


Taciana Dal'Forno1; Maria Paula Del Nero2; Fernanda Nunes2; Cíntia Cunha3; Alessandra Haddad4; Adriana Vilarinho2; Alessandra Nogueira5; Rafael Tomaz5
Funding source: Galderma provided support for the formation of the board and the writing of the manuscript.
Conflict of interest: Dr. Dal'Forno, Dr. Nunes, and Dr. Cunha are consultants for Galderma. Dr. Del Nero is a speaker, advisor, and consultant for Galderma. Dr. Haddad is a speaker, consultant, advisor, and researcher for Galderma. Dr. Nogueira is the Medical Director at Galderma, and Dr. Tomaz is the Senior Clinical Manager at Galderma. *Dr. Vilarinho, a dermatologist, was invited to contribute to the article for educational purposes only, based on her technical knowledge. She has no conflict of interest with Galderma and does not hold any position with the company. None of the professionals mentioned here received any remuneration for their collaboration in this article.
Is this a clinical trial? No
Submission date: 06/12/2024
Final decision: 06/28/2024
How to cite this article: Dal'Forno T, Del Nero MP, Nunes F, Cunha C, Haddad A,Vilarinho A, Nogueira A, et al. Clinical recommendations for the combined use of poly-L-lactic acid (PLLA-SCA) and energy-based devices: expert opinion and literature review. Surg Cosmet Dermatol. 2025;17:e20250377.
The clinical use of combined technologies has been increasing to address the effects of skin aging on the face and other areas of the body. Poly-L-lactic acid is a biocompatible, semipermanent synthetic filler used for volume enhancement through neocollagenesis induction by fibroblast activation. Similarly, energy-based technologies, such as high-intensity focused ultrasound and microneedling radiofrequency devices, promote fat reduction and collagen contraction by heating the deep dermis. This article presents expert panel recommendations and a literature review on the topic.
Keywords: Polylactic Acid-Polyglycolic Acid Copolymer; Radiofrequency Therapy; Collagen Type I; Collagen Type III; Adipose Tissue.
Aging is a dynamic and complex process influenced by both extrinsic factors and intrinsic changes. As a result, the use of combined therapies has grown significantly to address biometric volume loss and skin alterations.1,2 In recent decades, rapid technological advancements have driven the widespread adoption of nonsurgical aesthetic procedures.3 Minimally invasive treatments that integrate multimodal approaches and target various manifestations of aging are not only safe but also often yield superior outcomes compared to single-modality treatments.1,4
Despite the increasing body of evidence and the clinical application of combined technologies to enhance aesthetic results,1,2,4-8 the specific interaction between poly-L-lactic acid (PLLA-SCA) and energy-based devices remains an area requiring further investigation. Strategies to restore lost soft tissue volume include the use of injectable fillers, such as poly-L-lactic acid (Sculptra®, Galderma, Uppsala, Sweden).9 Sculptra® is a biostimulatory injectable implant containing 150 mg of PLLA-SCA microparticles per vial. Suh microparticles are unique in both shape and have a median particle size of approximately 50 µm, maintained through a rigorous quality control process.10 PLLA-SCA has been extensively studied for aesthetic applications and functions as an absorbable, a-hydroxy-based synthetic filler that induces neocollagenesis by stimulating fibroblast activity. It is biocompatible and immunologically inert.2,9,11
Unlike traditional dermal fillers that primarily provide mechanical volume replacement, PLLA-SCA offers longer-lasting effects, as it stimulates fibroblast activity for up to two years post-injection.2,12,13 Initially approved for HIV-associated lipoatrophy, PLLA-SCA has also been widely used to correct facial wrinkles and volume loss. More recently, there has been growing interest in the nonfacial applications of PLLA-SCA, including volume augmentation, body contouring, skin laxity improvement, cellulite reduction, scar treatment, and striae distensae correction.14
Nonsurgical thermal approaches have been increasingly used to selectively target subcutaneous adipose tissue, including high-intensity focused ultrasound (HIFU) and radiofrequency (RF) energy devices.15 Both RF and HIFU are noninvasive, energy-based technologies designed for wrinkle reduction, collagen contraction, and skin tightening.5,16 While RF induces apoptosis in fat cells, HIFU causes coagulative necrosis and cell death.15
HIFU delivers ultrasound energy to selectively heat dermal and subdermal tissues above 60°C, creating a linear array of tightly focused thermal coagulation points. This process stimulates long-term collagen remodeling, leading to tissue tightening and lifting without damaging the epidermis.1,17,18 Treatment parameters can be adjusted by modifying energy levels and focal depth. Depending on the device, transducers emit frequencies between 2 and 10 MHz, with focal depths ranging from 1.5 to 13.0 mm, allowing targeted treatment of different facial and body tissues.15,19,20,21 Multiple studies have demonstrated the clinical efficacy and safety of HIFU for facial, neck, and body rejuvenation.17,18,22,23
