


Emerson Henrique Padoveze1,2; Suelen Montagner3; Thamires Prado Dantas2; Nilton Gioia Di Chiacchio4,5; Nilton Di Chiacchio4
Funding source: None.
Conflict of interest: None.
Submission date: 09/04/2024
Final decision: 10/03/2024
How to cite this article: Padoveze EH, Montagner S, Dantas TP, Di Chiacchio NG, Di Chiacchio N. Treatment of periungual warts: a literature review. Surg Cosmet Dermatol. 2025;17:e20250402.
Periungual warts are the most common tumors of the periungual region, primarily affecting children and adolescents. Caused by human papillomavirus (HPV), they can lead to cosmetic disfigurement in patients. There are several therapeutic options for the treatment of this condition, and the choice of treatment depends on the number of warts, patient age, immune status, and skill of the dermatologist. Given the high recurrence rate and numerous therapeutic possibilities, this review article provides a comprehensive summary of the condition, with a particular focus on treatment modalities.
Keywords: Warts; Nail Diseases; Papillomavirus Infections.
Periungual warts are the most common tumors of the periungual region, primarily affecting children and adolescents. Caused by human papillomavirus (HPV), they can lead to cosmetic disfigurement in patients. There are several therapeutic options for the treatment of this condition, and the choice of treatment depends on the number of warts, patient age, immune status, and skill of the dermatologist. Given the high recurrence rate and numerous therapeutic possibilities, this review article provides a comprehensive summary of the condition, with a particular focus on the available treatment modalities.
Warts caused by HPV can appear anywhere on the body.1 Those located around the nail are known as periungual warts, while those found under the nail are called subungual warts. There are approximately 218 types of HPV, and genotypes 1, 2, 4, 27, and 57 are most commonly associated with periungual warts.2,3 They most frequently affect children and adolescents (peak between 12 and 16 years of age),4 reaching an estimated prevalence of 33% in this age group and 22% in the general population.5,6 HPV enters the skin through abrasions or maceration,4,7 which expose the keratinocytes of the basal layer, facilitating virus penetration.8,9 This explains the higher prevalence of periungual warts in individuals who bite their nails, suck their fingers, or work in humid environments. Warts are acquired through direct or indirect contact with HPV, and the development of infection depends on local and systemic factors, including host predisposition and immunity. Patients with HIV, hematologic malignancies, and transplant recipients tend to have larger and multiple lesions.10 In general, warts are not highly contagious,11 and clinical lesions can appear from a few weeks to 1 year after infection.4 The presence of viral DNA in apparently normal skin indicates the existence of subclinical viral infections.12 Most patients with periungual warts require treatment due to cosmetic disfigurement, as well as functional and social concerns. There are various treatment approaches for this condition, including the use of cytotoxic agents, cryotherapy, electrosurgery, immunotherapy, and laser. However, despite these treatment options, many lesions are resistant and recalcitrant, making their cure a challenge. Among all viral warts, those located in the periungual and plantar regions have the highest recurrence rates.13,14 In response to this challenge, this review article provides a comprehensive summary of the condition, with a particular focus on treatment modalities. We have categorized treatment modalities into 3 groups based on their mechanisms of action: destructive treatments, characterized by epidermal destruction or keratolysis; immunotherapy, focused on the production of antiviral cytokines and stimulation of cell-mediated immune responses; and cytotoxic agents, designed to interfere with viral replication. Doses, drug administration intervals, and potential adverse events will be discussed for each modality.
Periungual warts may originate from the proximal nail and lateral folds or hyponychium. They initially appear as 1-mm hyperkeratotic normochromic papules, which can later grow up to 1 cm in diameter or coalesce into plaques. When the proximal nail fold is affected, it may simulate a hyperkeratotic cuticle. Changes to the nail plate are uncommon, as HPV does not usually affect the nail matrix. However, external compression can lead to grooves and ridges. When the nail bed is affected, onycholysis and splinter hemorrhages may occur. In rare cases, hypercurvature of the nail plate may be observed4 (Figure 1). Dermoscopy is a useful diagnostic tool, revealing the typical punctate rough surface and dilated capillaries15 (Figure 2).
