


Rebecca Ignacio Subirá Medina; Gladstone Eustáquio de Lima Faria; Ricardo Frota Boggio
Funding support: None.
Conflict of interest: None.
Submitted on: 10/31/2023
Approved on: 07/04/2024
How to cite this article: Medina RIS, Faria GEL, Boggio RF. Eyebrow lift with cosmetic procedures: how to approach it. Surg Cosmet Dermatol. 2024;16:e20240318.
Eyebrow ptosis presents a significant challenge for cosmetic professionals. Minimally invasive procedures can improve eyebrow positioning; however, a thorough understanding of its varied etiologies is essential. The primary causes include skin laxity, muscular dysfunction, and tissue deflation, with the latter subdivided into frontal, temporal, and superciliary deflation. A precise diagnosis allows for the appropriate indication of microfocused ultrasound, botulinum toxin, biostimulators, and hyaluronic acid-based fillers, either as standalone treatments or in combination. At the end of this review, a treatment algorithm for eyebrow ptosis is proposed.
Keywords: Dermal Fillers; Botulinum Toxins; Eyebrows; Aesthetic Equipment.
In 1974, Westmore1 outlined the characteristics of the ideal eyebrow, and since then, various authors have sought to describe, in a more objective manner, what makes an eyebrow aesthetically appealing.2-4 Generally, these attributes play a significant role in facial beauty, particularly due to their ability to convey emotions and express individual identity.
Among the many changes that occur in this anatomical region with aging, eyebrow ptosis—especially affecting the lateral portion—stands out. It often imparts subjective impressions of fatigue and sadness, serving as a distinct hallmark of advanced age and contributing to a less attractive appearance.
Regarding its etiology, eyebrow ptosis may result from paralysis of various origins or occur as a natural part of the aging process. In the latter case, ptosis arises from a combination of structural changes affecting multiple layers of facial anatomy, including: 1) skin laxity; 2) the interplay of muscular traction forces; and 3) tissue deflation and bone resorption.
Through a comprehensive literature review, this study aims to provide a deeper understanding of the aging process in the periorbital region, with a particular focus on eyebrow ptosis, as well as to propose a treatment protocol tailored to its primary etiologies.
In the quest to define ideal parameters for eyebrow shape and positioning, opinions among authors vary, and aesthetic criteria are not unanimously established in literature.5,6 The optimal arch position has been extensively debated,3,4,7–9 with most authors advocating that it should be positioned: 1) along a vertical line tangent to the lateral limbus of the iris1; 2) halfway between the lateral limbus of the iris and the lateral canthus of the eye2,10; or 3) above the lateral canthus of the eye.8
Most authors agree that male eyebrows should be straighter, without any noticeable arch.10 While some researchers suggest that the medial and lateral ends of female eyebrows should be at the same height,11 the prevailing consensus is both should be positioned above the supraorbital margin, with the lateral portion slightly higher than the medial. Conversely, male eyebrows are typically positioned along the supraorbital margin, appearing straighter, with the lateral end at the same level or just slightly above the medial end, and a uniform distribution of volume along their entire length.12
Studies assessing individual preferences for different eyebrow shapes have yielded varied results.4,13,14 Interestingly, many of these studies found that participants within the same age group shared similar aesthetic preferences.13,14
Regarding age-related changes in eyebrow positioning, some researchers have reported an increase in height along the mediopupillary line,1,15 while others found no significant change in eyebrow height,15,16 and some described a descent of the lateral portion.15
A literature search was performed on PubMed. The search terms and filters applied were as follows: (("Eyebrow"[Title/Abstract] OR "Eyebrows"[Title/Abstract] OR "Brow"[Title/Abstract] OR "Brows"[Title/Abstract] OR "Periorbital"[Title/Abstract] OR "upper third"[Title/Abstract] OR "upper face" [Title/Abstract] OR "Orbital"[Title/Abstract] OR "Temple" [Title/Abstract] OR "temples"[Title/Abstract] OR "Frontal" [Title/Abstract] OR "Forehead"[Title/Abstract] OR "upper third"[Title/Abstract]) AND ("botulinum toxin"[Title/Abstract] OR "botulinum toxins"[Title/Abstract] OR "botulinum neurotoxin a"[Title/Abstract] OR ("Sculptra"[Title/Abstract] OR "Radiesse"[Title/Abstract] OR "calcium hydroxyapatite"[Title/Abstract] OR "biostimulation"[Title/Abstract] OR "poly-lactic- acid"[Title/Abstract]) OR ("hyaluronic acid"[Title/Abstract] OR "dermal filler"[Title/Abstract] OR "dermal fillers"[Title/Abstract] OR "Filler"[Title/Abstract] OR "Fillers"[Title/Abstract]))) AND ((y_10[Filter]) AND (review[Filter] OR systematic review[Filter])).
This search retrieved 145 publications, which were screened based on their abstracts to assess their relevance to the theme of this article. Additionally, bibliographic references of the selected articles were reviewed for further relevant sources.
The position of the eyebrows is influenced by various factors, particularly the balance of surrounding muscles. The occipitofrontalis is the sole elevator of the eyebrows, while several depressor muscles—including procerus, corrugator supercilii (bilaterally), orbicularis oculi, and depressor supercilii—act against it.
With aging, changes in facial mimic muscles can contribute to eyebrow ptosis. As the periosteum recedes, the outer surfaces of facial bones shift, altering the attachment sites of facial ligaments and muscles. Consequently, the muscles become straighter, potentially losing their mechanical advantage, which affects facial mimic dynamics.17 This process leads to reduced muscle amplitude and strength. However, while muscle contraction amplitude and strength decrease with age, resting muscle tone appears to increase.
The frontalis muscle is laterally limited by the temporal fusion lines, meaning that in the lateral eyebrow region, the combined effect of gravity and depressor muscle activity lacks opposition.18 This results in a cranio-caudal pull on the lateral portion of the eyebrows, particularly when skin laxity is present in the upper third of the face. Meanwhile, the medial eyebrow position is also influenced by the vertical traction of the frontalis muscle. Additionally, Knize suggested that the supraorbital and supratrochlear nerves may provide additional support to the medial eyebrow, helping to resist ptosis.18 Yun et al.19 proposed muscle activity patterns change with age. By comparing absolute muscle activity values across different age groups, the authors found that frontalis and corrugator muscle recruitment was lower in older participants, consistent with age-related muscle weakening. In contrast, elderly individuals exhibited increased activity in the orbicularis oculi, suggesting an enhanced downward pull, which may contribute to eyebrow ptosis.19
In 2007, Rohrich and Pessa20 introduced the concept of facial fat compartmentalization, proposing that these compartments age differently and non-uniformly. Their study identified three superficial fat compartments in the forehead—a central segment and two lateral segments—all located between the skin and the superficial fascia of the occipitofrontalis muscle, separated by fibrous protective sheaths surrounding the supraorbital neurovascular structures.