Most HIFU devices include multiple transducer depths and focal sizes. Macrofocused ultrasound (MaFU) transducers, with larger thermal coagulation points, are typically used for fat reduction, while microfocused ultrasound (MIFU) transducers operate at different frequencies to tighten and lift lax skin.20
Similarly, RF technology employs low-frequency waves to generate an electromagnetic field within the skin, producing thermal heating of the dermis. This process promotes neocollagenesis, elastin formation, and angiogenesis during the healing response.24,25 Microneedle RF (MRF) enhances this effect by combining the mechanical penetration of microneedles with the thermal impact of RF. This combination allows heat to be delivered at variable depths, expanding the range of anatomical locations and tissue types that can be effectively treated.25,26 The precision of energy delivery optimizes dermal, subdermal, and adipose heating while minimizing epidermal damage, thereby facilitating contraction of dermis, subdermis, and surrounding connective tissue. Additionally, MRF can induce fat coagulation.27
MRF is a safe and effective treatment for various dermatologic concerns, including sagging skin, wrinkles, acne vulgaris, photoaging, enlarged pores, skin laxity, and scars.27-29 MRF is a versatile treatment option for various dermatologic concerns and is safe for patients of all skin types.25 In this expert opinion article, we present group recommendations for the combined use of PLLA-SCA and energy-based devices, drawing from the best available evidence and extensive long-term private practice experience.
In August 2023, a multidisciplinary panel of eight Brazilian medical experts convened to discuss the combined use of injectable PLLA-SCA and energy-based technologies. The group comprised physicians specializing in dermatology and plastic surgery, each with extensive clinical experience in these treatment modalities. The objective of this collaboration was to provide insights and establish best practices for optimizing treatment outcomes.
Prior to the meeting, expert group members were invited to participate in a pre-meeting questionnaire comprising 17 key components related to various aspects of treatment. The questionnaire covered the following topics:
1. Patient selection criteria for therapy combination
2. Clinical indications
3. Contraindications
4. Preoperative preparations
5. PLLA-SCA dilution methods
6. Techniques for PLLA-SCA injection
7. Number of PLLA-SCA sessions
8. Commercially available tested devices (MiFU, MaFU, MRF)
9. Device application techniques
10. Number of sessions for each device
11. Interval between sessions for each device
12. Sequencing in combined therapy
13. Order of technology application
14. Guidelines for intraoperative care
15. Protocols for postoperative care
16. Potential adverse effects
17. Post-treatment follow-up strategies
During the meeting, a neutral and trained medical facilitator (RT) led the discussions, ensuring an organized and structured exchange of insights. The session was recorded on video to accurately capture the discussions based on the questionnaire responses. The facilitator guided the conversation, summarized key points, and facilitated clarifications to ensure balanced participation from all experts. Discussions centered on comprehensive explanations of different treatment methods, the rationale behind treatment sequencing, safety considerations, and the synergistic effects of combined therapies for aesthetic rejuvenation.
Open debates and discussions were conducted to reach a consensus on potentially controversial topics. Participants leveraged available evidence, personal clinical experience, and key concerns to identify the most relevant principles. Such deliberations, supplemented by a review of current literature, served as the foundation for a practical guideline covering facial and body aesthetic rejuvenation treatments.
Observations and recommendations from the panel discussions were systematically assessed and compiled into a manuscript. This document underwent multiple iterative revisions, with all authors contributing to its refinement. Through this collaborative process, unanimous agreement was reached on the final version. The recommendations presented in this study reflect the collective expertise of the panel, drawing from extensive clinical experience and supported by previously published data on the integration of PLLA-SCA and energy-based technologies in aesthetic medicine for rejuvenation.