Pathology reveals epithelial hyperplasia with acanthosis, papillomatosis, and hyperkeratosis with parakeratotic stratum corneum. Thrombi within dilated capillaries and mononuclear cells may be present in the dermis.8
The diagnosis of periungual warts is usually clinical. The classic clinical sign of warts is the pinpoint bleeding resulting from trauma to the capillaries.4 In doubtful cases, dermoscopy and biopsy can assist in diagnosis. In situ hybridization and polymerase chain reaction (PCR) allow viral identification.16,17 In older patients with long-standing single lesions or in cases refractory to conventional treatment, the diagnosis of squamous cell carcinoma should be ruled out with biopsy. HPV 16 is the most common subtype in malignant cases.
Treatment of periungual warts is challenging compared to other types of viral warts due to high recurrence and treatment-related pain. While it was believed that 65% of warts could disappear spontaneously,18 spontaneous resolution is more common in children. In adults and adolescents, these lesions are less likely to disappear spontaneously. Furthermore, untreated lesions can spread to other sites, increase in size, and even become a source of infection to other individuals. Several treatment modalities are available, which can be divided into destructive, immunotherapeutic, and cytotoxic. The choice of treatment depends on the number, location (periungual or subungual), and duration of the warts, age and immune status of the patient, and skill of the dermatologist.4 Below, we will address the specific characteristics of each treatment modality.
These are considered a good conservative treatment option, especially for children, as some lesions may regress spontaneously in this age group.18 This category includes keratolytic agents and caustics such as cantharidin, trichloroacetic acid, and fuming nitric acid.
These are the most popular treatment for periungual warts and are particularly suitable for children due to their safety profile, reduced pain, and topical application as creams, ointments, or quick-drying acrylate lacquers.4 They act by destroying and irritating virus-infected keratinocytes in the epidermis.19 Salicylic acid, at concentrations of 16% to 50%, is the most commonly used agent. It should be applied 5-7 times per week for 12 weeks to provide a clearance better than placebo (15% and 8%, respectively).8
Cantharidin is a vesicant that causes acantholysis and blistering within the epidermis. It is isolated from the insect Cantharis vesicatoria. At a concentration of 0.7%, it is applied to the wart using a cotton swab, while protecting the surrounding healthy skin. Patients should cover the treated area for 4 to 8 hours before washing it with soap and water. Blister formation at the application site is common and usually resolves within 1 to 2 weeks. The reported efficacy in the literature is approximately 80%.20 Pain and a burning sensation may occur as adverse events. This medicine is not available in Brazil.
The treatment involves applying liquid nitrogen at -196 ºC to lesions for approximately 10 to 15 seconds. This process induces irreversible damage to keratinocyte cell membranes through freezing and stimulates cellular immune response. For hyperkeratotic lesions, prior curettage can be performed to enhance the penetration of liquid nitrogen.4 Cryotherapy has an efficacy rate of approximately 70% and is generally well tolerated.21 Adverse events include pain at the application site, which may persist for up to 72 hours, hypochromia or hyperchromia, and scarring. Warts located in the proximal nail fold treated with cryotherapy may develop leukonychia, Beau's lines, and onychomadesis. Severe matrix damage may lead to irreversible nail atrophy.8
The 585 nm pulsed dye laser targets hemoglobin. The mechanism of action is attributed to thermal injury to HPV and the destruction of blood vessels supplying the warts.22 Studies generally indicate clearance rates comparable to those of conventional methods, and this treatment is considered safe for both adults and children.22 Potential adverse events include hypopigmentation, scarring, purpura, pain, and burning sensation at the application site.23,24 The CO2 laser emits at 10,600 nm, a wavelength absorbed by water, which causes thermal injury and vaporization of HPV-infected epidermal cells. For subungual lesions, removal of the nail plate is required before laser application.4 Lim & Goh25 reported a 57.4% clearance rate using power settings from 3 to 15 W and a spot size of 2 mm. Pain is the most common adverse event, but nail changes such as onycholysis, thinning of the nail plate, and transient changes in sensitivity may also occur.26 The Er:YAG laser emits at 2,940 nm, a wavelength also absorbed by water, and acts similarly to the CO2 laser. However, it is more selective, resulting in less tissue damage and, consequently, fewer adverse events. While there are reports of the use of the Er:YAG laser for facial flat warts with a 62.5% clearance rate,27 no published studies exist on its use for periungual warts.