Subsequent studies identified five deep forehead fat compartments: a central compartment, two lateral compartments (also separated by the supraorbital neurovascular bundles, positioned between the fascia covering the posterior surface of the frontalis muscle and the periosteum), and two additional compartments corresponding to the retro orbicularis oculi fat (ROOF), present bilaterally.21,22 ROOF is confined to the area between the inferior frontal septum and the upper portion of the orbit retaining ligament, with its lateral boundary at the temporal ligamentous attachments and medial boundary at the supraorbital neurovascular structures.21
The temporal fossae are bilateral depressions of the cranial vault, anatomically bounded by the temporal crest, lateral orbital rim, zygomatic arch, and posteriorly by the hairline. This region contains eleven anatomical layers, including three fat compartments: 1) the superficial temporal fat compartment, containing subcutaneous tissue; 2) the middle layer of temporal fat; and 3) the 3) deep layer of temporal fat, corresponding to the temporal portion of the buccal fat pad.21
Facial fat is thought to atrophy with age, especially in deep compartments. One possible explanation is the continuous compression of deep fat compartments between bone and overlying musculature.21 As a result, eyebrow positioning is particularly affected by volume depletion in the deep forehead fat compartments, temporal fat compartments, and ROOF.
The facial skeleton also plays a crucial role in supporting adjacent soft tissues, providing stability and definition. Beyond fat atrophy and displacement, the skull undergoes predictable remodeling with age, including changes in the eye orbit. The orbital opening increases over time, but bone resorption is not uniform along its margins. The inferolateral and superomedial regions experience greater resorption, with the inferolateral region changing earlier. Interestingly, in men, the inferomedial quadrant of the orbit recedes more significantly over time than in women.23 Meanwhile, the central portions of the upper and lower orbital margins remain relatively stable, exhibiting little to no bone resorption throughout life.23
In youthful individuals, the temporal region has a convex and continuous shape relative to the zygomatic arch, creating a smooth lateral orbital contour. However, with age, the temporal region becomes more concave, making the bony contour of the lateral orbital margin more pronounced. As a result, the tail of the eyebrow is pulled posteriorly and inferiorly, contributing to a heavier periorbital appearance and an aged facial look.
Aging-related changes in the extracellular matrix (ECM) are particularly significant in cutaneous aging, as the ECM is primarily composed of collagen types I and III, which play a crucial role in maintaining skin support and integrity.24
Decades ago, the ECM was considered an inert, metabolically inactive substance, merely a structural glue that bound tissues and supported cells.25 However, this perception has been radically revised. The ECM is now recognized as a highly dynamic system composed of proteins, glycosaminoglycans, and metabolically active cells that maintain a continuous equilibrium under physiological conditions.
During aging, the ECM undergoes gradual degradation, largely due to the increased activity of matrix metalloproteinases (MMPs), enzymes that regulate ECM remodeling. This process is observed in both intrinsic and extrinsic aging. MMP overactivity leads to the breakdown and fragmentation of collagen and elastin fibers, reducing their quantity and quality, which in turn causes a loss of skin elasticity and firmness, ultimately resulting in sagging and soft tissue ptosis.26,27
Emerging evidence suggests that dermal fibroblast aging is not solely a consequence of cellular senescence but is instead linked to their progressive loss of interaction with the ECM. This phenomenon occurs due to years of MMP-induced degradation, exacerbated by oxidative metabolism and accelerated by oxidative stress, primarily caused by ultraviolet (UV) radiation exposure.28
As fibroblasts lose their ability to bind to fragmented collagen, they collapse and undergo functional impairment. These collapsed fibroblasts produce low levels of collagen while simultaneously increasing the secretion of collagen-degrading enzymes. Consequently, once a critical threshold of collagen loss is reached, this imbalance perpetuates a self-sustaining cycle of progressive ECM deterioration and aging.29
A decrease in skin tension and elasticity, compounded by the effects of gravity, volumetric deflation of the upper third of the face, and muscular traction forces, contributes to the downward displacement of the eyebrows. Therefore, treatments that enhance the ECM microenvironment, preserving its physiological functions, as well as interventions that stimulate collagen and elastin production, may contribute to eyebrow repositioning.
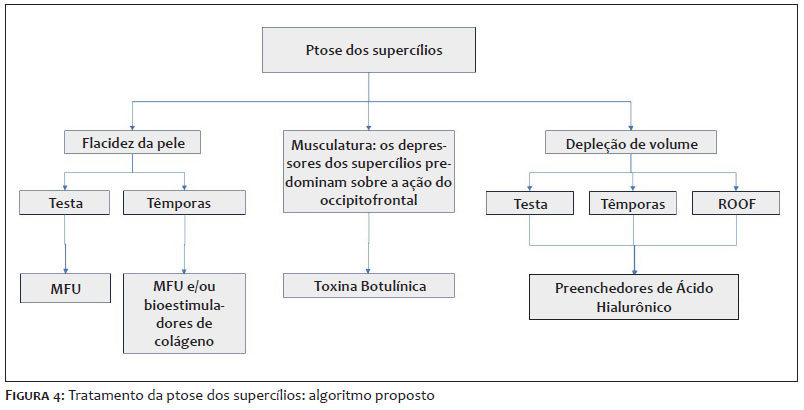
Based on the literature review presented in this article, we propose that the optimal strategy for minimally invasive eyebrow repositioning and shape enhancement consists of three distinct approaches: 1) treatments targeting skin quality and laxity improvement; 2) treatments optimizing muscular traction balance in the upper third of the face to achieve the desired eyebrow positioning; 3) treatments addressing tissue deflation through volumization.
Accordingly, we present a treatment algorithm for eyebrow lift, based on the authors' selection of key techniques for each approach.
In 2009, microfocused ultrasound (MFU) received US Food and Drug Administration (FDA) approval for brow lifting.30 The mechanism of action of MFU involves delivering acoustic energy to the target tissue, generating molecular vibration and friction. Part of this mechanical energy is converted into thermal energy, raising tissue temperature above 60ºC—a threshold necessary for collagen denaturation. This process creates small foci of thermal injury, stimulating neocollagenesis.31-34
Unlike other non-invasive tissue-tightening modalities, MFU is distinguished by its minimal downtime, precise energy delivery, and deeper penetration. The superficial musculoaponeurotic system (SMAS) is an attractive treatment target due to its viscoelastic properties35 and lifting capacity.
