


Yara Martins Ortigosa Leonardo1; Luciena Cegatto Martins Ortigosa1; Edmundo Pereira de Souza Neto2,3
Funding: None.
Conflict of interest: None.
Submission date: 07/20/2024
Final decision: 02/14/2025
How to cite this article: Leonardo YMO, Ortigosa LCM, Souza Neto EP. Double-blind randomized trial comparing commercial and compounded topical anesthetics for diode laser hair removal. Surg Cosmet Dermatol. 2025;17:e20250391.
INTRODUCTION: The demand for laser procedures in dermatology is increasing, and topical anesthetics are widely used to reduce pain, enhance patient comfort, and improve treatment outcomes. Despite their frequent use, the evaluation of pain perception during diode laser hair removal using topical anesthetics has not been extensively studied.
OBJECTIVE: This study aimed to compare the analgesic effects of a commercial 4% lidocaine formulation (Dermomax ®, Aché Pharmaceutical Company, São Paulo, Brazil) with a compounded formulation containing 23% lidocaine and 7% tetracaine (Artpharma Pharmaceutical Company, São Paulo, Brazil) during LightSheer® diode laser hair removal procedures.
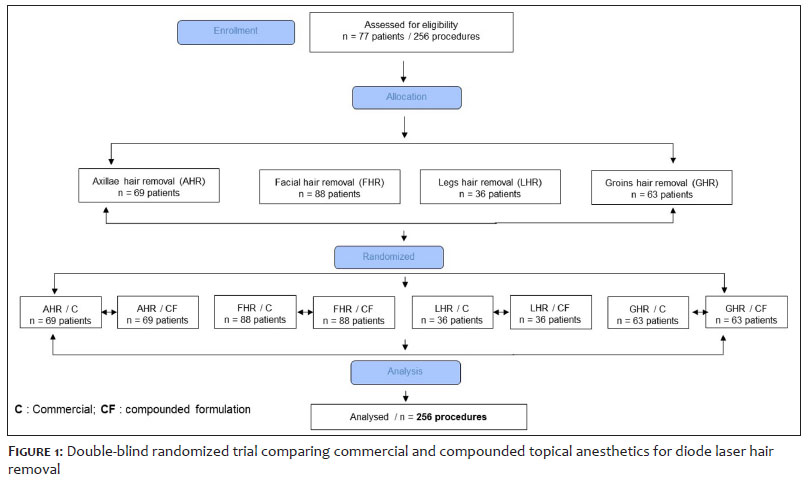
METHODS: A total of 74 women aged between 14 and 65 years underwent a total of 256 laser hair removal procedures. Sixty minutes before the procedure, the two anesthetic formulations were applied: the commercial 4% lidocaine on one half of the treatment area, and the compounded 23% lidocaine with 7% tetracaine on the other half. The treated areas included axillae, face, legs, and groin. The side of the body on which each formulation was applied, as well as the side to be treated first with the laser, were randomly assigned in a double-blind manner. Pain intensity was assessed using a Visual Analog Scale (VAS). Data were analyzed by comparing VAS scores across the different treatment areas.
RESULTS: Statistically significant differences in pain perception were found in all evaluated regions. The compounded formulation resulted in lower pain scores compared to the commercial formulation. No adverse effects were reported.
CONCLUSIONS: The compounded anesthetic formulation containing 23% lidocaine and 7% tetracaine was more effective in providing analgesia than the commercial 4% lidocaine product (Dermomax®) for diode laser hair removal.
Keywords: Pain; Anesthetics; Laser Therapy.
INTRODUCTION: The demand for laser procedures in dermatology is increasing, and topical anesthetics are widely used to reduce pain, enhance patient comfort, and improve treatment outcomes. Despite their frequent use, the evaluation of pain perception during diode laser hair removal using topical anesthetics has not been extensively studied.
OBJECTIVE: This study aimed to compare the analgesic effects of a commercial 4% lidocaine formulation (Dermomax ®, Aché Pharmaceutical Company, São Paulo, Brazil) with a compounded formulation containing 23% lidocaine and 7% tetracaine (Artpharma Pharmaceutical Company, São Paulo, Brazil) during LightSheer® diode laser hair removal procedures.
