescent anesthesia to promote anterior and posterior displacement of the cartilage, performing permanent percutaneous subcutaneous horizontal nonabsorbable sutures via the anterior approach and no incision. Percutaneous Mustardé mattress sutures are appropriately placed, forming the antihelix. To ensure that each suture is buried under the skin, the needle must re-enter the skin at the exact point where it exits. (Figure 1) The main indication is to correct the changes that caused the antihelix of the auricle to disappear without the need for incisions. After undergoing anamnesis, the selected patient, in an outpatient setting, with no need for sedation or general anesthesia, underwent rigorous antisepsis and placement of disposable sterile drapes. A surgical pen with a fine/thick double tip and methylene blue ink was used to mark the new antihelix, and 3 marks were made. The anesthesia injected into the antihelix was a 1% lidocaine solution with 1/200,000 adrenaline, achieving adequate blanching and distribution of the solution in the anterior and posterior aspects of the ear, with one of the objectives being the expansion and displacement of the skin from the cartilage. A 10-minute wait was observed between the application of the anesthetic in order to increase the efficiency of the vasoconstrictive action. A 22G hypodermic needle is then used on the previous markings to percutaneously mark the cartilage at the level where the antihelix fold is to be created, being placed percutaneously following a type of horizontal Mustardé mattress suture, which we numbered points 1-2-3-4, to recreate the antihelix fold and reduce the prominence of the concha. The first point was transfixed into the skin of the posterior surface of the auricle at point 1 and passed through the subcutaneous tissue, emerging in the skin at mark 2. It then re-entered the same puncture site, now transfixing the cartilage deeply, going to point 3, emerging at 3, re-entering the same puncture site, and going to point 4 in the subcutaneous tissue. It exits at point 4, passes the suture deeply through the cartilage, without exiting the skin anteriorly, continuing to point 1, closing the suture, and ending by cutting the knot. Transfixing only the skin, it returns to the initial region, forming a "rectangular design," Mustardé U-shaped sutures (Figure 2) and (Figure 3). It is important to note that the suture needle always enters and exits the skin between the surface and the perichondrium through the same puncture site and needle tract (Figure 1). Transfixation of the subdermal needle to hide the stitch and cut close to the skin. Note the positioning and posterior displacement of the auricle and formation of the new antihelix. We performed 2-3 sutures in the posterior region and in the anterior region along the erased antihelix. Compressive gauze and sterile micropore tape were inserted into the dressing. This technique does not involve skin resection, scraping, or incisions in the cartilage, nor does it leave visible stitches or require stitch removal. Postoperatively, the use of bandage is recommended to immobilize the ear against the head to prevent accidental folds, only at night for 2 months. Follow-up was performed through photos and patient visits to assess changes and complications, such as recurrence and infections, at 15 days, 2 months, and 24 months. The entire procedure is performed with a minimally invasive needle. For this reason, complications are minimized, as no dissection planes or skin flaps are created, nor is there any skin resection, scraping, or incisions in the cartilage, nor are there any visible stitches, and no need for stitch removal. Postoperatively, the use of bandage is recommended to immobilize the ear against the head to prevent accidental folds, only at night for 2 months. For this reason, postoperative care is minimal.
The otoplasty was performed with no incisions and, therefore, no scars, with a mean operative time of 30 minutes per ear. The entire procedure was performed with local anesthesia and no sedation. The patient reported mild to moderate pain in the first 3 days postoperatively, which was alleviated with analgesics. Healing ointment was applied to the wire entry sites for 15 days, and oral antibiotics were prescribed for 7 days. At the 2-month follow-up, no complications or adverse events such as ecchymosis, edema, necrosis, hyperesthesia, keloid, recurrence, exposure of stitches, or asymmetry were observed. Good modeling of the antihelix was observed even after 24 months, and the patient was very satisfied.
There are more than 200 techniques for correcting prominent ears. The main treatment is to correct the hypertrophic concha and shape the antihelix. In 1992, Fritsch modified the techniques from open to closed otoplasty. This surgical treatment provides many advantages for patients and surgeons due to its lower risk of complications and minimally invasive approach to correcting the ears. This new surgical approach has simplified otoplasty and made it more versatile in treating a wide range of ear deformities, especially those requiring antihelix correction. This study reports a secondary surgical case using the closed otoplasty technique in a 37-year-old female patient who had previously undergone unsuccessful open otoplasty surgery. At the time, the patient did not seek repair of the open otoplasty surgery because she had experienced trauma from the surgery in childhood, had experienced severe pain for 3 months, and had edema in her ear. She learned about this new approach and sought clarification. During the consultation, the patient was wary of the new surgical approach, but as her prominent ears still bothered her, it was explained to her that it would be a different technique, which reassured her, making her feel safe and satisfied. A new surgery was scheduled, now secondary with a closed approach. No complications occurred during the surgical procedure, and postoperatively, the patient only experienced pain within 24 hours of the procedure, which was resolved with analgesics. The results were evaluated subjectively after 15 days, 2 months, and 24 months, using preoperative and postoperative photos (Figures 4, 5, and 6), and the patient was very satisfied. (Figure 7)
We believe that different ear deformities should be corrected by different techniques, thus providing greater naturalness and harmony to overall appearance. The closed otoplasty technique is not a solution for all types of prominent ears, but rather for the correction of antihelix erasure, mainly in malleable cartilage with no conchal hypertrophy. This is a conservative procedure, easy to perform, easily reproducible, with low patient discomfort, and relatively no major complications. It has excellent applicability in all age groups. Otoplasty goes beyond facial aesthetics. It is a procedure that promotes the patient's well-being, restoring their self-esteem, self-confidence, and quality of life. Considering the benefits of a rapid and painless postoperative period, incisionless otoplasty clearly represents a valuable tool for promoting the individual's overall health. This technique is intended to be another asset in the arsenal of dermatological surgery.
Cinthia Trisóglio
ORCID: 0000-0001-8288-2518
Approval of the final version of the manuscript, conception and design of the study, preparation and writing of the manuscript, acquisition, analysis and interpretation of data, effective participation in the conduct of the study, intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, critical review of the literature, critical revision of the manuscript.
Silvia Maria de Souza Quaggio
ORCID: 0000-0001-8199-3961
Approval of the final version of the manuscript, conception and design of the study, preparation and writing of the manuscript, acquisition, analysis and interpretation of data, effective participation in the conduct of the study, intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, critical review of the literature, critical revision of the manuscript.
1. Mustardé JC. The correction of prominent ears using simple mattress sutures. Br J Plast Surg 1963;16:170-8.
2. Furnas DW. Correction of prominent ears by concha-mastoid sutures. Plast Reconstr Surg. 1968;42(3):189–93.
3. Fritsch MH. Incisionless Otoplasty. Otolaryngol Clin N Am. 2009; 42(6):1199-208.
4. Peled IJ. Knifeless otoplasty: how simple can it be? Aesth Plast Surg. 1995;19(3):253-5.
5. Serdev NP. Scarless serdev suture method in prominent ears. Int J Cosmet Surg. 2006;6(2):184–90.
6. Merck W. Ohrmuschelkorrektur ohne hautschnitt – die Fadenmethode von Merck. Korrektur und Rekonstruktion der Ohrmuschel. Berlim: Springer; 2017. p.153–69.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}