Regarding MFU for brow lifting, we believe the most logical approach is to apply this technology to the dermal layers of the forehead, temple, and periorbital regions. Since the average skin thickness in these areas does not exceed 2 mm,36 we recommend using transducers with depths up to this level. Deeper transducers may fail to adequately target the treatment area, potentially increasing discomfort and the risk of adverse effects.
A crucial consideration when treating the temple region is the potential risk of injuring the temporal branch of the facial nerve. This branch is exclusively motor and innervates the superior and anterior auricular muscles, the frontal belly of the occipitofrontalis, the orbicularis oculi, and the corrugator muscles. Injury to this nerve can result in muscle paralysis in the affected hemiface.21,37
When performing MFU treatment, several parameters must be customized based on the desired effect and individual patient characteristics. The number of coagulation points, spacing between points ("pitch"), depth, energy level, and point distribution within the treatment area are key factors influencing results.
Additionally, patient expectations should be carefully managed, as outcomes depend on individual factors such as the degree of cutaneous laxity, ECM quality, age, and lifestyle habits, all of which influence neocollagenesis capacity.
Injectable collagen biostimulators are substances that provide a lifting effect by increasing dermal thickness and stimulating the production of collagen and elastin fibers.38 Many experts, including the authors of this article, agree that poly-L-lactic acid (PLLA) and calcium hydroxyapatite (CaHA) can be used in various facial and body areas, as both appear to yield satisfactory collagen enhancement results.38–43 However, some questions remain regarding their comparative efficacy and whether one substance provides superior results in specific anatomical regions.38
For upper-face treatments, we recommend limiting the use of biostimulators to the temporal region, as injections into the forehead or periorbital area carry a higher risk of adverse effects, such as subcutaneous nodule formation, due to greater muscular activity in these areas.44
Because of the anatomical characteristics of the temporal region, cosmetic professionals should consider PLLA is a liquid product (reconstituted with sterile distilled water) and contains very small particles, which theoretically pose a lower risk of vascular occlusion, even in small vessels, compared to CaHA.
Regarding the injection plane, histological studies in animals comparing collagen production after intradermal versus subdermal injections have shown that intradermal application produces a greater amount of collagen.38,45 However, the intradermal plane also presents a higher risk of adverse effects, such as nodule formation and irregularities, compared to the subdermal plane.46,47 Therefore, we recommend the subdermal plane for the application of biostimulators (Figure 1).
Thread-lifting is a cosmetic procedure in which barbed threads are used to lift and rejuvenate facial tissues. Current research identifies two primary mechanisms by which thread-lifts achieve long-lasting effects. First, the threads anchor surrounding soft tissue, transferring tension to lift and reshape facial contours. Second, as the threads degrade, they stimulate the production of collagen and elastin fibers, providing semi-permanent tissue suspension.
Various brands offer thread-lifting products with different properties. Initially, polypropylene (PP) was widely used due to its nonabsorbable nature, taking over a year to degrade. More recently, absorbable materials such as polycaprolactone (PCL), polylactic acid (PLA), polyglycolic acid (PGA), and polydioxanone (PDO) have become more popular due to their biodegradable properties in facial rejuvenation procedures.48
Based on previous clinical experience, the ideal characteristics of barbed thread for facial thread-lifting include: 1) being absorbable and long-lasting; 2) having appropriately shaped barbs; 3) possessing suitable elastic modulus and mechanical strength; and 4) eliciting appropriate biological responses.
No direct comparative study in medical literature comprehensively evaluates all available thread brands based on these characteristics.48
While the long-term lifting effects of thread-lifting remain debatable, studies confirm that this technique is effective in promoting neocollagenesis.49–51 This is a significant advantage, particularly for eyebrow repositioning, since injectable biostimulators are not recommended for application in the frontal region.
Beyond material composition, threads vary in insertion method—whether via needles or cannulas. Cannulas have been shown to provide greater patient comfort, less pain, and fewer complications compared to needles, making them the preferred method. Cogged or beaded threads are typically inserted using wider cannulas, whereas needles, while easier to pass, can lead to increased bruising. Procedures such as Silhouette Soft™ require both entry and exit points, necessitating anesthesia at both sites.52
Threads also differ in shape and barb direction. Variants include simple filament threads, barbed (cogged) threads with spines along the same axis, threads with rotating spines along the thread axis, cogged threads with cones, and cogged threads with arrow-shaped spines. Additionally, threads with barbed sutures are often preferred for securing lifts. The direction of cogs or cones can be either unidirectional or bidirectional. Barbs may be replaced with cones in bidirectional threads, such as Silhouette Soft™.52 Cogged (barbed) threads are primarily used for brow lifting.
This article does not delve into specific eyebrow-lifting techniques using threads, as these methods vary significantly based on the type of thread chosen and the patient's anatomical characteristics. However, we emphasize that the key to success in all thread-lifting techniques is careful planning of lifting points and proper thread placement within the appropriate anatomical plane to optimize results and minimize complications.
For PDO thread insertion in eyebrow lift, the subdermal or subcutaneous plane is ideal,53 as these layers provide direct support to the skin, effectively lifting the eyebrows. Additionally, they minimize the risk of injury to underlying nerves and blood vessels, reducing potential complications. A thorough understanding of local anatomy is essential for precise thread placement.
Thus, the subdermal plane offers a safe, reliable site for thread insertion as it lies superficial to the facial musculature, avoiding deeper structures.21 By adhering to this anatomical plane, practitioners can achieve optimal lifting effects with a lower risk of adverse events.
We also advocate for the prior use of botulinum toxin in the upper third of the face. This approach serves as a complementary measure to thread-lifting procedures, as botulinum toxin selectively weakens specific facial muscles, reducing the likelihood of thread displacement due to muscle contraction. This combined strategy not only enhances the longevity and effectiveness of the thread lift but also improves aesthetic harmony and patient satisfaction with the outcome.
Botulinum toxin injection remodels the eyebrows through three distinct mechanisms: 1) when the lateral depressor muscles are injected, selective paralysis of the depressors results in unopposed elevation of the brow by the frontalis muscle; 2) when the medial depressor muscles are injected, toxin diffusion into the medial frontalis fibers causes partial paralysis of the medial frontalis and increased tone in the lateral frontalis fibers, leading to brow elevation; and 3) when the frontalis muscle is injected along with the brow depressors, the potential brow elevation by the frontalis muscle is attenuated, sometimes resulting in paradoxical brow depression.54
Since botulinum toxin acts at the neuromuscular junction, muscles with a higher concentration of neuromuscular junctions are more sensitive to the toxin. The region where neuromuscular junctions are distributed within a muscle is known as the zone of innervation.55 If neuromuscular junctions were evenly distributed, the zone of innervation would be diffuse. However, if junctions cluster in well-defined areas, the zones of innervation are considered focal.