METHODS: A total of 74 women aged between 14 and 65 years underwent a total of 256 laser hair removal procedures. Sixty minutes before the procedure, the two anesthetic formulations were applied: the commercial 4% lidocaine on one half of the treatment area, and the compounded 23% lidocaine with 7% tetracaine on the other half. The treated areas included axillae, face, legs, and groin. The side of the body on which each formulation was applied, as well as the side to be treated first with the laser, were randomly assigned in a double-blind manner. Pain intensity was assessed using a Visual Analog Scale (VAS). Data were analyzed by comparing VAS scores across the different treatment areas.
RESULTS: Statistically significant differences in pain perception were found in all evaluated regions. The compounded formulation resulted in lower pain scores compared to the commercial formulation. No adverse effects were reported.
CONCLUSIONS: The compounded anesthetic formulation containing 23% lidocaine and 7% tetracaine was more effective in providing analgesia than the commercial 4% lidocaine product (Dermomax®) for diode laser hair removal.
Keywords: Pain; Anesthetics; Laser Therapy.
RESUMO
INTRODUÇÃO: A busca por procedimentos a laser em dermatologia é crescente e os anestésicos tópicos são amplamente utilizados para reduzir a dor, oferecendo conforto e melhores resultados no tratamento. Apesar desse uso comum, a avaliação da percepção da dor durante o laser com anestésicos tópicos para depilação não foi amplamente estudada.
OBJETIVO: O objetivo deste estudo foi comparar o efeito analgésico da lidocaína comercial a 4% (Dermomax® Aché farmacêutica, São Paulo, Brasil) e da formulação magistral de lidocaína a 23% associada a tetracaína a 7% (farmácia Artpharma, São Paulo, Brasil), utilizados em procedimentos com laser diodo LightSheer® para depilação.
MÉTODOS: Analisaram-se 77 pacientes num total de 256 procedimentos. Anestésicos tópicos foram aplicados 60 minutos antes do procedimento, sendo a lidocaína comercial a 4% aplicada de um lado e a formulação magistral do outro lado das áreas a serem tratadas: axilas, face, pernas ou virilha. O lado do corpo em que o laser deveria ser aplicado primeiro foi escolhido aleatoriamente, como num estudo duplo-cego. A intensidade da dor foi avaliada através da utilização da escala visual analógica.
RESULTADOS: Houve diferença estatisticamente significativa em todas as regiões corporais avaliadas. Os dados sugerem que a formulação anestésica magistral proporcionou maior alívio da dor em comparação à comercial. Não houve efeitos colaterais no estudo.
CONCLUSÃO: O uso da formulação magistral é mais eficiente na produção de analgesia do que a lidocaína comercial a 4%.
Palavras-chave: Dor; Anestésicos; Terapia a Laser.
The term "laser" stands for "light amplification by stimulated emission of radiation." In practical terms, lasers are devices that generate electromagnetic radiation with specific characteristics and have a wide range of applications in dermatology.1 Their variety of wavelengths makes these systems highly versatile for procedures such as hair removal, skin rejuvenation, treatment of vascular lesions, and removal of pigmented lesions and tattoos.2
Unwanted hair growth is a common cosmetic concern for both men and women. In recent years, laser hair removal has emerged as a highly effective, long-lasting solution with minimal side effects.3 Among the lasers used for epilation are the ruby (695 nm), alexandrite (755 nm), diode (800 nm), and Nd:YAG (1064 nm). The most widely used diode laser for hair removal is the LightSheer®, manufactured by Lumenis® (Santa Clara, California, USA), which emits energy in the 800-810 nm range of the electromagnetic spectrum.3 It offers a selectable pulse duration between 5 and 400 ms and fluences ranging from 10 to 100 J/cm2.
