


Célia Luiza Petersen Vitello Kalil1,2; Augusto Casagrande1,3; Clarissa Reinehr1,4; Julia Frota Variani1
Funding: None.
Conflicts of interest: None.
Submitted on: 06/26/2024
Final decision: 07/25/2024
How to cite this article: Kalil CLPV, Casagrande A, Reinehr C, Variani JF. Late-onset complication after polymethyl methacrylate (PMMA) injections: diagnosis and treatment. Surg Cosmet Dermatol. 2025;17:e20250383.
At the beginning of dermal filler use, which started with fat grafts, a variety of products were tested for this purpose, from temporary to permanent fillers. The decision to use polymethyl methacrylate (PMMA) as a permanent dermal filler should be considered with caution.
Keywords: Polymethyl Methacrylate; Plastics; Cosmetic Industry.
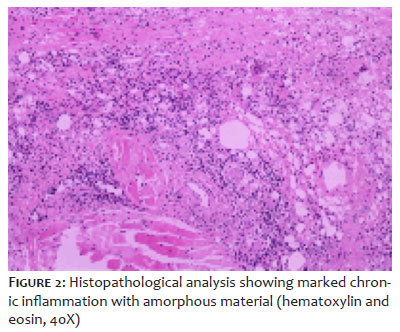
A 67-year-old woman presented with facial edema in areas previously treated with polymethyl methacrylate (PMMA) injections 16 years earlier by another physician (Figure 1). The patient reported that the edema had started 6 months previously, when she sought medical attention and was treated with antibiotics and corticosteroids, with poor clinical response. The patient was evaluated by a plastic surgeon for surgical removal of the PMMA, which was scheduled to be performed in two consecutive sessions. Histopathological analysis of the excised tissue revealed marked chronic inflammation with amorphous material, connective tissue fibrosis, and muscle and salivary accessory glands covered with squamous mucosa (Figure 2). Forty days after the first surgical session, the patient experienced a recurrence of edema and erythema, and an oral corticosteroid was restarted (prednisone 60 mg for 3 days, tapered to 40 mg for 7 days, 30 mg for 7 days, and finally 20 mg for 7 days). After the symptoms were controlled, the second procedure was performed. At the 2-year follow-up examination after completion of both procedures, the patient showed no signs of facial edema or erythema (Figure 3).
Following the initial use of dermal fillers, which started with fat grafts, a variety of products have been used for this purpose, from temporary to permanent fillers. PMMA is a low-cost thermoplastic material composed of microspheres suspended in a collagen matrix that offers long-lasting results. Within 1 to 3 months post-PMMA injection, the collagen carrier is absorbed, and new collagen is deposited by the host to encapsulate and engulf the remaining PMMA particles (fibroplasia).1,2 The main issue with PMMA is its permanence, which increases patient susceptibility to foreign body reactions, with an approximate 1.5% probability of granuloma formation, which can be triggered by systemic illness or orofacial infection/surgery. Treatment options for filler reactions include systemic anti-inflammatories, antibiotics, hyaluronidase, intralesional triamcinolone with 5-fluorouracil, and surgical excision.3 Our patient's clinical response to oral and intralesional corticosteroids was not sustained, prompting a discussion with the patient about the possibility of surgical removal of PMMA in an attempt to promote a sustained response. We identified only one previously published study that addressed the surgical excision of facial inflammatory nodules caused by PMMA. This retrospective review described 9 cases of periorbital PMMA nodules that were successfully treated with surgical excision, improving edema, erythema, and nodularity.4 The choice of PMMA injection as a dermal filler requires careful consideration, and nonpermanent fillers should generally be favored. Patients with a history of PMMA injections should be carefully evaluated before any subsequent cosmetic procedures, and imaging techniques should be used whenever possible, such as ultrasonography. It is also essential for dermatologists to be aware of the clinical management of PMMA injection complications and to refer patients to plastic surgeons for surgical removal if necessary.
Célia Luiza Petersen Vitello Kalil
ORCID: 0000-0002-1294-547X
Conception and design of the study, Intellectual participation in propaedeutic and/or therapeutic approach to studied cases, Critical review of the literature
Augusto Casagrande
ORCID: 0009-0008-3364-751X
Intellectual participation in propaedeutic and/or therapeutic approach to studied cases
Clarissa Reinehr
ORCID: 0000-0003-1811-4519
Approval of the final version of the manuscript, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in propaedeutic and/or therapeutic approach to studied cases
Julia Frota Variani
ORCID: 0000-0002-3420-6352
Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study
1. Ibrahim O, Dover JS. Delayed-onset nodules after polymethyl methacrylate injections. Dermatol Surg. 2018;44(9):1236-8.
2. Jones DH. Semipermanent and permanent injectable fillers. Dermatol Clin. 2009;27(4):433-44.
3. Christensen L, Breiting V, Janssen M, Vuust J, Hogdall E. Adverse reactions to injectable soft tissue permanent fillers. Aesthetic Plast Surg. 2005;29(1):34-48.
4. Limongi R, Tao J, Borba A, Pereira F, Pimentel A, Akaishi P, et al. Complications and management of polymethylmethacrylate (PMMA) injections to the midface. Aesthet Surg J. 2016;36(2):132-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}