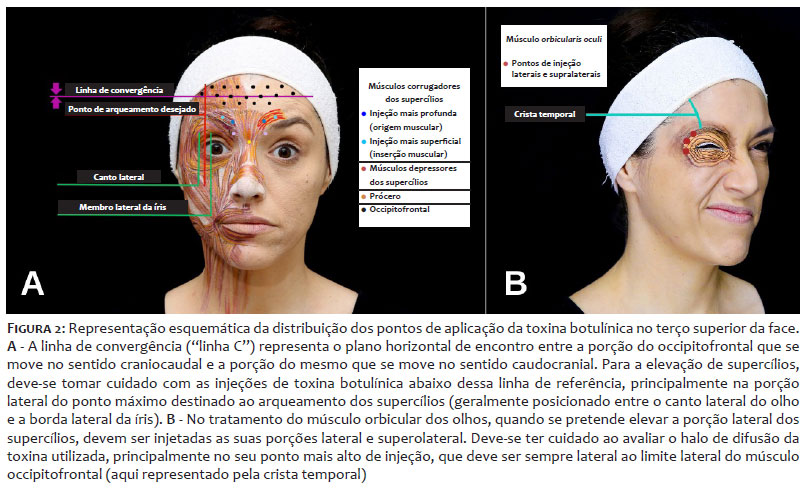
When zones of innervation are focal, precise botulinum toxin injection into these areas should maximize muscle relaxation. Therefore, our treatment recommendation for each muscle involved in brow lifting is as follows: the dose should be determined based on individual muscle strength assessment, while injection spacing should account for the expected diffusion halo, which depends on the toxin type, dilution, and planned dose (Figure 2).56,57
For the treatment of the procerus muscle, we recommend a single injection point in the muscular belly.
We suggest one to three injection points per side, with the number of injection sites determined by muscular palpation and inspection during contraction. The injection point near the muscular origin ("head" of the corrugator) should be deeper, considering its bony origin.²¹ Conversely, the closer the injection point is to the muscular insertion ("tail" of the corrugator), the more superficial it should be, as the muscle inserts into the skin.21
The fibers of the occipitofrontalis muscle in the region above the eyebrows also have cutaneous insertion. In this area, there is a crossing of fibers from the corrugator supercilii, occipitofrontalis, and orbicularis oculi muscles.21 Consequently, injectors should be cautious of toxin diffusion into the occipitofrontalis muscle, which could result in brow drooping at this point. On the other hand, some studies suggest that paralyzing the central portion of the frontalis muscle can lead to increased tone in the lateral frontalis fibers, which may be beneficial in elevating the lateral portion of the brows as part of a brow lift strategy.54
The depressor supercilii muscle is one of the glabellar muscles. It originates from the bony process of the maxilla and has one to two heads, which insert into the skin below the medial portion of the brow.58,59 It acts synergistically with the superomedial portion of the orbicularis oculi muscle and the corrugator supercilii muscle, contributing to inferomedial retraction of the brow.58
Additionally, the depressor supercilii plays a role in the formation of oblique expression lines, working alongside the procerus muscle and the medial portion of the orbicularis oculi muscle.58,60 For effective blocking of this muscle, botulinum toxin injection is performed approximately 10 to 15 mm above the medial canthal tendon, either to lift the medial portion of the brow or to reduce oblique glabellar wrinkles.61
As the sole muscle responsible for eyebrow elevation, the occipitofrontalis muscle must be treated with caution. To achieve this effect, we recommend targeting its central portion, which helps to reduce frontal wrinkles and may contribute to compensatory increased tone in the lateral portions of the muscle, thereby assisting in the elevation of the lateral portion of the eyebrows.
Cotofana et al.62 described a bidirectional movement of forehead skin during occipitofrontalis contraction: the lower forehead skin moves cranially, while the upper forehead skin moves caudally. These movements converge at a static and immobile line, referred to as the convergence line (C-line). To minimize the risk of eyebrow ptosis, botulinum toxin should be injected above the C-line while avoiding injections below it.62 Thus, laterally to the intended eyebrow elevation point (typically corresponding to the arching point), the frontalis muscle should only be treated above its convergence line,62 when identified.
In some patients, not treating the lower lateral portions of the frontalis muscle may lead to dissatisfaction due to the persistence or even exacerbation of wrinkles in these areas. In such cases, managing patient expectations and balancing wrinkle treatment with brow lifting is essential. If necessary, these areas can be treated using microdoses of botulinum toxin, a technique known as microbotox.63
Microbotox involves injecting multiple points of diluted botulinum toxin into small intradermal aliquots.64 This approach targets the superficial fibers of facial muscles, weakening their insertion into the skin's surface, which is responsible for fine lines and wrinkles. Since the three-dimensional nature of toxin diffusion, excessive intradermal dosing may lead to unintended muscle weakness or loss of facial mimetic activity in the treated areas. This effect could result in drooping of the lateral eyebrow portion if the microbotox technique is used too close to this anatomical region.63
The zone of innervation of the orbicularis oculi muscle appears to be diffuse, making it beneficial to use multiple injection points for optimized blocking.55 A motor point is defined as a small area on the skin near a specific muscle where the threshold for electrical excitability of that muscle is lower. In the study by Borodic,55 two consistent motor points of the orbicularis oculi muscle were identified across all observed cases. The first motor point was located in the superolateral portion at the level of the upper eyelid sulcus, while the second motor point was found in the inferomedial portion, near the anterior lacrimal crest.55
Additionally, injection point positioning should consider the specific function of each portion of the orbicularis oculi muscle. For brow lift, priority should be given to treating the lateral and upper portions of this muscle.21
Therefore, we recommend treating the orbicularis oculi muscle with multiple intramuscular injection points, focusing on its lateral and upper portions. Special care should be taken to prevent toxin diffusion into the lateral portion of the occipitofrontalis muscle, as this could result in brow tail ptosis.
To minimize this risk, the injector should first establish the point from which brow lift is desired—typically corresponding to the arching point—and avoid treating the frontalis muscle lateral to this point, or at least in the area below the previously mentioned C-line.
When injecting the superolateral portion of the orbicularis oculi muscle, we recommend using a highly precise toxin, with a dilution and dosage strategy that effectively reduces the chance of diffusion, ensuring optimal results while minimizing adverse effects.56,57
The next strategy for eyebrow repositioning involves addressing tissue deflation, if present. We recommend performing this step for at least 14 days after botulinum toxin treatment, once the desired effects of neuromodulation have been achieved.