The LightSheer® laser has been shown to be a highly effective method for hair removal. Like other long-pulse lasers, it operates based on the principle of selective photothermolysis, which targets specific tissue structures while minimizing damage to surrounding tissue.4,5
The number of cosmetic and surgical procedures has grown considerably, along with the demand for effective, fast, and safe methods of analgesia. This trend has led to an increased use of topical anesthetics in such procedures to enhance patient comfort and improve treatment outcomes.6 Many topical anesthetics are available for use prior to minor outpatient procedures and laser treatments.6-8
Adverse events depend on the chemical structure and concentration of the anesthetic, the extent of application, and the duration of skin contact. Topical anesthetics may trigger type I (immediate hypersensitivity) or type IV (contact dermatitis) allergic reactions.6 Systemic complications can result from toxic effects on the central nervous and cardiovascular systems, especially when high concentrations are applied over large areas, leading to rapid systemic absorption. These reactions may include agitation, paresthesia, metallic taste, nausea, vomiting, disorientation, tremors, loss of consciousness, atrioventricular block, bradycardia, and seizures, and may progress to respiratory depression, coma, hypotension, heart failure, and death.6,9
Lidocaine is an amide-type anesthetic that rarely causes severe allergic reactions. However, systemic absorption may lead to dose-dependent adverse effects.6,9-10 Tetracaine, an ester-type anesthetic, is more lipophilic than lidocaine and prilocaine, allowing it to penetrate the cornea more effectively and form deposits that are released gradually. This reduces systemic absorption and prolongs the anesthetic effect.8-9 Allergic contact reactions to ester anesthetics are relatively common.8-9 Tetracaine is hydrolyzed in the dermis by nonspecific tissue esterases into para-aminobenzoic acid (PABA), which is responsible for many of these reactions. Its use on mucous membranes is not recommended due to the lack of safety data.6,9-10
The ideal topical anesthetic should provide effective anesthesia within a short period, act on intact skin, and avoid both systemic and local adverse effects or discomfort. These pharmacological characteristics are found in commercially available eutectic and liposomal formulations, although only at lower concentrations.9,11 In contrast, compounded formulations containing higher concentrations of ester- and amide-type anesthetics have been used in cosmetic procedures to achieve stronger anesthetic effects. However, there are no comparative studies to confirm whether these higher-concentration combinations are more effective. As such, these agents and their formulations require further investigation.
The aim of this study was to compare the analgesic effects of a commercial 4% lidocaine formulation (Dermomax®, Aché Pharmaceutical Company, São Paulo, Brazil) and a compounded formulation containing 23% lidocaine and 7% tetracaine (Artpharma Pharmaceutical Company, São Paulo, Brazil) in patients undergoing hair removal with the LightSheer® diode laser.
This study was conducted at a private dermatology clinic over a period of 2 years. Following approval by the Research Ethics Committee (protocol number 1255) and the signing of informed consent forms, we performed a randomized, controlled, blinded trial with a single operator. Adult patients undergoing hair removal procedures on one or more of the following body areas were included: axillae, face, legs, and groin (trial registration: RBR-373nm7). A single patient could undergo multiple sessions and have one or more areas treated.
Exclusion criteria included a history of allergic reactions to any of the products used in the study, the presence of keloids, or sun exposure within four weeks prior to treatment. After providing informed consent, eligible patients were referred for laser hair removal sessions using the LightSheer® diode laser device.
To eliminate potential bias in treatment techniques, all procedures were performed by the same dermatologist using identical laser settings. Randomization was conducted using sealed envelopes to determine which anesthetic formulation would be applied to each side of the body as well as which side would be treated first. Both the patient and the dermatologist were blinded to the treatment allocation. Double blinding was maintained throughout the study unless unblinding was deemed necessary for clinical reasons — which did not occur. The coordinating investigator remained blinded until the study was completed and ready for analysis.
A total of 60 minutes prior to the laser procedure, patients received a single oral dose of 10 mg ketorolac tromethamine (Toragesic®, Sigma Laboratories, São Paulo, Brazil). At the same time, the treatment area was cleansed with a mild emollient and water to remove any residues from moisturizers or other home-use products. Topical anesthetics were then applied in equal amounts (approximately 2 mm thick). The average treatment area was estimated to be less than 500 cm2 per patient, calculated using the surface area of the palm (excluding fingers).12
Commercial 4% lidocaine was applied to one half of the treatment area, and the compounded formulation containing 23% lidocaine and 7% tetracaine was applied to the other half. Treated regions included the axillae, face, legs, and groin. After 60 minutes, the anesthetics were removed, and the laser procedure was performed using identical parameters on both sides of each treatment area. Settings were individualized according to the body area, hair thickness and color, and the patient's Fitzpatrick skin type, with pulse durations ranging from 5 to 100 ms and fluences between 30 and 60 J/cm2. No cooling was used.
