


Rogerio Nabor Kondo; Barbara Messias Pereira; Bianca Miyazawa; João Marcos Franco de Souza; Marina Gubert
Funding: None.
Conflicts of interest: None.
Submitted on: 28/04/2024
Approved on: 08/08/2024
How to cite this article: Kondo RN, Pereira BM, Miyazawa B, Souza JMF, Gubert M. Keloid surgery on the earlobe by total excision with fistulectomy: two case reports. Surg Cosmet Dermatol. 2025;17:e20250367.
Several surgical techniques are available for the treatment of keloids on the earlobes. Depending on the size, depth, duration, and morphology of the lesion, the procedure can pose significant challenges for the dermatologic surgeon, as these factors are associated with a higher risk of recurrence and local deformities. We report two cases in which total excision with fistulectomy was performed, yielding favorable aesthetic outcomes.
Keywords: Keloid; Ear; Case Reports; Ambulatory Surgical Procedures.
Keloids are benign, dense, and disorganized overgrowths of type I and III collagen fibers that develop in response to skin trauma.1 Earlobe keloids (ELK) are relatively common and may affect up to 2.5% of individuals who wear earrings in this region.2 The surgical removal of ELK can be challenging for dermatologic surgeons due to high recurrence rates, the potential for unaesthetic scarring, and the risk of local disfigurement.3
Several treatment options are available, including partial or total excision, intralesional corticosteroids, excision combined with corticosteroid injection, cryotherapy, silicone sheeting, pressure dressings, immunosuppressive or antitumor agents, laser therapy, and radiotherapy.2,3 Combined therapies have demonstrated better outcomes and lower recurrence rates compared to monotherapy.2
We report two cases in which patients underwent multiple sessions of intralesional triamcinolone followed by total excision with fistulectomy, resulting in satisfactory cosmetic outcomes. The aim of this case report is to illustrate a possible surgical approach for treating ELK that yielded high patient satisfaction.
Two patients with ELK were treated. Both received monthly intralesional injections of triamcinolone (10 mg), totaling four applications prior to surgery.
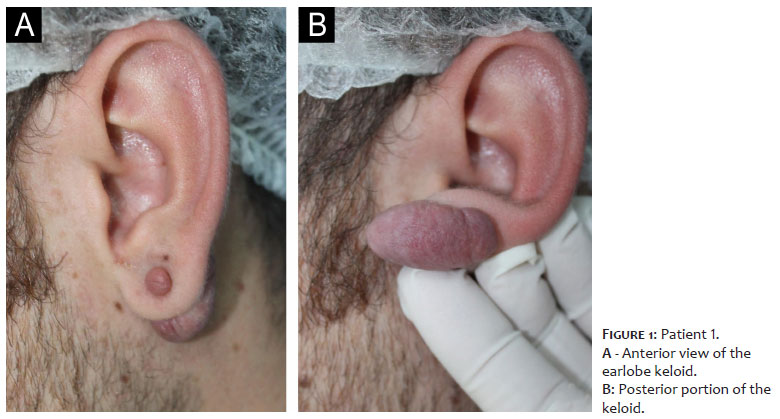
Patient 1: Male, 23 years old, White, presented with a 9-millimeter (mm) papule connected to a 35 mm plaque on the anterior and posterior aspects of the left earlobe, respectively (Figure 1).
The patient was placed in the right lateral decubitus position.
Antisepsis was performed using 10% topical povidone-iodine.
Sterile surgical drapes were applied.
Local infiltrative anesthesia was administered with 2% lidocaine containing a vasoconstrictor.
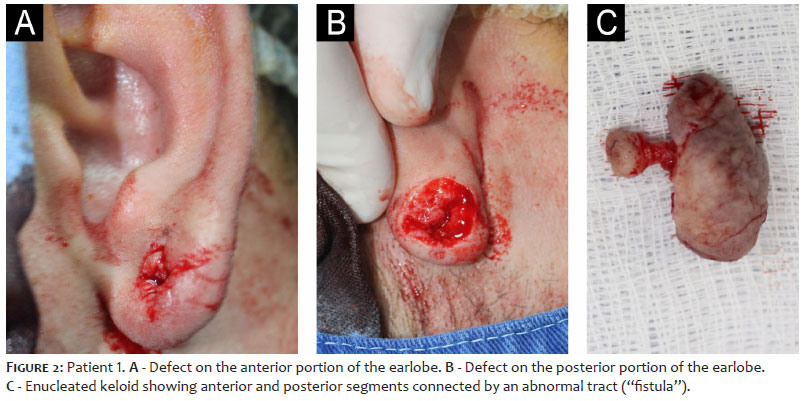
An incision was made with a no. 15 scalpel blade on the anterior portion of the keloid, followed by full-thickness excision through the earlobe (fistulectomy) extending to the posterior region. The keloid was removed en bloc (Figure 2).