Three anatomical regions should be evaluated for volumization: the temples, forehead, and lateral portion of the eyebrows. Treatment indications should be assessed individually for each patient based on their specific needs.
If volumization is required in more than one of these areas, we suggest prioritizing the temples first, followed by the forehead, and finally the tail of the eyebrows.
Casabona et al.65 retrospectively evaluated the effects of three hyaluronic acid temple-filling techniques, categorized by injection planes: subdermal, interfascial, and supraperiosteal. Each injection plane influenced facial aging changes to varying degrees, with the interfascial plane yielding superior results for eyebrow repositioning.65
The anatomy team of Instituto Boggio (São Paulo, Brazil) conducted a cadaveric study66 to replicate the interfascial injection technique.67 In this study, 89% of injections were performed in the incorrect layer, and in one case, the superficial temporal artery was transfixated by the cannula. The authors noted differences between performing procedures on freshly frozen cadaver specimens and live patients. However, given the anatomical complexity of the temporal region and the lack of established safety for reproducibility of the interfascial technique, our group considers this approach to carry a high risk of vascular complications and therefore avoids its use.
Our treatment algorithm recommends that temporal volumetric correction, when necessary, be performed through hyaluronic acid deposition in the supraperiosteal and subdermal planes, with the supraperiosteal plane reserved for cases with more significant deflation. Thus, we propose the following techniques.
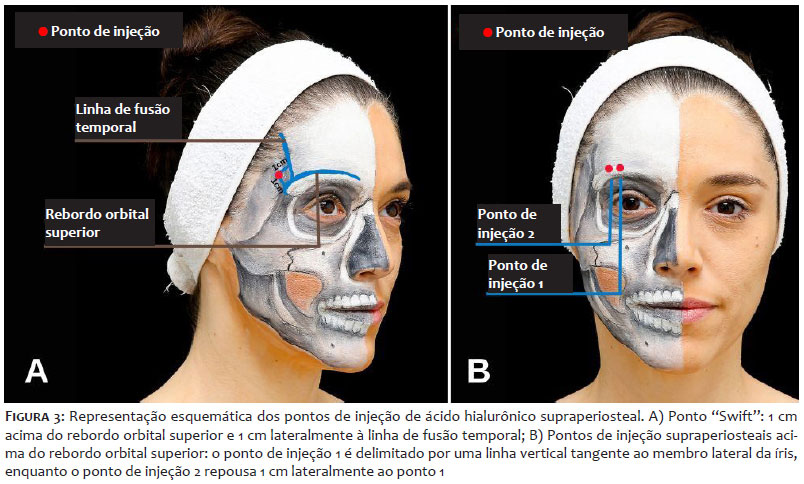
According to the technique described by Swift, a single injection point is made approximately 1 cm lateral to the temporal fusion line and 1 cm above the supraorbital margin, parallel to it. Before injecting, digital palpation is recommended to detect arterial pulsation and reduce the risk of significant vascular complications.67,68
After the needle reaches the temporal bone, aspiration is performed, followed by a slow bolus injection while maintaining continuous contact with the periosteum. For this technique, the use of high G' and high cohesiveness hyaluronic acid fillers is recommended to ensure circumferential product dispersion while still achieving effective elevation of the overlying tissues.69 The author of this technique recommends using an average of 0.25 to 0.75 mL per temple.
Cotofana et al.70 suggested injection into the temporal compartment generally requires more than 0.5 mL per side to produce a visible change in surface projection, which aligns with the clinical experience of the authors of this article (Figure 3A).
Many authors consider the supraperiosteal plane safe for injection due to the major vessels, such as the superficial temporal artery and the middle temporal vein, running through more superficial planes. However, branches of the deep temporal artery course between the temporal muscle and the periosteum, posing a potential vascular risk for deep injections in this region.71–73
The deep temporal artery, a branch of the maxillary artery, may anastomose with various arteries in the region, including the lacrimal, supraorbital, and middle meningeal arteries.21,74,75 Another important artery that may be present in the temporal region is the zygomatico-orbital artery, a bifurcation of the superficial temporal artery, sometimes emerging from its frontal or parietal branches. This sizable artery is typically described as running parallel and superior to the upper border of the zygomatic arch.21,76 However, in the study by Park et al.,76 the zygomatico-orbital artery followed a course along a line passing through the tragus and the supraorbital ridge, at approximately ±1 cm from this line.
Freytag et al.77 injected 20 hemifaces of fresh cadaveric specimens. The deep temporal injection was performed with a 25G needle, keeping constant contact with bone. Upon subsequent dissection, most of the product was found inside the temporal muscle, which the authors attributed to retrograde flow along the injection canal of the needle.
In our opinion, due to the extremely thin layers of the anatomical structures in the temple, positioning the needle perpendicular to the supraperiosteal plane may result in the bevel being partially within the intramuscular plane, even when the needle tip is in direct contact with the periosteum. This could explain misplaced injections.
In addition, the use of aspiration as a safeguard against vascular complications is highly controversial. The thicker consistency of certain fillers can lead to inconsistent aspiration results, requiring greater suction pressure and longer aspiration time to obtain a positive result. Therefore, a negative aspiration test (absence of blood in the needle hub) should not be relied upon alone, as the likelihood of a false-negative result is high.78
Therefore, we emphasize there is no consensus regarding the safety of supraperiosteal injections in the temples. Vascular complications in this region could result in shunting between the internal and external carotid systems, and injecting physicians must remain highly vigilant to the possibilities of anatomical variations.
For subdermal injection, this algorithm follows the technique described in the study by Faria et al.79 In this approach, hyaluronic acid is deposited in the subdermal plane through multiple linear retroinjections using a 22G cannula, with the entry point located in the inferolateral region of the orbit.
According to this technique, the various injection vectors form a larger angle relative to the path of the superficial temporal artery, which enhances vascular safety compared to other cannula entry points.79
For this filling plane, we recommend using high-cohesiveness hyaluronic acid products with low to medium G', depending on the thickness of the skin in the temporal region being treated (Figure 1).
To contribute to eyebrow lift, we recommend filling the deep fat compartments of the forehead whenever concavity is observed in this area. Typically, the injection site is in the vertical middle third of the forehead. In this region, the supraorbital and supratrochlear vessels become more superficial, increasing the risk of intravascular injection. To mitigate this risk, filler should be placed in the subgaleal plane, positioned immediately above the periosteum.68
For this technique, we recommend injecting hyaluronic acid using a 22G cannula, with the entry point positioned lateral to the injection area. The filler should be deposited as several small boluses of a high G' and high-cohesiveness product. After injection, manual massage should be performed to ensure better product distribution and accommodation.