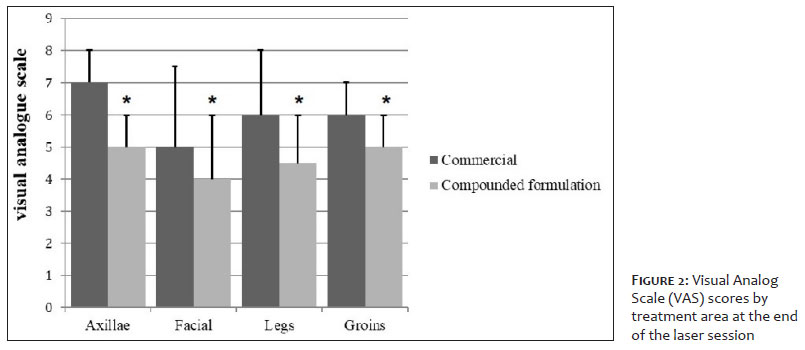
Pain intensity was assessed using the Visual Analog Scale (VAS). At the end of each session, patients were asked to rate their pain on a scale from 0 to 10, where 0 represented no pain and 10 indicated the highest level of pain. Data analysis was performed by comparing pain scores between the two sides of the body within the same treated area. Adverse events were monitored on the day of the procedure and again at a follow-up visit 2 days later. No significant changes were made to the study methods or outcome measures after the trial began.
Power analysis indicated that 80 procedures were required to detect a 1-point difference in VAS scores between the two products, with a 5% type I error rate, an 80% power, and a two-tailed test. Results were expressed as medians ± standard deviation (SD) of the median. The median absolute deviation (MAD), a variation of mean absolute deviation, was used because it is less influenced by outliers; extreme values have less impact on the median than on the mean. For datasets with extreme values, the MAD or interquartile range generally provides a more robust estimate of variability than the SD.
The nonparametric Wilcoxon signed-rank test was used to compare VAS scores. Qualitative variables were analyzed using Fisher's exact test. Linear correlations were assessed using Spearman's rank correlation coefficient. A p-value < 0.05 was considered statistically significant. All statistical analyses were performed by using StatView® for Windows (Abacus® Concepts Inc., Berkeley, CA, USA; version 4.57, 1996).
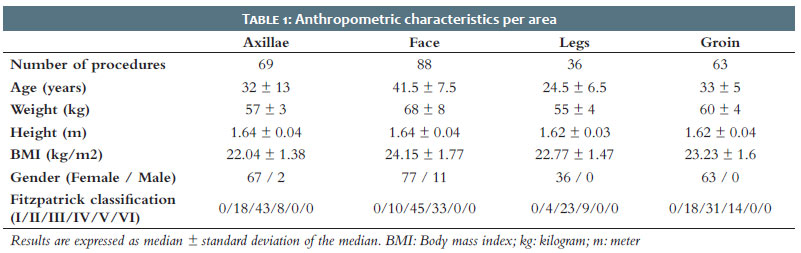
A total of 77 patients were included in the study, of whom 64 underwent more than one procedure. There were no losses or exclusions after randomization (Figure 1). Table 1 presents the patients' anthropometric characteristics according to the number of procedures performed per treatment area.
None of the participants had previously undergone light-based or laser therapy, and all were free of systemic diseases. Throughout routine follow-up, no adverse effects related to the laser procedure or topical anesthetics were reported by any patient.
A total of 256 laser hair removal procedures were performed, distributed across four body areas in the following manner: 69 axillary, 88 facial, 36 legs, and 63 groin treatments. A statistically significant difference in pain control was observed between the two anesthetic formulations used with the LightSheer® diode laser. The compounded formulation resulted in significantly lower pain scores compared to the commercial product, demonstrating greater anesthetic efficacy across all evaluated body regions (Figure 2).
Pain can reduce patient satisfaction and compromise the efficacy of laser procedures, often requiring the use of lower laser settings. Patients undergoing diode laser hair removal frequently report pain, described as burning or stinging sensations. This discomfort can be distressing for both the operator and the patient.