Electrosurgery should be avoided for tissue destruction in wart-affected areas due to the risk of scarring and permanent nail matrix damage.8 In addition, it is associated with prolonged healing times and postoperative pain. In general, regardless of the selected method, the aggressiveness of the technique is not related to the clearance rate.
It acts as an immunomodulator due to its ability to stimulate the production of cytokines (especially interferon) and the migration of Langerhans cells.28,29 The literature shows varying dosing regimens, typically ranging from 3 to 5 times per week. Some authors use imiquimod under occlusive dressing or in combination with keratolytics,30 because, when used alone, its efficacy is reduced due to the difficulty of penetration of the medication into the keratotic surface of warts.31 Micali et al.32 reported an 80% clearance rate for periungual and subungual warts applying 5% imiquimod for 5 consecutive days per week over 6 weeks, combined with 50% salicylic acid in white petrolatum (Figure 3). Furthermore, the literature also indicates that the combined use of imiquimod and ablative lasers for recalcitrant warts yields superior results compared with the use of imiquimod alone.10
Diphencyprone is a sensitizer used in weekly applications, with dilutions ranging from 0.001% to 3% according to the patient's response. The goal of treatment is to induce mild contact dermatitis.33 Rampen et al.,34 in a study of periungual and palmoplantar warts, applied a diphencyprone solution of 0.1%-3% to the warts once a week for 8 weeks, in 154 patients. The results showed a clearance rate of 8% after 2 months and 44% after a 4-month follow-up. Adverse events were considered mild.
Another immunotherapy option is the application of vitamin D3 (calcipotriol), topically or by injection. Vitamin D is believed to regulate the proliferation and differentiation of epidermal cells and to modulate cytokine production.35 Topical calcipotriol can be applied 1 to 3 times a day, with a treatment duration of 3 to 18 months, as reported in the literature.36-38 For injectable vitamin D, the described dose is 0.2 mL of vitamin D at a concentration of 15 mg/mL, administered at the base of the periungual wart after injecting local anesthetic.10,39 Adverse events such as mild pain, edema, and erythema may occur at the application site.40 A recent study comparing intralesional vitamin D and purified protein derivative (PPD) for the treatment of extragenital warts showed slightly lower efficacy in the vitamin D group (21.7% vs. 59%).10 The application of PPD antigen provides an increase in interleukin (IL)-12 and IL-14 levels, contributing to a cell-mediated reaction. Cure rates with this treatment modality range from 23% to 77%. Clearance rates with this treatment modality range from 23% to 77%.40-42 Adverse events include pain, blistering, and erythema.
Cimetidine, a histamine H2 receptor antagonist, has demonstrated variable efficacy in the treatment of warts. Its action is attributed to an increase in T cells, leading to cellular immune response. The reported dosage in the literature is 25-40 mg/kg/day, divided into 3 daily doses.8 This medication is generally well tolerated, and the most frequently reported adverse events are gastrointestinal disturbances, dizziness, and drowsiness.43 A major drawback of cimetidine treatment is the need for multiple daily administrations over months, which may impact treatment adherence.44 For children with multiple, extensive, or recalcitrant warts, treatment with cimetidine has reported cure rates ranging from 56% to 82%.29,45
HPV vaccines, which contain noninfectious virus-like particles of the L1 capsid protein, have shown well-established efficacy in the prevention of HPV-related diseases, such as anogenital warts and cervical, vulvar, vaginal, and anal cancers. Currently, 3 types of HPV vaccines are available: bivalent – against HPV 16 and 18; quadrivalent – against HPV 6, 11, 16 and 18; and nonavalent – against HPV 6, 11, 16, 18, 31, 33, 45, 52 and 58. These vaccines are associated with strong cellular immune responses and the production of HPV type-specific neutralizing antibodies.46 In the treatment of warts caused by HPV strains other than those contained in the vaccines, it is believed that a cross-immune response occurs, leading to the resolution of non-genital lesions.47,48 Studies have explored the use of bivalent,47 quadrivalent,49,50 and nonavalent51 HPV vaccines (administered at 0, 2, and 6 months) for the treatment of periungual warts. In the treatment of common warts, a comparative study of intralesional versus intramuscular bivalent HPV vaccine showed a clearance rate of 81.8% in the intralesional group and 63.3% in the intramuscular group, with no significant difference between the groups.47 Shin et al.51 treated 45 patients with recalcitrant extragenital warts, primarily plantar and periungual, using the nonavalent HPV vaccine. A dose of 0.5 mL was injected intramuscularly at 0, 2, and 6 months, resulting in a 62.2% clearance rate. Potential adverse events included pain at the application site, pruritus, and fatigue.