The expert panel had an average age of 48 years and an average of 25 years of medical practice. Their expertise was further strengthened by advanced training through residencies, master's programs, and doctoral degrees in specialized fields such as general surgery, plastic surgery, dermatology, and internal medicine. Following in-depth discussions, the panel formulated expert recommendations based on a combination of scientific evidence and the collective clinical experience of leading dermatologists, plastic surgeons, and researchers.
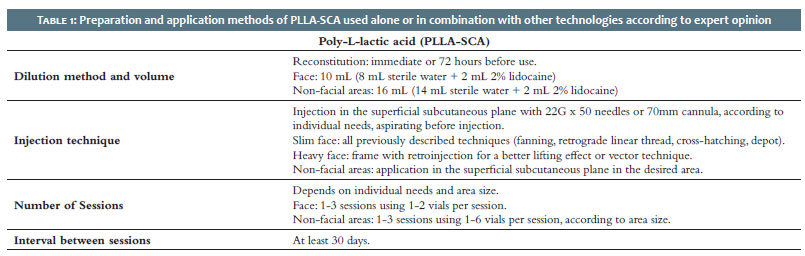
Since PLLA-SCA is the primary technology combined with selected energy-based devices, Table 1 presents detailed expert recommendations on dilution, injection techniques, number of sessions, and treatment intervals, both as a monotherapy and in combination therapy.
After reconstitution, PLLA-SCA can be used immediately or stored for up to 72 hours. Studies indicate immediate injection post-reconstitution is safe, associated with a low rate of adverse events (AEs), and offers practical advantages, such as reduced procedure time and minimized product loss for the injector.30,31
Regarding dilution volume, expert consensus established 10 mL for facial treatments and up to 16 mL for nonfacial applications, both with an additional 2 mL of 2% lidocaine. One expert referenced a prior study supporting the use of 12 mL for body injections.32 While various studies have explored the safety and efficacy of different dilution volumes for PLLA-SCA, a 2014 consensus by Vleggaar et al.33 recommended 9 mL for facial treatments and 16 mL for the décolletage, already incorporating anesthetics. Importantly, dilutions below 5 mL should be avoided, as highly concentrated formulations increase the risk of known AEs, including nodules and papules.34
The choice of dilution depends on the treatment goals. More concentrated formulations are preferred for volumization, as they require deep dermal or subdermal injections. In contrast, higher dilutions are typically used to improve skin quality or treat cellulite.3
PLLA-SCA injection sites yielding the best outcomes are dynamically stable and have sufficient dermal thickness to accommodate proper injection depth.33 Several injection techniques are reported for facial PLLA-SCA application, including fanning, retrograde linear threading, depot, or vector techniques, depending on the anatomic area and desired effect.11,33,35
Special caution is advised when treating patients with a heavier facial structure, thicker skin, and prominent superficial fat compartments. In such cases, the midface is typically avoided, while the upper and lower temples are prioritized, followed by the preauricular area, extending from the zygomatic arch to the mandible.35
For nonfacial areas, the choice of injection technique depends on the treatment site. A recent review identified linear threading and fanning as the most used techniques, performed with either a needle or cannula, on the neck, chest, buttocks, abdomen, and thighs.14 Treating large off-face areas may require up to 20 vials of PLLA-SCA to achieve significant aesthetic enhancement36; however, this approach can be costly and time-consuming. To optimize product usage for gluteal augmentation, Sarubi et al.37 developed a novel injection technique consisting of three distinct approaches, tailored to the primary aesthetic concern: improving skin quality, enhancing contour and lifting, or increasing projection and volume.
Overall, common adverse events, such as localized swelling, tenderness, redness, itching, and bruising, typically resolve within a week.30 Firmly massaging the treated areas immediately after injection promotes even product distribution and may help reduce the incidence of these side effects.4
Few studies have explored the combined use of PLLA-SCA with HIFU or MRF devices.2,4,6,38 As a result, the recommendations presented here are based on the authors' expertise, extrapolating from the available research. When implementing combination therapies, it is essential to consider individual patient needs, treatment goals, and the specific indications of each technology. Tables 2 and 3 outline the authors' recommendations for combining PLLA-SCA with MiFU and MaFU, respectively.