In our pain management approach, we combined topical anesthetic creams with ketorolac, a potent nonsteroidal anti-inflammatory drug (NSAID) with both anti-inflammatory and analgesic properties. Indeed, ketorolac pretreatment has been shown to be a safe, effective method for pain relief prior to procedures such as chemical peeling, without adverse reactions.13,14 The combination of topical anesthetics and NSAIDs can be useful in minimizing treatment-related discomfort. Topical anesthetics are painless to administer and reduce the risk of systemic exposure.15
A systematic review of noninvasive anesthetic methods for dermatologic laser procedures included several studies involving the use of topical anesthetics during laser hair removal.15-23 Although these agents were associated with pain reduction, the overall quality of evidence was low. Many studies failed to report or perform statistical analyses and did not provide p-values or confidence intervals.12 Additionally, randomization was not always employed, and blinding was often not feasible — particularly relevant since that pain is a subjective outcome measure.15
In addition to the low quality of existing studies, no previous research has compared commercial preparations to compounded formulations across different body regions. This gap underscores the relevance of our study, which statistically compared both anesthetic types across four body areas.
The anesthetics evaluated in our study were lidocaine and tetracaine. Tetracaine is a highly potent, long-acting ester-based anesthetic. Its prolonged action is due to its high hydrophobicity, which allows sustained interaction with sodium channel binding sites, conferring greater potency than lidocaine. In contrast, lidocaine is a moderately hydrophobic, amide-based anesthetic with a rapid onset of action and a moderate duration of effect (approximately 1-2 hours). It also has a lower risk of triggering allergic reactions.24
Compounded anesthetic formulations — such as the one evaluated in our study — are commonly used before dermatologic procedures to enhance anesthetic efficacy. These formulations allow for higher concentrations and combinations of multiple anesthetic agents.25,26 Our study assessed the efficacy of a compounded formulation containing 23% lidocaine and 7% tetracaine and found it to be superior to the commercial 4% lidocaine product (Dermomax®) in terms of pain control.
However, the use of high-concentration compounded topical anesthetics requires additional precautions. Reports of systemic toxicity have typically involved application of such formulations under occlusion to large surface areas.27 Some studies advise against applying large quantities, under occlusion, for extended durations, or on irritated or broken skin.28-30 Caution is also advised when using these formulations in conjunction with laser procedures — particularly resurfacing techniques.29 Moreover, it is recommended to use the same compounding pharmacy consistently to reduce variability in product composition.26
Although adverse events reported in research highlight the importance of proper education regarding the use and risks of compounded topical anesthetics, our study did not identify any side effects. These findings support the efficacy and apparent safety of the compounded formulation containing 23% lidocaine and 7% tetracaine when used appropriately.
This study presents several limitations. First, we did not measure plasma levels of lidocaine, monoethylglycinexylidide, or tetracaine. Elevated serum levels of lidocaine have been associated with higher topical concentrations, longer exposure times, larger application areas, and the use of occlusive dressings. Some studies suggest that combining ester- and amide-type anesthetics may present a higher risk of toxicity than combining two amides, such as lidocaine and prilocaine.32-34 However, Spiegel et al. found no evidence of synergistic central nervous system toxicity between lidocaine and tetracaine in a rat model.35
As noted by Oni et al. (2010), there is significant interindividual variability in lidocaine absorption through the skin. Moreover, systemic levels are not always directly correlated with the applied dose or exposure time.33 In our study, exposure time was minimized, no occlusive dressings were used, and the same compounding pharmacy was consistently employed to ensure formulation consistency. Additionally, a trained health professional — familiar with the warning signs of lidocaine toxicity — was present during all procedures and prepared to manage any adverse reactions. No clinical signs of toxicity were observed in any of the participants.
Second, this was a single-center study, which may limit the generalizability of the findings to other clinical settings. Third, the compounded formulation used in this study may differ from similar formulations prepared by other institutions. The efficacy of a topical anesthetic depends not only on concentration and dosage, but also on the vehicle used for delivery.30-32
The findings suggest that the compounded formulation containing 23% lidocaine and 7% tetracaine is more effective in providing analgesia across all treated areas compared to the commercial 4% lidocaine cream (Dermomax®). No allergic reactions or other adverse effects were observed during the study. Nevertheless, proper administration is essential to avoid potential, though rare, serious complications.