Hemostasis was achieved.
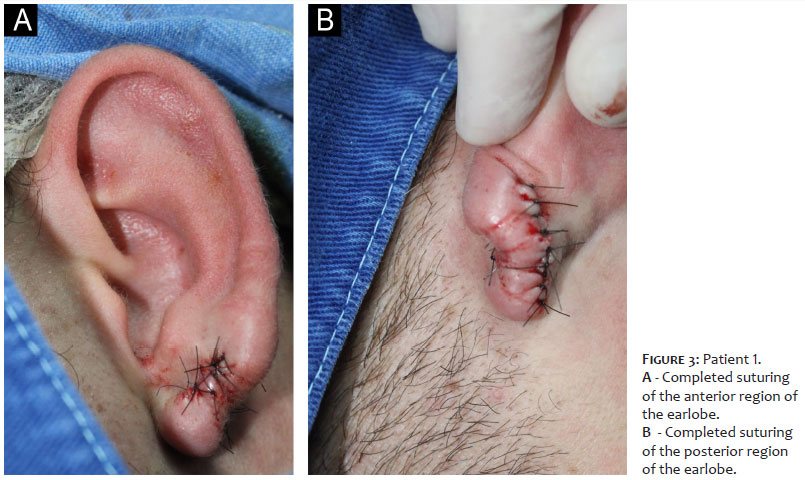
The wound was closed using simple interrupted sutures with 5-0 mononylon on both the anterior and posterior aspects of the left earlobe (Figure 3).
An additional intralesional injection of triamcinolone (10 mg) was administered (Figure 2).
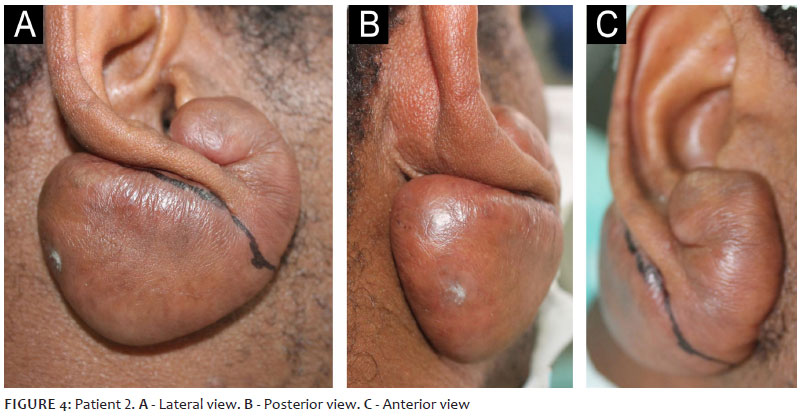
Patient 2: Male, 47 years old, Brown, presented with a 33-millimeter (mm) plaque on the anterior aspect of the right earlobe, connected to a 54 mm plaque on the posterior aspect (Figure 4).
The patient was placed in the left lateral decubitus position.
Antisepsis was performed using 10% topical povidone-iodine.
Sterile surgical drapes were applied.
Local infiltrative anesthesia was administered with 2% lidocaine containing a vasoconstrictor.
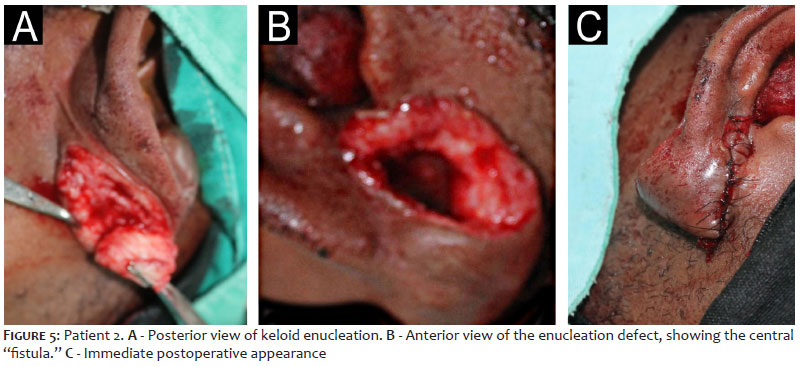
An incision was made with a no. 15 scalpel blade on the anterior portion of the keloid, followed by full-thickness excision through the earlobe (fistulectomy) extending to the posterior region. The keloid was removed en bloc (Figure 5).