HIFU is used as a monotherapy in only 5–10% of patients, as it is more commonly combined with neuromodulators, fillers, and laser treatments to enhance outcomes.39 When paired with PLLA-SCA, HIFU simultaneously promotes volume restoration, neocollagenesis, and tissue contraction, offering multilevel cosmetic revitalization.2
The primary indications for this combined approach include facial lifting, rejuvenation, and the treatment of mild to moderate skin laxity, particularly in areas with concurrent fat compaction, such as the neck. Azuelos et al.40 demonstrated a single session of HIFU effectively improves cervical skin laxity, reduces submental fat (double chin), and diminishes neck wrinkles. Additionally, a study by Friedmann et al.4 confirmed the safety and enhanced efficacy of using MiFU followed by PLLA-SCA for multilayer facial rejuvenation, either in a single session or with a two-week interval to allow swelling to subside.
Coleman & Pozner38 proposed the use of HIFU followed by PLLA-SCA or HA as a treatment option for laxity and volume loss in the inner thigh and buttocks. However, given the larger treatment area, multiple sessions and vials are typically required. To minimize the risk of nodule formation, a higher PLLA-SCA dilution volume (12–16 mL) is recommended.32,38
The decision to administer facial biostimulatory fillers before or after energy-based therapies depends on the type and depth of treatment.7 Based on research involving other fillers, such as hyaluronic acid (HA) and calcium hydroxyapatite (CaHA), experts generally recommend applying HIFU first, followed by injectable fillers, as a standard approach.1,5,7,39 If both treatments are performed in the same session, MiFU should be applied first, followed by PLLA-SCA injection, to prevent water displacement from interfering with the targeted tissue depths and to avoid blood contamination of the ultrasound transducers.2
Conversely, in patients with a very low body mass index (BMI), skin laxity may result from volume depletion, in which case volume restoration should be prioritized before HIFU treatment.39 By restoring lost volume and structural support in the cheeks with fillers like PLLA-SCA, followed by MiFU treatment, fat pads are reinflated, and the zygomatic-buccal retaining ligaments are tightened and lifted. This approach often improves the appearance of nasolabial folds and other facial imperfections without the need for additional procedures.1
Based on the authors' experience, it is safe to apply line counts approximately 20% above the manufacturer's recommendation to achieve enhanced results; however, this approach may also increase patient discomfort. In a consensus guideline on MiFU applications, experts universally agreed that energy settings should be adjusted to the highest tolerable level, with titration as needed for patient comfort.41 Further research is warranted to assess the safety and efficacy of this approach.
Post-procedure care is essential to minimize the main side effects of both technologies, particularly when used in the same session. A common recommendation for facial treatment is a massage regimen in the treated area for 5 minutes, 5 times a day, for 5 days, which helps prevent nodule and papule formation. Additionally, maintaining a one-month interval between sessions can help avoid overcorrection.3,4,6,30,42 Similarly, for large non-facial areas, such as the gluteal region, it is recommended to massage the treated area in circular motions for 5 minutes, twice daily, for 5 to 7 days post-procedure to reduce bruising.37
Since both PLLA-SCA and energy-based devices stimulate collagen production through a wound-healing response, it is important to systematically evaluate patients for preexisting immune-mediated diseases. Chronic treatment with anti-inflammatory or immunosuppressive medications may impair the body's ability to recover from thermal injury.39
Table 4 presents the authors' recommendations for combining MRF with PLLA-SCA. RF therapy targets both the skin and soft tissue, inducing contraction by optimally heating dermal collagen while protecting the epidermis from injury.25 There are three primary types of RF energy—monopolar, bipolar, and multipolar—which differ in the number of emitting electrodes and depth of energy penetration. Monopolar RF is particularly effective for eyelid skin tightening, as the haptic contact lens protects the globe.1 RF energy can be delivered as bulk or fractional heating, with fractional modes allowing for interspersed untreated areas, promoting faster healing and reduced downtime.27 MRF further enhances skin tightening and adipose tissue remodeling by delivering energy through microneedles at a predetermined depth. This approach provides quick recovery, minimal downtime, and a low risk of pigmentation or skin infection.28
Antiviral therapy may be indicated before microneedling treatment, especially for patients with a history of prior viral infections, in accordance with current surgical guidelines. Additionally, standardized microneedling protocols should be developed, incorporating regulatory guidelines on prophylactic therapy and recommendations for medication suspension in patients on anticoagulants.43
Table 4 presents the authors' recommended protocols for combining PLLA-SCA with MRF. According to expert recommendations, the primary indications for this combination include the treatment of mild to severe skin laxity, attenuation of fine lines and ridges, and targeting fat compartments when using multilayer MRF devices.
