


Inês Stafin1; Flávia Vieira Brandão2; Ana Maria Costa Pinheiro1
Funding: None.
Conflict of interest: None.
Submitted on: 08/08/2024
Final decision: 12/09/2024
How to cite this article: Stafin I, Brandão FV, Pinheiro AMC. Target nevus: dermoscopy and reflectance confocal microscopy. Surg Cosmet Dermatol. 2025;17:e20250395.
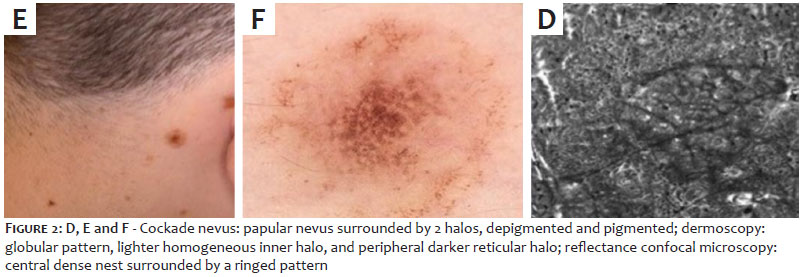
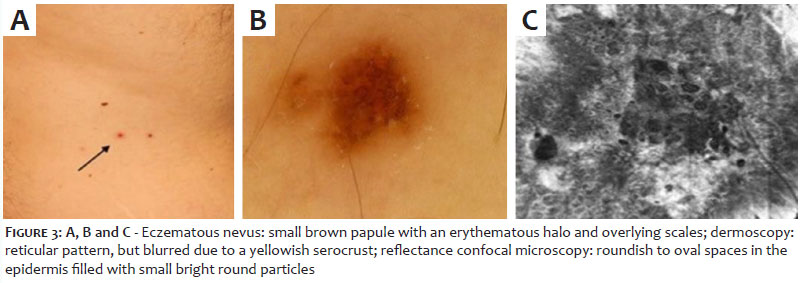
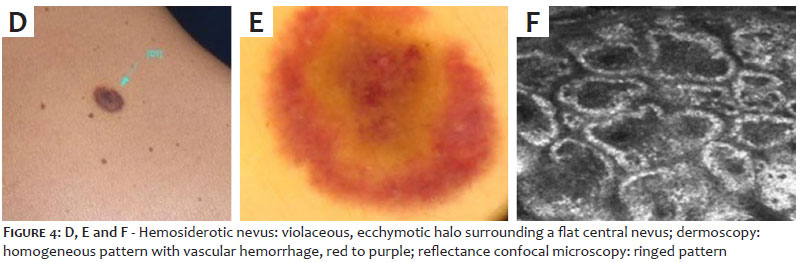
Halo, cockade, eczematous, and targetoid hemosiderotic nevi are known as target nevi, classified as melanocytic nevi with special features and often mimic melanoma. This communication aims to demonstrate clinical manifestations, dermoscopic patterns, and reflectance confocal microscopy findings in 4 patients with different types of target nevi.
Keywords: Dermoscopy; Microscopy, Confocal; Melanoma; Nevus, Halo.