Hemostasis was achieved.
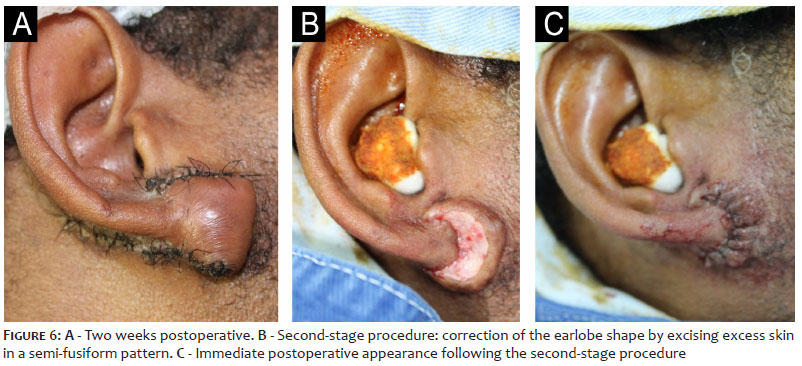
The wound was closed using simple interrupted sutures with 5-0 mononylon on both the anterior and posterior aspects of the left earlobe (Figures 6A and 6B).
An additional intralesional injection of triamcinolone (10 mg) was administered.
A second-stage procedure was performed three weeks later to correct the earlobe shape. This involved excision of a semi-fusiform strip of skin, followed by closure with simple interrupted sutures using 5-0 mononylon.
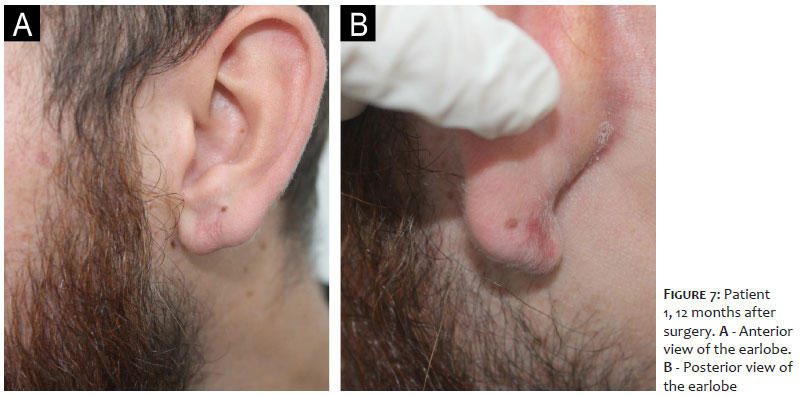
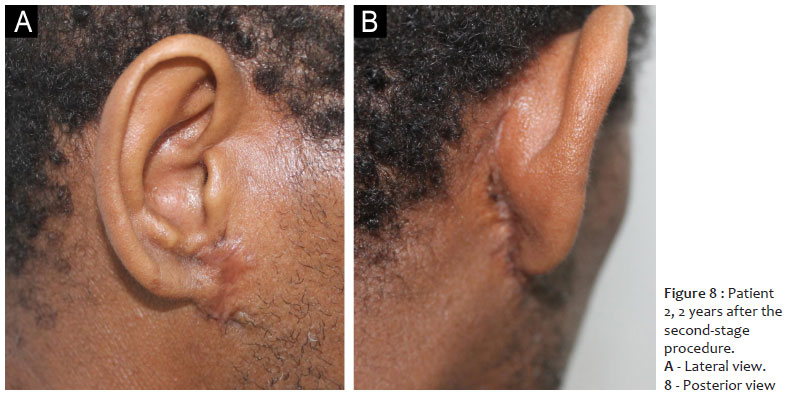
Both patients had an uneventful recovery during the early postoperative period. Wound healing was satisfactory, and the late postoperative phase showed good aesthetic outcomes (Figures 7 and 8).