Carruthers & Carruthers44 proposed the use of RF and HIFU devices to address skin laxity and submental fat accumulation after first rebuilding the supporting structures around the mouth and jawline using PLLA-SCA.44 Theoretically, MRF microneedles could enable the physical transdermal delivery of macromolecules with high molecular masses. However, concerns have been raised regarding whether the heat and energy delivered might accelerate filler degradation.45
A retrospective study of 28 patients treated with different fillers in combination with MRF found no unexpected filler loss or migration, even in highly expressive facial areas, after three treatment passes.46 Similarly, animal studies have demonstrated that monopolar RF applied over PLLA-SCA injections significantly enhances the inflammatory, foreign body, and fibrotic responses, which are essential for the clinical improvements observed. Additionally, RF treatment over filler-injected skin did not reduce the residence time of PLLA-SCA but instead enhanced collagen deposition within and around the treated areas.47,48
Beyond its applications in volume restoration, biostimulatory fillers such as PLLA-SCA have been used to mitigate acne scars, particularly where volume loss and tissue redistribution exacerbate scarring. A randomized controlled study reported that combining topical polylactic acid (PLA) injection before MRF significantly improved acne scars compared to MRF monotherapy. After three sessions at 4–6-week intervals, patient satisfaction scores and acne scar assessments were statistically superior with the combination approach.45
The interaction between RF and dermal fillers varies based on several factors, including RF type, energy level, filler type, depth of injection, and the interval between treatments.49 While some researchers suggest that fillers can be combined with RF devices on the same day without an increase in adverse effects or a decrease in efficacy,50 other studies have documented HA degradation when RF is applied immediately after filler injection49. An ex vivo study demonstrated that MRF applied over recently injected filler could damage HA due to its deeper dermal penetration.51 Conversely, a case study found that MRF performed one week after HA injection showed no evidence of HA degradation after 8 weeks, with no breakdown or extravasation into the epidermis.52 These findings suggest that treatment order and session intervals are crucial for optimal treatment outcomes and filler longevity.
While the recommendations presented in this study are based on several years of the authors' multicenter clinical experience and currently available literature, certain limitations must be acknowledged. The primary limitation is the level of evidence, as these guidelines rely on expert opinion rather than large-scale clinical trials. Further clinical and histological studies in large patient cohorts are needed to develop robust, evidence-based guidelines for combined aesthetic technologies in skin rejuvenation.
The combination of energy-based devices and fillers has become an integral part of clinical practice for patients seeking minimally invasive treatments to address multiple aspects of skin aging and achieve enhanced results. However, there remains a gap in the literature regarding the integration of PLLA-SCA with energy-based technologies, particularly concerning treatment sequencing, session intervals, device selection, injection methods, and application techniques. Based on the available evidence and the authors' clinical experience, this combination has been shown to be both safe and effective for improving skin quality in facial and non-facial areas. By targeting multiple skin layers and tissue types in a single session, this approach enhances treatment outcomes, reduces recovery time, and provides long-lasting aesthetic benefits for patients.
The authors thank Mauricio Dourado for the technical and editorial support.
Taciana Dal'Forno
ORCID: 0000-0003-0848-9042
Final approval of the manuscript; study conception and planning; manuscript drafting and writing; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the diagnostic and/or therapeutic management of studied cases; critical literature review; critical manuscript review.
Maria Paula Del Nero
ORCID: 0000-0002-5369-3504
Final approval of the manuscript; study conception and planning; manuscript drafting and writing; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the diagnostic and/or therapeutic management of studied cases; critical literature review; critical manuscript review.
Fernanda Nunes
ORCID: 0009-0002-2057-7344
Final approval of the manuscript; study conception and planning; manuscript drafting and writing; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the diagnostic and/or therapeutic management of studied cases; critical literature review; critical manuscript review.
Cíntia Cunha
ORCID: 0009-0009-4919-4882
Final approval of the manuscript; study conception and planning; manuscript drafting and writing; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the diagnostic and/or therapeutic management of studied cases; critical literature review; critical manuscript review.
Alessandra Haddad
ORCID: 0000-0002-5552-7251
Final approval of the manuscript; study conception and planning; manuscript drafting and writing; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the diagnostic and/or therapeutic management of studied cases; critical literature review; critical manuscript review.