In addition to skin distension and eyebrow traction, volumization beneath the occipitofrontalis muscle enhances its activity through a mechanism known as myomodulation.79,80
The goal of filling the lateral portion of eyebrow is to restore volume in the ROOF. This fat pad defines the shape of the eyebrow and the upper eyelid above the supratarsal crease.68,81 Loss of volume in this compartment contributes to deflation and descent of the eyebrow tail.82,83
For this procedure, a cannula entry point is created immediately lateral to the eyebrow. A 22G cannula is inserted parallel to the supraorbital rim, just above the bone, advancing to an appropriate clinically assessed distance. The filler should be placed laterally to the supraorbital neurovascular bundle to avoid injury and deep to the orbicularis oculi muscle. To enhance precision and minimize complications, the eyebrow is elevated with the nondominant hand, moving it away from the orbital rim.69
The filler should be deposited gradually, either in an anterograde or retrograde manner, ensuring placement above the orbital rim. The push-ahead technique, performed with anterograde injection, allows the material to lift the area in front of the cannula tip, reducing the risk of bruising.84 We suggest depositing the product in several small boluses.
After injection, manual shaping of the filler is performed to enhance symmetry, ensure homogeneity, and optimize anterior projection.
To further enhance the eyebrow lift, we recommend adding supraperiosteal injection points along the superior orbital rim at the precise locations where lifting is desired, while ensuring anatomical safety.
Typically, we suggest placing the first injection point along a vertical line aligned with the lateral limbus of the iris, and the second point approximately 1 cm lateral to it.
To prevent anterior eyebrow projection, these injections should be performed just above the supraciliary crest, where a palpable depression can be identified in the frontal bone (Figure 3B).
Eyebrow ptosis is not a universal occurrence in the aging process, but when present, it is typically more pronounced in the lateral third of the eyebrows. This condition results from a combination of anatomical and physiological changes affecting multiple tissue layers. Because of this complexity, botulinum toxin alone may not always be sufficient to achieve the desired eyebrow lift. A thorough and individualized assessment is essential to determine which aging-related changes predominate in each patient. By doing so, we can select the most appropriate tools and techniques for each case. Hence, we propose an algorithm for eyebrow repositioning using minimally invasive procedures (Figure 4).
Rebecca Ignacio Subirá Medina
ORCID: 0000-0001-6756-4263
Approval of the final version of the manuscript; study design and planning; manuscript drafting and writing; data acquisition, analysis, and interpretation; active participation in research supervision; intellectual contribution to the propaedeutic and/or therapeutic management of studied cases; critical review of the literature; critical review of the manuscript.
Gladstone Eustáquio de Lima Faria
ORCID: 0000-0002-0754-2019
Approval of the final version of the manuscript; study design and planning; manuscript drafting and writing; data acquisition, analysis, and interpretation; active participation in research supervision; intellectual contribution to the propaedeutic and/or therapeutic management of studied cases; critical review of the literature; critical review of the manuscript.
Ricardo Frota Boggio
ORCID: 0000-0002-5139-0243
Approval of the final version of the manuscript; study design and planning; manuscript drafting and writing; data acquisition, analysis, and interpretation; active participation in research supervision; intellectual contribution to the propaedeutic and/or therapeutic management of studied cases; critical review of the literature; critical review of the manuscript.
1. Westmore M. Facial cosmetics in conjunction with surgery. In: Aesthetic Plastic Surgical Society Meeting; 1974; Vancouver, British Columbia.
2. Wolfort FG, Gee J, Pan D, Morris D. Nuances of aesthetic blepharoplasty. Ann Plast Surg. 1997;38(3):257-262.
3. Gunter JP, Antrobus SD. Aesthetic analysis of the eyebrows. Plast Reconstr Surg. 1997;99(7):1808-1816.
4. Roth JM, Metzinger SE. Quantifying the arch position of the female eyebrow. Arch Facial Plast Surg. 2003;5(3):235-239.
5. Kunjur J, Sabesan T, Ilankovan V. Anthropometric analysis of eyebrows and eyelids: an inter-racial study. Br J Oral Maxillofac Surg. 2006;44(2):89-93.
6. Freund RM, Nolan WB. Correlation between brow lift outcomes and aesthetic ideals for eyebrow height and shape in females. Plast Reconstr Surg. 1996;97(7):1343-1348.
7. Flowers RS, Flowers SS. Precision planning in blepharoplasty. The importance of preoperative mapping. Clin Plast Surg. 1993;20(2):303-310.
8. Cook TA, Brownrigg PJ, Wang TD, Quatela VC. The versatile midforehead browlift. Arch Otolaryngol Head Neck Surg. 1989;115(2):163- 168.
9. Artz JS, Dinner MI, Foglietti MA. Planning the aesthetic foreheadplasty. Ann Plast Surg. 1990;25(1):1-6.
10. Tolleth H. Concepts for the plastic surgeon from art and sculpture. Clin Plast Surg. 1987;14(4):585-598.
11. Van den Bosch WA, Leenders I, Mulder P. Topographic anatomy of the eyelids, and the effects of sex and age. Br J Ophthalmol. 1999;83(3):347-352.
12. Maio M, Swift A, Signorini M, Fagien S. Facial assessment and injection guide for botulinum toxin and injectable hyaluronic acid fillers: focus on the upper face. Plast Reconstr Surg. 2017;140(2):265e-276e.
13. Feser DK, Gründl M, Eisenmann-Klein M, Prantl L. Attractiveness of eyebrow position and shape in females depends on the age of the beholder. Aesthetic Plast Surg. 2007;31(2):154-160.
14. Richer V, Berkowitz, Almeida AT. Eyebrow shape preference across age, gender, and self-reported ethnic Group. Dermatol Surg. 2023;49(2):171-176.
15. Matros E, Garcia JA, Yaremchuk MJ. Changes in eyebrow position and shape with aging. Plast Reconstr Surg. 2009;124(4):1296-1301.
16. Goldstein SM, Katowitz JA. The male eyebrow: a topographic anatomic analysis. Ophthalmic Plast Reconstr Surg. 2005;21(4):285-291.
17. Mendelson B, Wong CH. Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation. Aesthetic Plast Surg. 2012;36(4):753-760.
18. Knize DM. An anatomically based study of the mechanism of eyebrow ptosis. Plast Reconstr Surg. 1996;97(7):1321-1333.
19. Yun S, Son D, Yeo H, Kim S, Kim J, Han K, et al. Changes of eyebrow muscle activity with aging: functional analysis revealed by electromyography. Plast Reconstr Surg. 2014;133(4).
20. Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119(7):2219-2227.