In conclusion, the compounded formulation of 23% lidocaine and 7% tetracaine proved to be an effective, noninvasive, well-tolerated option for topical anesthesia during laser hair removal. It represents a promising choice for patients who are likely to undergo repeated procedures requiring topical anesthesia.
Yara Martins Ortigosa Leonardo
ORCID: 0000-0001-9892-2887
Approval of final version of the manuscript, Study conception and planning, Manuscript preparation and writing, Data collection, analysis, and interpretation, Critical review of literature, Critical review of manuscript.
Luciena Cegatto Martins Ortigosa
ORCID: 0000-0002-3541-9456
Approval of final version of the manuscript, Study conception and planning, Manuscript preparation and writing, Data collection, analysis, and interpretation, Active participation in research supervision, Intellectual contribution to the diagnostic and/or therapeutic management of studied cases, Critical review of literature, Critical review of manuscript.
Edmundo Pereira de Souza Neto
ORCID: 0000-0001-6921-235X
Statistical analysis, approval of final version of the manuscript, Study conception and planning, Manuscript preparation and writing, Data collection, analysis, and interpretation, Active participation in research supervision, Intellectual contribution to the diagnostic and/or therapeutic management of studied cases, Critical review of literature, Critical review of manuscript.
1. Gianfaldoni S, Tchernev G, Wollina U, Fioranelli M, Roccia MG, Gianfaldoni R, et al. An overview of laser in dermatology: the past, the present and... the future (?). Open Access Maced J Med Sci. 2017;5(4):526-30.
2. Callaghan DJ 3rd, Bonati LM, Alam M, Jerdan K, Taylor MB, Dover JS. Sound levels and safety in cosmetic laser surgery. Lasers Surg Med. 2019;51(6):491-4.
3. Shapiro J, Lui H. Treatments for unwanted facial hair. Skin Therapy Lett. 2005;10(10):1-4.
4. Ataie-Fashtami L, Shirkavand A, Sarkar S, Alinaghizadeh M, Hejazi M, Fateh M, et al. Simulation of heat distribution and thermal damage patterns of diode hair-removal lasers: an applicable method for optimizing treatment parameters. Photomed Laser Surg. 2011;29(7):509-15.
5. Gan SD, Graber EM. Laser hair removal: a review. Dermatol Surg. 2013;39(6):823-38.
6. Sobanko JF, Miller CJ, Alster TS. Topical anesthetics for dermatologic procedures: a review. Dermatol Surg. 2012;38(5):709-21.
7. Kundu S, Achar S. Principles of office anesthesia: part II. Topical anesthesia. Am Fam Physician. 2002;66(1):99-102.
8. Boyce RA, Kirpalani T, Mohan N. Updates of topical and local anesthesia agents. Dent Clin North Am. 2016;60(2):445-71.
9. Lee HS. Recent advances in topical anesthesia. J Dent Anesth Pain Med. 2016;16(4):237-44.
10. Catterall W, Mackie K. Local anesthetics. In: Goodman & Gilman's editors. The pharmacological basis of therapeutics. New York: McGraw-Hill; 2006. p.369-86.
11. Lirk P, Picardi S, Hollmann MW. Local anaesthetics: 10 essentials. Eur J Anaesthesiol. 2014;31(11):575-85.
12. Scarisbrick JJ, Morris S. How big is your hand and should you use it to score skin in cutaneous T-cell lymphoma? Br J Dermatol. 2013;169(2):260-5.
13. Kim JH, Whang KK, Hahm JH. The Effect of Premedication with Ketorolac on Pain Relief During Chemical Peeling. Ann Dermatol. 2002;14(1):18-21.
14. Esparza-Villalpando V, Ortiz-Barroso G, Masuoka-Ito D. Evidence-based safety profile of oral ketorolac in adults: systematic review and meta-analysis. Pharmacol Res Perspect. 2024;12(6):e70033.
15. Greveling K, Prens EP, Liu L, Van Doorn MBA. Non-invasive anaesthetic methods for dermatological laser procedures: a systematic review. J Eur Acad Dermatol Venereol. 2017;31(7):1096-110.