Some melanocytic nevi are classified dermoscopically as special nevi, exhibiting distinct clinical and histopathologic features. They are considered "melanoma mimics" and include target nevi, such as halo, cockade, eczematous, and targetoid hemosiderotic nevi.1 While the dermoscopy and reflectance confocal microscopy (RCM) patterns of typical nevi are well-documented, there are limited data on this specific category of nevi.2 This communication aims to demonstrate clinical manifestations, dermoscopic patterns, and RCM findings in different cases of target nevi. We present 4 patients (2 men and 2 women), aged 24 to 39 years with phototypes 1-3, with distinct presentations of target nevi: halo, cockade, eczematous, and targetoid hemosiderotic nevi, detailing their clinical, dermoscopic, and RCM structures. Dermoscopy was performed using the FotoFinder medicam 1000 imaging system, and RCM was performed using the VivaScope 1500. We report 4 different benign melanocytic nevi, termed target nevi: halo, cockade, eczematous, and targetoid hemosiderotic. The halo nevus, also known as Sutton nevus,3 presents as a pigmented lesion located on the patient's lower back, surrounded by a peripheral white halo. Dermoscopically, the nevus exhibits a globular pattern, surrounded by a white rim of depigmentation. RCM mosaic image shows dense bright nests at the dermoepidermal junction (DEJ) and in the dermis (Figure 1 A, B, C). The cockade nevus, located on the patient's neck, features a central pigmented papular nevus,4 surrounded by a depigmented inner rim and a pigmented outer rim. Dermoscopically, the nevus exhibits a central globular pattern, a lighter homogeneous inner ring, and a peripheral darker reticular ring. RCM mosaic image shows, at the level of the DEJ, a central dense nest and a ringed pattern at the periphery (Figure 2 D, E, F). The eczematous nevus,1 also known as Meyerson's phenomenon, presents as an eczematous halo surrounding a pigmented nevus, located on the patient's back. Clinically, it appears as a small brown papule with an erythematous halo and evident overlying scales. Dermoscopically, the phenomenon does not modify the characteristics of the nevi, maintaining a reticular pattern, although it may appear blurred due to yellowish serocrusts. RCM mosaic image shows roundish to oval spaces in the epidermis filled with small bright round particles, indicative of inflammatory cells (Figure 3 A, B, C). The targetoid hemosiderotic nevus5 was reported by the patient as a sudden change in the pigmentation of a preexisting nevus, clinically resulting in an asymptomatic, violaceous, ecchymotic halo surrounding a flat central nevus. Dermoscopically, the lesion shows a homogeneous pattern with hemorrhagic vascular features, ranging from red to purple, superimposed on and surrounding the nevus. RCM mosaic image reveals the presence of a ringed pattern at the level of the DEJ (Figure 4 D, E, F). Recognizing the clinical, dermoscopic, and RCM features of melanocytic nevi with special features is crucial for improving diagnostic accuracy in unusual clinical and dermoscopic cases. This recognition helps to avoid unnecessary excisions in cases that are frequently misdiagnosed as melanoma.
Inês Stafin
ORCID: 0000-0003-0518-0066
Preparation and writing of the manuscript; acquisition, analysis and interpretation of data; critical review of the literature; critical revision of the manuscript.
Flávia Vieira Brandão
ORCID: 0000-0003-3809-9774
Conception and design of the study; acquisition, analysis and interpretation of data; critical review of the literature; critical revision of the manuscript.
Ana Maria Costa Pinheiro
ORCID: 0000-0002-7804-3567
Author contribution: Approval of the final version of the manuscript; conception and design of the study; acquisition, analysis and interpretation of data; effective participation in the conduct of the study; critical review of the literature; critical revision of the manuscript.
1. Larre Borges A, Zauladek I, Longo C, Dufrechou L, Argenziano G, Lallas A et al. Melanocytic nevi with special features: clinical-dermoscopic and reflectance confocal microscopic- findings. J Eur Acad Dermaol Venereol 2014;28(7):833-45.
2. Porto AC, Blumetti TP, Castro RPR, Pinto CALP, Mendes ASPM, Duprat Neto, et al. Recurrent halo nevus: dermoscopy and confocal microscopy features. J Am Acad Dermatol Case reports. 2017;3(3):256-8.
3. Aouthmany M, Mhsa BS, Weinstein M, Zirwas JZ, Brodell RT. The natural history of halo nevi: a retrospective case series. J Am Acad Dermatol 2012;67(4):582-6.
4. Kessides MC, Puttgen KB, Cohen BA. No biopsy needed for eclipse and cockade nevi found on the scalps of children. Arch Dermatol 2009;145(11);1334-6.
5. Patrizi A, Giacomini F, Savoia F, Miscialli C, Neri I. Targetoid hemosiderotic naevus. J Am Acad Dermatol. 2009;23(4):493-4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}