It has been a safe and effective antimitotic agent in the treatment of periungual warts for over 5 decades.52 It acts primarily on DNA cleavage53 and promotes endothelial damage,54 resulting in high clearance rates of 92% to 96%. Most studies suggest an optimal dose between 0.1 and 0.3 U/lesion, with a maximum recommended dose of 3 U per session. The medication can be administered by needle injection at the base of the lesion or by applying a drop of bleomycin solution to the surface of the lesion, followed by multiple punctures. Typically, 2 to 3 sessions are required, with intervals of 3 to 4 weeks between them55 (Figure 4).
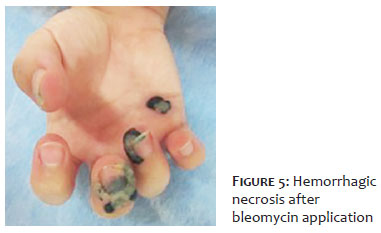
The main limiting factor of this treatment is pain, which can range from moderate to severe during application.11 However, pain can be alleviated by adding an anesthetic during medication dilution or by performing a digital nerve block before infiltration. Other side effects include erythema, edema, ulceration, hemorrhagic crusting, transient hypopigmentation or hyperpigmentation, atrophic or hypertrophic scars, and hematoma. Less common adverse events include Raynaud's phenomenon, tissue necrosis, nail dystrophy, and nail loss (Figure 5).
Cidofovir is a nucleoside analog antiviral agent that resembles cytosine. After intracellular phosphorylation, the active metabolite cidofovir diphosphate serves as a substrate for viral DNA polymerase, being incorporated into viral DNA and terminating its replication. It has a 25- to 50-fold higher affinity for viral over cellular DNA polymerase and, unlike other nucleoside analogs (acyclovir and ganciclovir), it does not require viral enzymes for molecular activation, making it effective against viral strains resistant to tyrosine kinase.56,57 Due to poor oral bioavailability, cidofovir is often administered intravenously, topically, and intralesionally. The intralesional route provides the highest clearance rates for the treatment of viral warts (75.9%-100%), with a recommended dose of 15 mg/mL every 15-30 days, which may be preceded by local anesthesia with lidocaine. Potential adverse events include erythema, pruritus, and blistering at the application site.58 Cidofovir cream (1%-3%), applied twice daily with or without occlusive dressing, can achieve a 55.2% clearance rate. It is suitable for both adults and children, whether immunocompromised or not.59,60 Due to a possible delayed response, treatment may be prolonged for at least 10-12 weeks.61 Adverse events include erythema, pruritus, and burning sensation. Injectable cidofovir, administered at a dose of 3.5-5 mg/kg for 2 weeks to 4 months, can achieve a 75% clearance rate. However, caution is advised due to potential nephrotoxicity and immunosuppression.10 Overall, despite the promising results, the use of cidofovir is limited by its high cost.
The treatment of periungual warts poses a challenge in dermatological practice, primarily due to the risk of scarring and pain associated with the procedures. While several treatment modalities are currently available, selecting the most suitable method requires careful consideration of factors such as the number of lesions, patient age, degree of immunosuppression, and the availability and cost of treatment. Among the existing options, bleomycin has been our treatment of choice due to its high clearance rates and good tolerability. Immunotherapies have emerged as a promising, safe, and less invasive alternative. However, further studies are needed to fully demonstrate the efficacy of these new treatment options.
Emerson Henrique Padoveze
ORCID: 0009-0001-3025-0372
Approval of the final version of the manuscript, conception and design of the study, preparation and writing of the manuscript, acquisition, analysis and interpretation of data, effective participation in the conduct of the study, intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, critical review of the literature, critical revision of the manuscript.
Suelen Montagner
ORCID: 0000-0002-6597-2981
Approval of the final version of the manuscript, conception and design of the study, preparation and writing of the manuscript, acquisition, analysis and interpretation of data, effective participation in the conduct of the study, intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, critical review of the literature, critical revision of the manuscript.