Earlobes are common sites for keloid formation. The management of ELK can be particularly challenging for dermatologic surgeons, especially when the lesion exceeds 2 cm in size, due to the increased risk of anatomical deformity.3 Monotherapy is associated with higher recurrence rates, ranging from 40% to 100%. Combined treatments involving corticosteroids, pressure earrings, radiotherapy, and surgical excision appear to reduce recurrence rates.2
Some surgical techniques preserve the keloid margins through intralesional excision, aiming to avoid injury to surrounding non-keloidal skin and the deep dermis, focusing instead on removing only the central, most proliferative fibroblastic component. However, current literature does not provide sufficient evidence that this approach is superior to extralesional (total) excision.1
In 2015, Zhu et al. described the use of total excision with fistulectomy. This technique involves complete removal of the lesion and a full-thickness incision through the earlobe (anteroposterior perforation) at the site of the abnormal connection between the anterior and posterior portions of the keloid — the so-called "fistula" and the keloid core. In their study, 11 ELKs were treated, and no recurrences were observed after 12 months.3
In the present report, we replicated the total excision with fistulectomy technique in two cases. Based on this experience, we suggest that in ELKs larger than 50 mm — such as in Case 2 — excess skin should not be removed during the initial procedure to avoid anatomical distortion. Lobe reshaping should be performed after 3 weeks. In both cases, four monthly intralesional triamcinolone injections were administered prior to surgery, as well as an additional dose during the procedure. The objective was to suppress inflammatory processes and mitigate secondary effects such as collagen and glycosaminoglycan synthesis as well as to inhibit growth factors that may contribute to keloid recurrence.2
Radiotherapy is also a recognized adjuvant treatment for ELK surgery,4,5 helping control fibroblast proliferation, disrupt the cell cycle, and induce premature cellular senescence. Although it can be combined with intraoperative corticosteroid injections, it was not used in these cases due to its limited availability and high cost.
Neither patient experienced recurrence: Patient 1 at 1 year and Patient 2 at 2 years of follow-up. Although Patient 2 had a visibly smaller earlobe postoperatively, he reported satisfaction with the aesthetic outcome and an improvement in quality of life, having previously experienced distress due to the appearance of the keloid.
Despite the existing knowledge of extralesional excision with fistulectomy for ELK, few cases have been reported in the literature. Based on our experience, we consider this surgical technique a viable, effective treatment option, as demonstrated in the two cases presented.
Total excision with fistulectomy combined with adjuvant corticosteroid infiltration appears to be a promising treatment option for ELK, providing satisfactory aesthetic outcomes.
Rogerio Nabor Kondo
ORCID: 0000-0003-1848-3314
Final approval of the manuscript, study conception and design, manuscript drafting and writing, active participation in research supervision, intellectual contribution to the diagnostic and/or therapeutic management of the cases, critical manuscript revision
Barbara Messias Pereira
ORCID: 0000-0002-1180-7438
Final approval of the manuscript, manuscript drafting and writing, critical literature review, critical manuscript revision
Bianca Miyazawa
ORCID: 0009-0003-0561-8504
Final approval of the manuscript, manuscript drafting and writing, critical literature review, critical manuscript revision
João Marcos Franco de Souza
ORCID: 0000-0002-9297-7841
Final approval of the manuscript, manuscript drafting and writing, critical literature review, critical manuscript revision
Marina Gubert
ORCID: 0000-0002-9293-5019
Final approval of the manuscript, manuscript drafting and writing, critical literature review, critical manuscript revision
1. Olewinski L, Khodaee M. Posterior Earlobe Mass. Am Fam Physician. 2018;98(10):603-4.
2. Mascarenhas MRM, Paiva JMG, Mutti LA, Vivan MM, Yarak S. Efeito da terapia combinada no tratamento do queloide auricular. Surg Cosmet Dermatol 2015;7(3):253-6.
3. Zhu Z, Shan Y, Ying L, Zheng J, Mohamed S, Ma Z. Complete earlobe keloid resection with fistulectomy. Dermatol Surg. 2015;41(1):83-6.
4. Ekstein SF, Wyles SP, Moran SL, Meves A. Keloids: a review of therapeutic management. Int J Dermatol. 2021;60(6):661-71.
5. Cheraghi N, Cognetta A Jr, Goldberg D. Radiation therapy for the adjunctive treatment of surgically excised keloids: a review. Clin Aesthet Dermatol. 2017;10(8):12-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}