Adriana Vilarinho
ORCID: 0009-0006-7381-6299
Final approval of the manuscript; study conception and planning; manuscript drafting and writing; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the diagnostic and/or therapeutic management of studied cases; critical literature review; critical manuscript review.
Alessandra Nogueira
ORCID: 0009-0005-9951-9471
Final approval of the manuscript; study conception and planning; manuscript drafting and writing; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the diagnostic and/or therapeutic management of studied cases; critical literature review; critical manuscript review.
Rafael Tomaz
ORCID: 0000-0001-8775-2173
Final approval of the manuscript; study conception and planning; manuscript drafting and writing; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the diagnostic and/or therapeutic management of studied cases; critical literature review; critical manuscript review.
1. Carruthers J, Burgess C, Day D, Fabi SG, Goldie K, Kerscher M, et al. Consensus recommendations for combined aesthetic interventions in the face using botulinum toxin, fillers, and energy-based devices. Dermatol Surg. 2016;42(5):586-97.
2. Hart DR, Fabi SG, White WM, Fitzgerald R, Goldman MP. Current concepts in the use of PLLA: clinical synergy noted with combined use of microfocused ultrasound and poly-l-lactic acid on the face, neck, and décolletage. Plast Reconstr Surg. 2015;136(5 Suppl):180S-187S.
3. Shridharani SM, Tisch GM, Ebersole TG, Moak TN, Edwartz C. Clinical experience of poly-L-lactic acid injections for body contouring treatment. J Cosmet Dermatol. 2021;20(6):1655-62.
4. Friedmann DP, Fabi SG, Goldman MP. Combination of intense pulsed light, sculptra, and ultherapy for treatment of the aging face. J Cosmet Dermatol. 2014;13(2):109-18.
5. Melo F, Carrijo A, Hong K, Trumbic B, Vercesi F, Waldorf HA, et al. Minimally invasive aesthetic treatment of the face and neck using combinations of a PCL-based collagen stimulator, PLLA/PLGA suspension sutures, and cross-linked hyaluronic acid. Clin Cosmet Investig Dermatol. 2020;13:333-44.
6. Peterson JD, Kilmer SL. Three-dimensional rejuvenation of the décolletage. Dermatol Surg. 2016;42 Suppl 2:S101-7.
7. Langelier N, Beleznay K, Woodward J. Rejuvenation of the upper face and periocular region: combining neuromodulator, facial filler, laser, light, and energy-based therapies for optimal results. Dermatol Surg. 2016;42 Suppl 2:S77-82.
8. Casabona G, Michalany N. Microfocused ultrasound with visualization and fillers for increased neocollagenesis: clinical and histological evaluation. Dermatol Surg. 2014;40 Suppl 12:S194-8.
9. Almukhtar RM, Wood ES, Loyal J, Hartman N, Fabi SG. A randomized, single-center, double-blinded, split-body clinical trial of poly- l -lactic acid for the treatment of cellulite of the buttocks and thighs. Dermatol Surg. 2023;49(4):378-82.
10. Morgan P, Bråsäter D, Öhrlund A. Product manufacturing process for poly-l-lactic acid (PLLA-SCA). Poster presented at the International Master Course on Aging Science (IMCAS) World Congress, 26 January to 28 January 2023, Paris, France.
11. Munia C, Parada M, Morais MHA. Changes in facial morphology using poly-l-lactic acid application according to vector technique: a case series. J Clin Aesthet Dermatol. 2022;15(7):38-42.
12. Trinh LN, Gupta A. Non-hyaluronic acid fillers for midface augmentation: a systematic review. Facial Plast Surg. 2021;37(4):536-42.
13. Zhang Y, Liang H, Luo Q, Chen J, Zhao N, Gao W, et al. In vivo inducing collagen regeneration of biodegradable polymer microspheres. Regen Biomater. 2021;8(5):rbab042.
14. Christen MO. Collagen stimulators in body applications: a review focused on poly-l- lactic acid (PLLA). Clin Cosmet Investig Dermatol. 2022;15:997-1019.
15. Coleman WP 3rd, Coleman W 4th, Weiss RA, Kenkel JM, Ad-El DD, Amir R. A multicenter controlled study to evaluate multiple treatments with nonthermal focused ultrasound for noninvasive fat reduction. Dermatol Surg. 2017;43(1):50-7.