21. Boggio R, Núcleo de Anatomia do Instituto Boggio. Anatomia Facial Aplicada. 1st . Di Livros Editora Ltda. 2022.
22. Cotofana S, Mian A, Sykes JM, Redka-Swoboda W, Ladinger A, Pavicic T, et al. An update on the anatomy of the forehead compartments. Plast Reconstr Surg. 2017;139(4):864e-872e.
23. Kahn DM, Shaw RB. Aging of the bony orbit: a three-dimensional computed tomographic study. Aesthet Surg J. 2008;28(3):258-264.
24. Lohwasser C, Neureiter D, Weigle B, Kirchner T, Schuppan D. The receptor for advanced glycation end products is highly expressed in the skin and upregulated by advanced glycation end products and tumor necrosis factor- alpha. J Invest Dermatol. 2006;126(2):291-299.
25. Uitto J, Olsen DR, Fazio MJ. Extracellular matrix of the skin: 50 years of progress. J Invest Dermatol. 1989;92(4):S61-S77.
26. Lee H, Hong Y, Kim M. Structural and functional changes and possible molecular mechanisms in aged skin. Int J Mol Sci. 2021;22(22):12489.
27. Reilly DM, Lozano J. Skin collagen through the lifestages: importance for skin health and beauty. Plast Aesthet Res. 2021;8:2.
28. Cole MA, Quan T, Voorhees JJ, Fisher GJ. Extracellular matrix regulation of fibroblast function: redefining our perspective on skin aging. J Cell Commun Signal. 2018;12(1):35-43.
29. Shanina NA, Patrushev AV, Zorman A. Histological and immune histochemical changes in facial skin treated with combined ablative and non-ablative laser therapy. J Cosmet Dermatol. 2021;20(11):3509-3516.
30. lkan A, Fabi S, Green J. Microfocused Ultrasound for Facial photo rejuvenation: a review. Facial Plast Surg. 2016;32(03):269-275.
31. Bozec L, Odlyha M. Thermal denaturation studies of collagen by microthermal analysis and atomic force microscopy. Biophys J. 2011;101(1):228-236.
32. Minkis K, Alam M. Ultrasound skin tightening. Dermatol Clin. 2014;32(1):71-77.
33. Alam M, White LE, Martin N, Witherspoon J, Yoo S, West DP. Ultrasound tightening of facial and neck skin: a rater-blinded prospective cohort study. J Am Acad Dermatol. 2010;62(2):262-269.
34. White WM, Makin IRS, Barthe PG, Slayton MH, Gliklich RE. Selective creation of thermal injury zones in the superficial musculoaponeurotic system using intense ultrasound therapy. Arch Facial Plast Surg. 2007;9(1):22-29.
35. Har-Shai Y, Bodner SR, Egozy-Golan D, Lindenbaum ES, Ben-Izhak O, Mitz V, et al. Viscoelastic properties of the superficial musculoaponeurotic system (SMAS): a microscopic and mechanical study. Aesthet Plast Surg. 1997;21(4):219-224.
36. Meng Y, Feng L, Shan J, Yuan Z, Jin L. Application of high-frequency ultrasound to assess facial skin thickness in association with gender, age, and BMI in healthy adults. BMC Med Imaging. 2022;22(1):113.
37. Silva MLA, Aboudib JH, Castro CC. Anatomia aplicada do ramo temporal do nervo facial: estudo do risco potencial de lesão durante a cirurgia do rejuvenescimento facial. Rev Bras Cir Plast. 2010;25(4):604-613.
38. Cunha MG, Engracia M, Souza LG, Machado Filho CD. Bioestimuladores e seus mecanismos de ação. Surg Cosmet Dermatol. 2020;12(2).
39. Corduff N, Chen JF, Chen YH, Choi HS, Goldie K, Lesthari, et al. Pan-asian consensus on calcium hydroxyapatite for skin biostimulation, contouring, and combination treatments. J Clin Aesthet Dermatol. 2021;14(8):E76-E85.
40. Haddad A, Menezes A, Guarnieri C, Coimbra D, Ribeiro E, Sarubi J, et al. Recommendations on the use of injectable poly-L-lactic acid for skin laxity in off-face areas. J Drugs Dermatol. 2019;18(9):929-935.
41. Casabona G, Pereira G. Microfocused ultrasound with visualization and calcium hydroxylapatite for improving skin laxity and cellulite appearance. Plast Reconstr Surg Glob Open. 2017;5(7):e1388.
42. Goldie K, Peeters W, Alghoul M, Butterwick K, Casabona G, Chao YYY, et al. Global consensus guidelines for the injection of diluted and hyperdiluted calcium hydroxylapatite for skin tightening. Dermatol Surg. 2018;44(1):S32-S41.
43. Vleggaar D, Fitzgerald R, Lorenc ZP. Consensus recommendations on the use of injectable poly-L-lactic acid for facial and nonfacial volumization. J Drugs Dermatol. 2014;(4 Suppl):s44-51.
44. Almeida AT, Figueredi V, Cunha ALG, Casabona G, Faria JRC, Alves EV, et al. Consensus recommendations for the use of hyperdiluted calcium hydroxyapatite (radiesse) as a face and body biostimulatory agent. Plast Reconstr Surg Glob Open. 2019;7(3):e2160.
45. Fenske NA, Lober CW. Structural and functional changes of normal aging skin. J Am Acad Dermatol. 1986;15(4):571-585.
46. Breithaupt A, Fitzgerald R. Collagen stimulators: poly-L-lactic acid and calcium hydroxyl apatite. Facial Plast Surg Clin North Am. 2015;23(4):459-469.
47. Hevia O. A retrospective review of calcium hydroxylapatite for correction of volume loss in the infraorbital region. Dermatol Surg. 2009;35(10):1487- 1494.
48. Cao L, Qiu H, Yu D, Shuo L, Wang H. Comparison of different thread products for facial rejuvenation: Materials and barb designs. J Cosmet Dermatol. 2023;22(7):1988-1994.
49. Tong LX, Rieder EA. Thread-lifts: a double-edged suture? A comprehensive review of the literature. Dermatol Surg. 2019;45(7):931-940.
50. Obourn CA, Williams EF. A decade of thread-lifting—what have we learned over the last 10 years? JAMA Facial Plast Surg. 2018;20(5):349-350.
51. Rachel JD, Lack EB, Larson B. Incidence of complications and early recurrence in 29 patients after facial rejuvenation with barbed suture lifting. Dermatol Surg. 2010;36(3):348-354.
52. Felipe I. Eyebrow thread lifting. In: Minimally invasive aesthetic procedures. Springer International Publishing; 2020:407-413.
53. Kim H, Jung J, Choi SW, Yun CW, Lee W. Eyebrow lifting using multidirectional absorbable thread. J Cosmet Dermatol. 2023;22(10):2780-2784.