16. Akinturk S, Eroglu A. Effect of piroxicam gel for pain control and inflammation in Nd:YAG 1064-nm laser hair removal. J Eur Acad Dermatol Venereol. 2007;21(3):380-3.
17. Akinturk S, Eroglu A. A clinical comparison of topical piroxicam and EMLA cream for pain relief and inflammation in laser hair removal. Lasers Med Sci. 2009;24(4):535-8.
18. Bernstein EF. Pneumatic skin flattening reduces pain during laser hair reduction. Lasers Surg Med. 2008;40(3):183-7.
19. Eremia S, Newman N. Topical anesthesia for laser hair removal: comparison of spot sizes and 755 nm versus 800 nm wavelengths. Dermatol Surg. 2000;26(7):667-9.
20. Guardiano RA, Norwood CW. Direct comparison of EMLA versus lidocaine for pain control in Nd:YAG 1,064 nm laser hair removal. Dermatol Surg. 2005;31(4):396-8.
21. Ke M. Pain inhibition with pneumatic skin flattening (PSF) in permanent diode laser hair removal. J Cosmet Laser Ther. 2007;9(4):210-2.
22. Nahm WK, Tsoukas MM, Falanga V, Carson PA, Sami N, Touma DJ. Preliminary study of fine changes in the duration of dynamic cooling during 755-nm laser hair removal on pain and epidermal damage in patients with skin types III-V. Lasers Surg Med. 2002;31(4):247-51.
23. Rashidi T, Hoseinzade N. Comparison of pain reduction between lidocaine-prilocaine cream and diclofenac gel in patients treated with the alexandrite laser. Iran J Dermatol 2012;15:109-10.
24. Becker DE, Reed KL. Local anesthetics: review of pharmacological considerations. Anesth Prog. 2012;59(2):90-101.
25. Railan D, Alster TS. Use of topical lidocaine for cosmetic dermatologic procedures. J Drugs Dermatol. 2007;6(11):1104-8.
26. Carruthers JA, Carruthers JD, Poirier J, Oliff HS, Mordaunt J, Schreiber WE. Safety of lidocaine 15% and prilocaine 5% topical ointment used as local anesthesia for intense pulsed light treatment. Dermatol Surg. 2010;36(7):1130-7.
27. Neal JM, Bernards CM, Butterworth JF 4th, Di Gregorio G, Drasner K, Hejtmanek MR, et al. ASRA practice advisory on local anesthetic systemic toxicity. Reg Anesth Pain Med. 2010;35(2):152-61.
28. Kapes B. Media microscope analyzes misuse of topicals. Dermatol Times 2005;26:22.
29. Kumar M, Chawla R, Goyal M. Topical anesthesia. J Anaesthesiol Clin Pharmacol. 2015;31(4):450-6.
30. Tayeb BO, Eidelman A, Eidelman CL, McNicol ED, Carr DB. Topical anaesthetics for pain control during repair of dermal laceration. Cochrane Database Syst Rev. 2017;2(2):CD005364.
31. Berkman S, MacGregor J, Alster T. Adverse effects of topical anesthetics for dermatologic procedures. Expert Opin Drug Saf. 2012;11(3):415-23.
32. McCleskey PE, Patel SM, Mansalis KA, Elam AL, Kinsley TR. Serum lidocaine levels and cutaneous side effects after application of 23% lidocaine 7% tetracaine ointment to the face. Dermatol Surg. 2013;39(1 Pt 1):82-91.
33. Oni G, Brown S, Burrus C, Grant L, Watkins J, Kenkel M, et al. Effect of 4% topical lidocaine applied to the face on the serum levels of lidocaine and its metabolite, monoethylglycinexylidide. Aesthet Surg J. 2010;30(6):853-8.
34. Oni G, Brown S, Kenkel J. Comparison of five commonly-available, lidocaine-containing topical anesthetics and their effect on serum levels of lidocaine and its metabolite monoethylglycinexylidide (MEGX). Aesthet Surg J. 2012;32(4):495-503.
35. Spiegel DA, Dexter F, Warner DS, Baker MT, Todd MM. Central nervous system toxicity of local anesthetic mixtures in the rat. Anesth Analg. 1992;75(6):922-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}