16. Park JY, Lin F, Suwanchinda A, Wanitphakdeedecha R, Yu J, Lim TS, et al. Customized treatment using microfocused ultrasound with visualization for optimized patient outcomes: a review of skin-tightening energy technologies and a pan-asian adaptation of the expert panel's gold standard consensus. J Clin Aesthet Dermatol. 2021;14(5):E70-E79.
17. Kumar V, Jain A, Vadera S, Shome D, Kapoor R. Effectiveness of HIFU Therapy for nonsurgical facial and body contouring: a systematic review of prospective and experimental studies. Plast Reconstr Surg. 2023;151(3):533-44.
18. Khan U, Khalid N. A systematic review of the clinical efficacy of micro-focused ultrasound treatment for skin rejuvenation and tightening. Cureus. 2021;13(12):e20163.
19. Park JY, Youn S, Hong W, Lee KC, Kim I. Treatment protocol on using microfocused ultrasound with visualization for skin quality improvement: the korean experience. Plast Reconstr Surg Glob Open. 2023;11(5):e5029.
20. Casabona G, Kaye K. Facial skin tightening with microfocused ultrasound and dermal fillers: considerations for patient selection and outcomes. J Drugs Dermatol. 2019;18(11):1075-82.
21. Choi SY, No YA, Kim SY, Kim BJ, Kim MN. Tightening effects of high-intensity focused ultrasound on body skin and subdermal tissue: a pilot study. J Eur Acad Dermatol Venereol. 2016;30(9):1599-602.
22. Ling J, Zhao H. A systematic review and meta-analysis of the clinical efficacy and patients' satisfaction of Micro-focused Ultrasound (MFU) treatment for facial rejuvenation and tightening. Aesthetic Plast Surg. 2023;47(5):1806-23.
23. Ayatollahi A, Gholami J, Saberi M, Hosseini H, Firooz A. Systematic review and meta- analysis of safety and efficacy of high-intensity focused ultrasound (HIFU) for face and neck rejuvenation. Lasers Med Sci. 2020;35(5):1007-24.
24. Chao JR, Porter JP, Hessler J. Cosmetic treatments with energy-based devices in skin of color. Facial Plast Surg. 2023;39(5):496-500.
25. Hendricks AJ, Farhang SZ. Dermatologic facial applications of Morpheus8 fractional radiofrequency microneedling. J Cosmet Dermatol. 2022;21 Suppl 1:S11-S19.
26. Feng J, Zhang L, Qi J, Huang L. Histological damage characteristics and quantitive analysis of porcine skin with non-insulated microneedle radiofrequency. Skin Res Technol. 2023;29(6):e13396.
27. Magro I, Kochhar A, Arnaoutakis D, Karimi K. Transcutaneous radiofrequency microneedling in the facial plastic surgeon's practice: a review. Facial Plast Surg Aesthet Med. 2022;24(S1): S3-S10.
28. Wu X, Zhang Z, Zhu J, Lu S, Chen C, Wu X, et al. Can microneedle fractional radiofrequency system treatment impair the skin barrier function in chinese patients? A prospective clinical trial. Dermatol Ther (Heidelb). 2022;12(10):2371-82.
29. Suh DH, Cho M, Kim HS, Lee SJ, Song KY, Kim HS. Clinical and histological evaluation of microneedle fractional radiofrequency treatment on facial fine lines and skin laxity in Koreans. J Cosmet Dermatol. 2023;22(5):1507-12.
30. Bravo BSF, Carvalho RM. Safety in immediate reconstitution of poly-l-lactic acid for facial biostimulation treatment. J Cosmet Dermatol. 2021;20(5):1435-8.
31. Baumann K, Alm J, Norberg M, Ejehorn M. Immediate use after reconstitution of a biostimulatory poly-l-lactic acid injectable implant. J Drugs Dermatol. 2020;19(12):1199-203.
32. 32. Mazzuco R, Dal'Forno T, Hexsel D. Poly-l-lactic acid for nonfacial skin laxity. Dermatol Surg. 2020;46 Suppl 1:S86-S88.
33. Vleggaar D, Fitzgerald R, Lorenc ZP, Andrews JT, Butterwick K, Comstock J, et al. Consensus recommendations on the use of injectable poly-L-lactic acid for facial and nonfacial volumization. J Drugs Dermatol. 2014;13(4 Suppl):s44-51.
34. Palm M, Weinkle S, Cho Y, LaTowsky B, Prather H. A randomized study on plla using higher dilution volume and immediate use following reconstitution. J Drugs Dermatol. 2021;20(7):760-6.