Thamires Prado Dantas
ORCID: 0009-0002-8379-1401
Approval of the final version of the manuscript, conception and design of the study, preparation and writing of the manuscript, acquisition, analysis and interpretation of data, effective participation in the conduct of the study, intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, critical review of the literature, critical revision of the manuscript
Nilton Gioia Di Chiacchio
ORCID: 0000-0001-5944-7737
Approval of the final version of the manuscript, conception and design of the study, preparation and writing of the manuscript, acquisition, analysis and interpretation of data, effective participation in the conduct of the study, intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, critical review of the literature, critical revision of the manuscript.
Nilton Di Chiacchio
ORCID: 0000-0001-9536-2263
Approval of the final version of the manuscript, conception and design of the study, preparation and writing of the manuscript, acquisition, analysis and interpretation of data, effective participation in the conduct of the study, intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, critical review of the literature, critical revision of the manuscript.
1. Xu J, Zhang D, Feng L, Liu Y, Diao Q. The efficacy and safety of topical Tretinoin combined with superficial X-ray therapy (SXRT) in treating periungual warts. Dermatol Therap. 2022;35(3):e15295.
2. Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, Fitzpatrick TB. Fitzpatrick's dermatology in general medicine. 5th ed. Nova York: McGraw- Hill (US); 1999.2484p.
3. Herschthal J, McLeod MP, Zaiac M. Management of ungual warts. Dermatol Therap. 2012;25(6):545-50.
4. Tosti A, Piraccini BM. Warts of the nail unit: surgical and nonsurgical approaches. Dermatol Surg. 2001;27(3):235–9.
5. Bruggink SC, Koning MNC, Gussekloo J, Egberts PF, Schegget JT, Feltkamp MCW, et al. Cutaneous wart-associated HPV types: prevalence and relation with patient characteristics. J Clin Virol. 2012;55(3):250-5.
6. Kilkenny M, Merlin K, Young R, Marks R. The prevalence of common skin conditions in Australian school students: 1. Common, plane and plantar viral warts. Br J Dermatol. 1998;138(5):840-5.
7. Jablonska S, Obalek S, Golebiowska A, Favre M, Orth G. Epidemiology of butchers' warts. Arch Dermatol Res.1988;280:S24–8.
8. Sonali Nanda, Rachel Fayne, Martin N. Zaiac. Warts. In: Nilton di Chiacchio, Antonella Tosti, editors. Therapies for Nail Disorders. Boca Raton. 2020, p. 156- 67.
9. Egawa N, Egawa K, Griffin H, Doorbar J. Human Papillomaviruses; Epithelial Tropisms, and the development of neoplasia. Viruses. 2015;7(7):3863-90.
10. Kanchana L, Sasima T, Poonkiat S, Suthinee R. A comprehensive review of treatment options for recalcitrant nongenital cutaneous warts. J Dermatolog Treat. 2022;33(1):23-40.
11. Silgal A, Grover C. Efficacy and safety of intralesional bleomycin in the management of ungual warts. Skin Appendage Disord. 2020;6(6):346–50.
12. Boxman IL, Berkhout RJ, Mulder LH, Wolkers MC, Bavinck JNB, Vermeer BJ, et al. Detection of human papillomavirus DNA in plucked hairs from renal transplant recipients and healthy volunteers. J Invest Dermatol 1997;108(5):712–5.
13. Leung L. Treating common warts - options and evidence. Aust Fam Physician. 2010;39(12):933-7.
14. Choi Y, Kim DH, Jin SY, Lee Ai-Young, Lee SH. Topical immunotherapy with diphenylcyclopropenone is effective and preferred in the treatment of periungual warts. Ann Dermatol. 2013;25(4):434-9.
15. Piraccini BM, Bruni F, Starace M. Dermoscopy of non-skin cancer nail disorders. Dermatol Ther. 2012;25(6):594-602.
16. Callen JP, Jorizzo JL, Bolognia JL, Zone JJ, Piete WW. Dermatological signs of internal diseases. 4th ed. New York: Sounders Elsevier; 2009. p.311-24.
17. Sterlin JC, Tyring SK. Human papillomaviruses: clinical and scientific advances. New York: Oxford University Press; 2001.p.10-23.
