


Ana Carolina Cechin de Mello; Rogerio Nabor Kondo; Betina Samesima e Singh; Airton dos Santos Gon
Funding: None.
Conflict of interest: None.
Submitted on: 10/22/2023
Final decision: 02/27/2025
How to cite this article: Mello ACC, Kondo RN, Samesina e Singh B, Gon AS. Giant Merkel cell carcinoma: report of an atypical case. Surg Cosmet Dermatol. 2025;17:e20250314.
Merkel cell carcinoma is a rare and aggressive cutaneous neuroendocrine cancer that occurs on sun-damaged skin in older White patients. It typically manifests as a solitary plaque or nodule in the head and neck region. We report an unusual presentation of Merkel cell carcinoma in a black patient who simultaneously developed two primary tumors located in the trunk region.
Keywords: Carcinoma, Merkel Cell; Immunohistochemistry; Neuroendocrine Tumors; Upper Extremity.
Dear Editor,
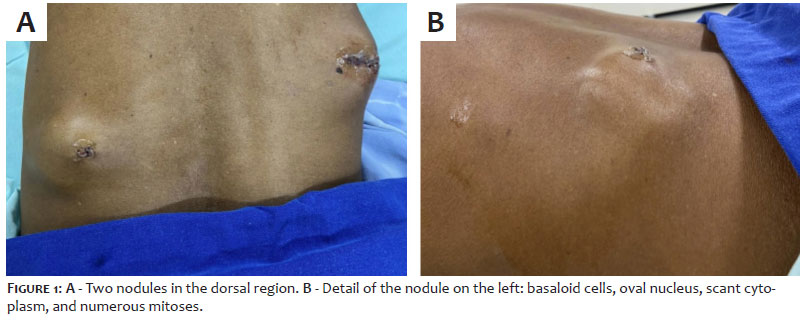
A 78-year-old black man, who works as a gardener, presented with two nodules on his back that had been rapidly growing over the past 3 months. He denied fever, weight loss, or other related symptoms. His medical history includes prostate adenocarcinoma, treated with an orchiectomy in 2019. Dermatological examination revealed two indurated nodules measuring 12 and 16 cm in the dorsal region (Figure 1), with no associated lymph node enlargement. Histopathological examination of both nodules revealed basaloid cells with oval nuclei, scant cytoplasm, and numerous mitoses, suggestive of Merkel cell carcinoma (MCC). Immunohistochemistry was positive for cytokeratin 20 (CK20) and negative for prostate-specific antigen (PSA) and thyroid/lung transcription factor-1 (TTF-1) (Figures 2 and 3).
MCC is a rare and aggressive neuroendocrine cancer that primarily affects sun-exposed skin in older White individuals, with a rare incidence in black individuals. It commonly appears as a solitary plaque or nodule on the head or neck.1,2 Although MCC accounts for less than 1% of all malignant skin tumors, it is the third leading cause of skin cancer-related deaths.2 It was first described by Toker et al. in 1972 as trabecular carcinoma of the skin, suggesting, at the time, a possible glandular origin. In 1978, the same authors identified electron-dense granules in the cytoplasm of tumor cells, indicating a neuroendocrine origin similar to epidermal Merkel cells.2 The pathogenesis of MCC remains unclear, but ultraviolet (UV) radiation, immunosuppression, and, recently, the presence of Merkel cell polyomavirus in the tumor genome appear to play key roles.2,3 The acronym "AEIOU" was developed to aid in considering a diagnosis of MCC, corresponding to: A = asymptomatic, E = expanding rapidly, I = immunosuppression, O = older than 50 years, and U = UV-exposed site.2 Histopathology shows a dermal lesion consisting of clusters of monomorphic, round, basophilic cells with large vesicular nuclei with finely granular chromatin, pyknotic nuclei, and abundant mitotic figures.4 While CK20 is a key immunohistochemical marker for diagnosis, it can be negative in up to 20% of cases.2 The TTF-1 marker is typically positive in lung and thyroid cancers, and a negative result can support the diagnosis of MCC.2 The differential diagnosis for MCC includes epidermal cysts, dermatofibroma, basal cell carcinoma, squamous cell carcinoma, amelanotic melanoma, lymphoma, skin metastases, and adnexal tumors.2 Staging, for determining prognosis and treatment strategies, adheres to the American Joint Committee on Cancer criteria: stage 1 (primary tumor < 2 cm); stage 2 (primary tumor ≥ 2 cm); stage 3 (regional lymph node involvement); and stage 4 (distant metastasis).2 Surgical excision with 1 cm margins is the treatment of choice. Inoperable or recurrent tumors can be treated with radiotherapy. Chemotherapy serves as a palliative treatment option for patients in stage 4.5 In the case reported here, tomography revealed bone metastases and lymph node involvement in the mediastinum, pelvis, and abdomen. However, no neuroendocrine tumor was identified at any other site or primary focus. The two lesions observed in this case are presumed to be synchronous due to their concurrent appearance without a known primary focus and their size. Nevertheless, the authors do not rule out the possibility that these are two metastases originating from an undetected primary tumor, given the patient's stage 4 presentation and the extremely aggressive nature of MCC, which often metastasizes even from small primary lesions. Regardless, this case has an unusual presentation, with the emergence of two large synchronous lesions in a black individual. The patient has been referred to an oncology hospital in the city for chemotherapy treatment.
Ana Carolina Cechin de Mello
ORCID: 00009-0007-6862-6287
Preparation and writing of the manuscript, effective participation in the conduct of the study, intellectual participation in propaedeutic and/or therapeutic approach to studied cases, critical review of the literature.
Rogerio Nabor Kondo
ORCID: 0000-0003-1848-3314
Approval of the final version of the manuscript, conception and design of the study, preparation and writing of the manuscript, acquisition, analysis and interpretation of data, effective participation in the conduct of the study, intellectual participation in propaedeutic and/or therapeutic approach to studied cases, critical review of the literature, critical revision of the manuscript.
Betina Samesima e Singh
ORCID: 0000-0002-6055-0341
Acquisition, analysis and interpretation of data, effective participation in the conduct of the study, critical review of the literature, critical revision of the manuscript.
Airton dos Santos Gon
ORCID: 0000-0003-1219-5581
Approval of the final version of the manuscript, conception and design of the study, effective participation in the conduct of the study, intellectual participation in propaedeutic and/or therapeutic approach to studied cases, critical revision of the manuscript.
1. Coggshall K, Tello TL, North JP, Yu SS. Merkel cell carcinoma: An update and review: Pathogenesis, diagnosis, and staging. J Am Acad Dermatol. 2018;78(3):433-42.
2. Llombart B, Requena C, Cruz J. Atualização em carcinoma de células de Merkel: Epidemiologia, etiopatogenia, características clínicas, diagnóstico e estadiamento. Actas Dermosifiliogr. 2017;108(2):108-19.
3. Góes HFO, Lima CS, Issa MCA, Luz FB, Pantaleão L, Paixão JGM. Carcinoma de células de Merkel em um paciente imunossuprimido. An Bras Dermatol. 2017;92(3):395-7.
4. Walsh NM, Cerroni L. Merkel cell carcinoma: a review. J Cutan Pathol. 2021;48(3):411-21.
5. Tétu P, Baroudjian B, Madelaine I, Delyon J, Lebbé C. Update in treatment for Merkel cell carcinoma and clinical practice guide. Bull Cancer. 2019;106(1):64-72.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}