35. Avelar LET, Haddad A. Facial assessment for poly-l-lactic acid application— one product, different outcomes. J Dermat Cosmetol. 2023;7(3):75-7.
36. Durairaj KK, Devgan L, Lee Bs A, Khachatourian Bs N, Nguyen Bs V, Issa Bs T, et al. Poly-L-Lactic acid for gluteal augmentation found to be safe and effective in retrospective clinical review of 60 patients. Dermatol Surg. 2020;46 Suppl 1:S46-S53.
37. Sarubi J, Guarnieri C, Del Nero MP, Kamamoto C, Honda M, Saito F, et al. Targeted and individualized gluteal poly-l- lactic acid injection for optimal aesthetic results in the gluteal region. J Clin Aesthet Dermatol. 2023;16(6):30-6.
38. Coleman KM, Pozner J. Combination therapy for rejuvenation of the outer thigh and buttock: a review and our experience. Dermatol Surg. 2016;42 Suppl 2:S124-30.
39. Fabi SG, Joseph J, Sevi J, Green JB, Peterson JD. Optimizing patient outcomes by customizing treatment with microfocused ultrasound with visualization: gold standard consensus guidelines from an expert panel. J Drugs Dermatol. 2019;18(5):426-32.
40. Azuelos A, SidAhmed-Mezi M, La Padula S, Aboud C, Meningaud JP, Hersant B. High- intensity focused ultrasound: a satisfactory noninvasive procedure for neck rejuvenation. Aesthet Surg J. 2019;39(8): NP343-NP351.
41. Fabi SG, Burgess C, Carruthers A, Carruthers J, Day D, Goldie K, et al. Consensus recommendations for combined aesthetic interventions using botulinum toxin, fillers, and microfocused ultrasound in the neck, décolletage, hands, and other areas of the body. Dermatol Surg. 2016;42(10):1199-208.
42. Wu DC, Goldman MP. The efficacy of massage in reducing nodule formation after poly-l-lactic acid administration for facial volume loss: a randomized, evaluator- blinded clinical trial. Dermatol Surg. 2016;42(11):1266-1272. Erratum in: Dermatol Surg. 2017;43(7):1001.
43. Chu S, Foulad DP, Atanaskova MN. Safety profile for microneedling: a systematic review. Dermatol Surg. 2021;47(9):1249-14.
44. Carruthers J, Carruthers A. A multimodal approach to rejuvenation of the lower face. Dermatol Surg. 2016;42 Suppl 2:S89-93.
45. An MK, Hong EH, Suh SB, Park EJ, Kim KH. Combination therapy of microneedle fractional radiofrequency and topical poly-lactic acid for acne scars: a randomized controlled split-face study. Dermatol Surg. 2020;46(6):796-802.
46. Wang JV, Valiga A, Albornoz CA, Geronemus RG. Safety of combining cosmetic injectables with radiofrequency microneedling: a 4.5-year review. J Cosmet Dermatol. 2021;20(4):1084-5.
47. Shumaker PR, England LJ, Dover JS, Ross EV, Harford R, Derienzo D, et al. Effect of monopolar radiofrequency treatment over soft-tissue fillers in an animal model: part 2. Lasers Surg Med. 2006;38(3):211-7.
48. England LJ, Tan MH, Shumaker PR, Egbert BM, Pittelko K, Orentreich D, et al. Effects of monopolar radiofrequency treatment over soft-tissue fillers in an animal model. Lasers Surg Med. 2005;37(5):356-65.
49. Jurairattanaporn N, Amornpetkul W, Rutnin S, Vachiramon V. The effect of combined hyaluronic acid filler injection and radiofrequency treatment: a clinic histological analysis. J Cosmet Dermatol. 2023;22(3):798-803.
50. Humphrey S, Beleznay K, Fitzgerald R. Combination therapy in midfacial rejuvenation. Dermatol Surg. 2016;42 Suppl 2:S83-8.
51. Hsu SH, Chung HJ, Weiss RA. Histologic effects of fractional laser and radiofrequency devices on hyaluronic acid filler. Dermatol Surg. 2019;45(4):552-6.
52. Shao EX, Lim D. Stability of hyaluronic acid fillers after insulated microneedle radiofrequency treatment. Dermatol Surg. 2019;45(9):1213-6.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}