18. Laurent R, Kienzler JL. Epidemiology of HPV infections. Clin Dermatol. 1985;3(4):64-70.
19. Sterling J. Treatment of warts and molluscum: what does the evidence show? Curr Opin Pediatr. 2016;28(4):490-9.
20. Wolverton SE, Comprehensive dermatologic drug therapy. Philadelphia: W.B Saunders Company; 2001. p.524-36.
21. Walkzuk I, Eertmans F, Rossel B, Cegielska A, Stockfleth E, Antunes A, et al. Efficacy and safety of three cryotherapy devices for wart treatment: a randomized, controlled, investigator- blinded, comparative study. Dermatol Ther (Heidelb). 2018;8(2):203-16.
22. Jacobsen E, McGraw R, McCagh S. Pulsed dye laser efficacy as initial therapy for warts and against recalcitrant verrucae. Cutis. 1997;59(4):206-8.
23. Nguyen J, Korta DZ, Chapman LW, Kelly KM. Laser treatment of nongenital verrucae: a systematic review. JAMA Dermatol. 2016;152(9):1025-34.
24. Park HS, Choi WS. Pulsed dye laser treatment for viral warts: a study of 120 patients. J Dermatol. 2008;35(8):491-8.
25. Lim JT, Goh CL. Carbon dioxide laser treatment of periungual and subungual viral warts. Australas J Dermatol. 1992;33(2):87-91.
26. Street ML, Roenigk RK. Recalcitrant periungual verrucae: the role of carbon dioxide laser vaporization. J Am Acad Dermatol. 1990;23(1): 115-20.
27. Balevi A, Ustuner P, Ozdemir M. Use of Er:YAG for the treatment of recalcitrant facial verruca plana. J Dermatolog Treat. 2017;28(4):368-71.
28. Suzuki H, Wang B, Shivji GM, Toto P, Amerio P, Tomai MA, et al. Imiquimod, a topical immune response modifier, induces migration of Langerhans cells. J Invest Dermatol. 2000;114(1):135-41.
29. Veasey JV, Miguel BAF, Campaner AB, Manzione TS. Imiquimod use for the treatment of extramammary Paget disease: series of four cases. Surg Cosmet Dermatol. 2018;10(4):309-13.
30. Ahn CS, Huang WW. Imiquimod in the treatment of cutaneous warts: an evidence-based review. Am J Clin Dermatol. 2014;15(5):387-99.
31. Edwards L. Imiquimod in clinical practice. J Am Acad Dermatol. 2000;43:S12-7.
32. Micali G, Dall'Oglio F, Nasca MR. An open label evaluation of the efficacy of imiquimod 5% cream in the treatment of recalcitrant subungual and periungual cutaneous warts. J Dermatolog Treat. 2003;14(4):233-6.
33. Silverberg NB, Lim JK, Paller AS, Mancini AJ. Squaric acid immunotherapy for warts in children. J Am Acad Dermatol. 2000;42(5 Pt 1):803–8.
34. Rampen FH, Steijlen PM. Diphencyprone in the management of refractory palmoplantar and periungual warts: an open study. Dermatology. 1996;193(3):236-8.
35. Osborne JE, Hutchinson PE. Vitamin D and systemic cancer: is this relevant to malignant melanoma? Br J Dermatol. 2002;147(2):197-213.
36. Egawa K, Ono T. Topical vitamin D3 derivatives for recalcitrant warts in three immunocompromised patients. Br J Dermatol. 2004;150(2):374-6.
37. Moscarelli L, Annunziata F, Mjeshtri A, Paudice N, Tsalouchos A, Zanazzi M, et al. Successful treatment of refractory wart with a topical activated vitamin d in a renal transplant recipient. Case Rep Transplant. 2011:2011:368623.
38. Imagawa I, Suzuki H. Successful treatment of refractory warts with topical vitamin D3 derivative (maxacalcitol, 1alpha, 25-dihydroxy-22-oxacalcitriol) in 17 patients. J Dermatol. 2007;34(4):264-6.
39. Jain Sk, Mohta A. Recalcitrant periungual warts in a paediatric patient treated with intralesional vitamin D3. Indian J Med Res. 2020;152 (Suppl 1):S44.
40. Abd-Elazeim FM, Mohammed GF, Fathy A, Mohamed RW. Evaluation of IL-12 serum level in patients with recalcitrant multiple common warts, treated by intralesional tuberculin antigen. J Dermatolog Treat. 2014;25(3):264-7.