54. Jabbour S, Awaida C, Kechichian E, Rayess Y, Abdelmassih Y, Noel W, et al. Botulinum toxin for eyebrow shaping: a systematic review. Dermatol Surg. 2017;43(3):S252-S261.
55. Borodic GE, Cozzolino D, Ferrante R, Wiegner AW, Young RR. Innervation zone of orbicularis oculi muscle and implications for botulinum A toxin therapy. Ophthalmic Plast Reconstr Surg. 1991;7(1):54-60.
56. Hsu TSJ, Dover JS, Arndt KA. Effect of volume and concentration on the diffusion of botulinum exotoxin A. Arch Dermatol. 2004;140(11).
57. Costa A, Pereira ESP, Pereira MO, Santos FBC, Favaro R, Stocco PL, et al. Comparative study of the diffusion of five botulinum toxins type-A in five dosages of use: Are there differences amongst the commercially-available products? Dermatol Online J. 2012;18(11).
58. Cook BE, Lucarelli MJ, Lemke BN. Depressor supercilii muscle. Ophthalmic Plast Reconstr Surg. 2001;17(6):404-411.
59. Daniel R, Landon B. Endoscopic forehead lift: anatomic basis. Aesthet Surg J. 1997;17(2):97-104.
60. Fagien S. Botox for the treatment of dynamic and hyperkinetic facial lines and furrows: adjunctive use in facial aesthetic surgery. Plast Reconstr Surg. 1999;103(2):701-713.
61. Domínguez-Duarte A. Aesthetic implications of depressor supercilii muscle block with botulinum toxin type A. J Cosmet Dermatol. 2022;21(4):1374-1378.
62. Cotofana S, Freytag DL, Frank K, Sattler S, Landau M, Pavicic, et al. The bidirectional movement of the frontalis muscle: introducing the line of convergence and it's cotential clinical relevance. Plast Reconstr Surg. 2020;145(5):1155-1162.
63. Diaspro A, Calvisi L, Manzoni V, Sito G. Microbotulinum: a quantitative evaluation of aesthetic skin improvement in 62 patients. Plast Reconstr Surg. 2020;146(5):987-994.
64. Wu WTL. Microbotox of the lower face and neck. Plast Reconstr Surg. 2015;136:92S-100S.
65. Casabona G, Frank K, Moellhoff N, Gavril DL, Swift A, Freytag DL, et al. Full-face effects of temporal volumizing and temporal lifting techniques. J Cosmet Dermatol. 2020;19(11):2830-2837.
66. Faria GEL, Nassif AD, Schwartzmann G, Zattar L, Boggio RF. Interfascial technique for volumizing the temple with no image guidance: is it safe? Eur J Plast Surg. 2023.
67. Cotofana S, Gaete A, Hernandez CA,Casabona G, Bay S, Pavicic T, et al. The six different injection techniques for the temple relevant for soft tissue filler augmentation procedures – clinical anatomy and danger zones. J Cosmet Dermatol. 2020;19(7):1570-1579.
68. Sykes JM, Cotofana S, Trevidic P, Solish N, Carruthers J, et al. Upper face: clinical anatomy and regional approaches with injectable fillers. Plast Reconstr Surg. 2015;136(5):204S-218S.
69. Almeida ART, Sampaio GAA, Queiroz NPL. Ácido hialuronico no rejuvenescimento do terço superior da face: revisão e atualização. Parte 2: regiões temporal e supraórbitária. Surg Cosmet Dermatol. 2017;9(2):113-121.
70. Cotofana S, Koban KC, Konstantin F, Green JB, Etzel L, Giunta R, et al. The surface-volume coefficient of the superficial and deep facial fat compartments: a cadaveric three-dimensional volumetric analysis. Plast Reconstr Surg. 2019;143(6):1605-1613.
71. Jung W, Youn KH, Won SY, Park JT, Hu KS, Kim HJ. Clinical implications of the middle temporal vein with regard to temporal fossa augmentation. Dermatol Surg. 2014;40(6):618-623.
72. Beleznay K, Carruthers JDA, Humphrey S, Jones D. Avoiding and treating blindness from fillers. Dermatol Surg. 2015;41(10):1097-1117.
73. Bae H, Choi Y, Lee K, Gil Y, Hu K, Kim H. The deep temporal arteries: anatomical study with application to augmentations procedures of the temple. Clin Anato. 2023;36(3):386-392.
74. Amans MR, Narvid J, Halbach VV. Intra-arterial chemotherapy for bilateral retinoblastoma via left ophthalmic artery and right anterior deep temporal artery. Case Reports. 2014;2014(sep19 3):bcr2014204549-bcr2014204549.
75. Quisling RG, Seeger JF. Orbital anastomoses of the anterior deep temporal artery. Neuroradiology. 1975;8(5):259-262.
76. Park HJ, Lee JH, Jung W. The superficial temporal artery and zygomatico-orbital artery: superficial arterial distribution of the anterior temple area. Biomed Res Int. 2022;2022:1-6.
77. Freytag DL, Frank K, Haidar R, Rudolph C, Muste J, Schenck TL, et al. Facial safe zones for soft tissue filler injections: a practical guide. J Drugs Dermatol. 2019;18(9):896-902.
78. Van Loghem J, Sattler S, Casabona G, Cotafona S, Fabi SG, Goldie K, et al. Consensus on the use of hyaluronic acid fillers from the cohesive polydensified matrix range: best practice in specific facial indications. Clin Cosmet Investig Dermatol. 2021;14:1175- 1199.
79. Faria GEL, Bastos AQ, Vilela CL, Zattar L, Boggio RF. Safety of the inferolateral orbital access for filling the temporal region with the fanning technique. J Cosmet Dermatol. 2022;21(11):5569-5575.
80. Maio M. Myomodulation with injectable fillers: an update. Aesthetic Plast Surg. 2020;44(4):1317-1319.
81. Goldberg RA. Eyelid anatomy revisited. Dynamic high-resolution magnetic resonance images of Whitnall's ligament and upper eyelid structures with the use of a surface coil. Arch Ophthalmol. 1992;110(11):1598.
82. Javidnia H, Sykes J. Endoscopic brow liftslifts: have they replaced coronal lifts? Facial Plast Surg Clin North Am. 2013;21(2):191-199.
83. Hetzler L, Sykes J. The brow and forehead in periocular rejuvenation. Facial Plast Surg Clin North Am. 2010;18(3):375-384.
84. Faria GEL, Bent AM, Santos DB, Tartare A, Boggio RF. Facial beautification with fillers and main differences between genders. Rev Bras Cir Plást. 2021;36(1).
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}