41. Amirnia M, Khodaeiani E, Fouladi DF, Masoudnia S. Intralesional immunotherapy with tuberculin purified protein derivative (PPD) in recalcitrant wart: a randomized, placebo- controlled, double-blind clinical trial including an extra group of candidates for cryotherapy. J Dermatolog Treat. 2016;27(2):173-8.
42. Kus S, Ergun T, Gun D, Akin O. Intralesional tuberculin for treatment of refractory warts. J Eur Acad Dermatol Venereol. 2005;19(4):515-6.
43. Jafarzadeh A, Nemati M, Khorramdelazad H, Hassan ZM. Immunomodulatory properties of cimetidine: its therapeutic potentials for treatment of immune-related diseases. Int Imunopharmacol. 2019;70:156-66.
44. Arancibia NR, Varas C, Munoz ER. Severe and recalcitrant periungual warts in a child successfully treated with cimetidine. Dermatol Therap. 2021;34(6):151-4.
45. Chern E, Cheng YW. Treatment of recalcitrant periungual warts with cimetidine in pediatrics. J Dermatolog Treat. 2010;21:314-6.
46. Ahn J, Best SRA & Tunkel DE. Advances in Vaccine Technology. In: Campisi P. editor. Recurrent Respiratory Papillomatosis. Springer: Cham. 2018; p.45-58.
47. Nofal A, Marei A, Ibrahim Al-Shimaa M, Nofal E, Nabil M. Intralesional versus intramuscular bivalent human papillomavirus vaccine in the treatment of recalcitrant common warts. J Am Acad Dermatol. 2020;82:94-100.
48. Lowe J, Panda D, Rose S, Jensen T, Hughes WA, Tso FY, et al. Evolutionary and structural analyses of alpha-papillomavirus capsid proteins yields novel insights into L2 structure and interaction with L1. Virol J. 2008;5(1):150.
49. Waldman A, Whiting D, Rani M, Alam M. HPV vaccine for treatment of recalcitrant cutaneous warts in adults: a retrospective cohort study. Dermatol Surg. 2019;45(12):1739-41.
50. Yang MY, Son JH, Kim GW, Kim HS, Ko HC, Kim MB, et al. Quadrivalent human papilloma virus vaccine for the treatment of multiple warts: a retrospective analysis of 30 patients. J Dermatolog Treat. 2019;30(4):405-9.
51. Shin JO, Son JH, Lee J, Kim HS, Ko HC, Kim BS, et al. Nonavalent human papilloma virus vaccine for the treatment of multiple recalcitrant warts: an open-label study. J Am Acad Dermatol; 86(4):940-1.
52. Umenzawa H, Maeda K, Takeuchi T. New antibiotics, bleomycin A and B. J Antibiot. 1966;19:200–9.
53. Saitta P, Krishnamurthy K, Brown LH. Bleomycin in dermatology: a review of intralesional applications. Dermatol Surg. 2008;34(10):1299-313.
54. Lee JH, Burm JS, Yang WY, Kang SY, Byun SW. Treatment of verruca vulgaris in both external auditory canals using bleomycin injections. Clin Exp Otorhinolaryngol. 2015;8(3):295-7.
55. Noriegal LF, Valandro LS, Di Chiacchio NG, Vieiral ML, Di Chiacchio N. Treatment of viral warts with intralesional bleomycin. Surg Cosmet Dermatol. 2018;10(1):16-20.
56. Zabawski J, Cockerell CJ. Topical and intralesional cidofovir: a review of pharmacology and therapeutic effects. J Am Acad Dermatol 1998;39(5 Pt 1):741-5.
57. Gnann JW, Salvaggio MR. Drugs for herpesvirus infections. Infect Dis. 2010;2:1454-63.
58. Cook Mk, Hagen EM, Feldman SR. Cidofovir in the management of non-genital warts: a review. J Drugs Dermatol. 2023;22(10):1009-16.
59. Cha S, Johnston L, Natkunam Y, Brown J. Treatment of verruca vulgaris with topical cidofovir in an immuno- compromised patient: a case report and review of the literature. Transpl Infect Dis.2005;7(3-):158–61.
60. Gupta M, Bayliss SJ, Berk DR. Topical cidofovir for refractory verrucae in children. Pediatr Dermatol. 2013;30(1):131–4.
61. Spaña LP, Boz J, Morano TF, Villafranca JA, Troya M. Successful treatment of periungual warts with topical cidofovir. Dermatol Therap. 2014;27(6):337-42.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}