


Isabelle Ary Duque; Francisco Jefferson Araújo Elias; Matheus Morais Lima
Funding source: None.
Conflict of interest: None.
Submission date: 02/25/2024
Final decision: 09/12/2024
How to cite this article: Duque IA, Elias FJA, Lima MM. Transverse facial artery occlusion following hyaluronic acid and calcium hydroxyapatite filler injection: a case report. Surg Cosmet Dermatol. 2025;17:e20250352.
This case report describes a complication following the use of a filler composed of hyaluronic acid and calcium hydroxyapatite mixed in the same syringe, resulting in vascular occlusion of the right transverse facial artery. The patient developed hypopigmented macules, followed by a reticulated pattern and pustules. Treatment included prednisone, enoxaparin, and hyaluronidase. Due to worsening symptoms, including arterial obstruction confirmed by ultrasound, ultrasound-guided hyaluronidase injection and hyperbaric oxygen therapy were administered. The patient showed a favorable recovery, with regression of vascular complications. This case underscores the importance of early identification and intervention to minimize complications associated with vascular occlusion in aesthetic procedures.
Keywords: Dermal Fillers; Hyaluronoglucosaminidase; Arterial Occlusive Diseases.
A 43-year-old woman (phototype III) underwent zygomatic region filler injection for volumetric restoration. The product used was a combination of hyaluronic acid and calcium hydroxyapatite (Harmonyca), applied with a 22G × 70 mm cannula. Injections were administered at three points, each 0.1 mL bolus, targeting the zygomatic arch, zygomatic prominence, and malar region.
Immediately after the procedure, the patient developed hypopigmentation on the right hemiface (Figures 1 and 2). At the time, she did not report any symptoms. Hyaluronidase was promptly administered, prepared as 2,000 IU diluted in 5 mL of diluent, and the patient was referred for ultrasound assessment to investigate possible vascular obstruction, which was not confirmed.
Twelve hours later, photographic records sent by the patient revealed the development of livedo reticularis (Figure 3). At that point, treatment was initiated, including prednisone (0.5 mg/kg/day), aspirin (200 mg/day), enoxaparin (1 mg/kg every 12 hours), and an empirical antibiotic regimen with amoxicillin-clavulanate. Additionally, a new hyaluronidase application was performed over the entire livedo-affected area (Figure 4).
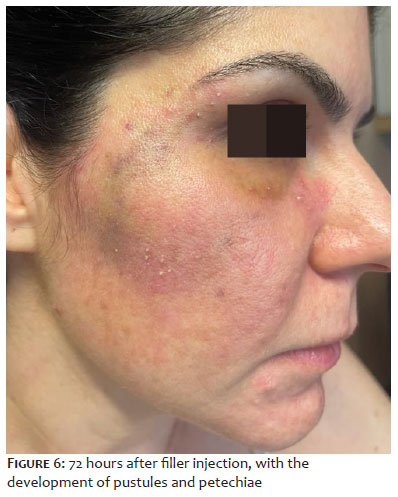
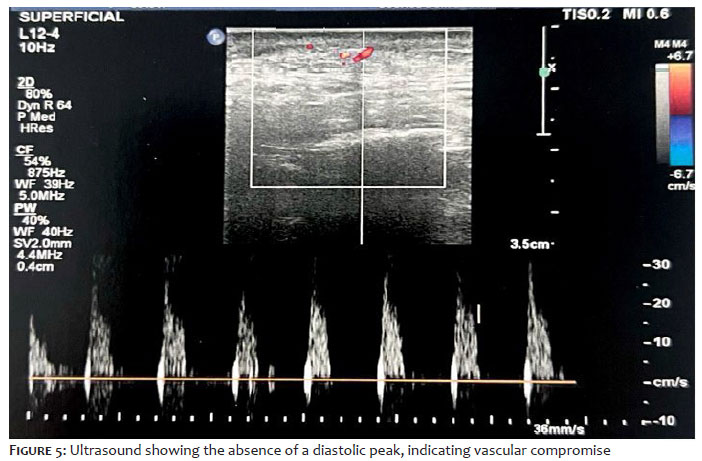
Seventy-two hours after the procedure, signs of vascular obstruction progressed, with the formation of pustules and petechiae (Figure 6). A repeat ultrasound revealed extrinsic subocclusion of the transverse facial artery at the middle third (Figure 5). Ultrasound-guided hyaluronidase injection was then performed.
Adjuvant therapy with hyperbaric oxygen therapy was initiated. After 10 days, the patient achieved complete resolution of clinical signs (Figure 7).
This case underscores the importance of early identification and intervention to minimize complications related to vascular occlusion in aesthetic procedures.
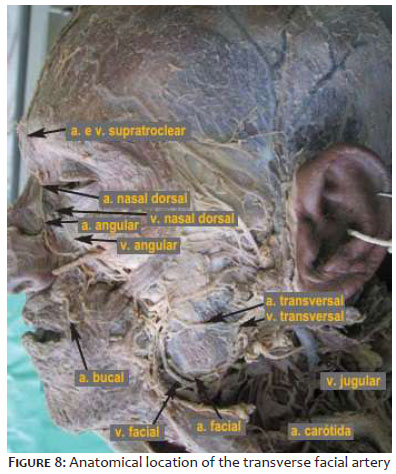
The transverse facial artery plays a crucial role in lateral facial irrigation and is one of the primary arteries affected in cases of vascular occlusion. It is located approximately two centimeters above the zygomatic arch and runs parallel to it, although anatomical variations may occur. This artery typically originates from the superficial temporal artery, but in some cases, it may arise directly from the external carotid artery (Figure 8). It supplies blood to the parotid gland, facial nerve, and zygomatic region.
When considering vascular events, a survey of 370 dermatologists found that the incidence of vascular occlusion was approximately 1 in 6,410 injections with a needle and 1 in 40,882 injections with a cannula. Another study showed that the relative risk of vascular occlusion was twice as high among physicians with less than five years of practice compared to more experienced professionals, highlighting clinical experience as a key factor in reducing complications.1
A case series analyzing 46 articles with 164 patients reported 436 complications related to calcium hydroxyapatite and hyaluronic acid fillers. Among them, 31 cases involved the malar region and were classified as mild or transient, with the most common complications being redness and edema at the injection site.7 The zygomatic area is generally considered a moderate- to low-risk region.2
Early identification of vascular occlusion—particularly in its initial stage (pallor)—and immediate administration of hyaluronidase are essential to minimize the risk of tissue necrosis. Key criteria for assessing arterial occlusion include capillary refill time, pain, and skin color.2 In this case, the patient initially presented with pallor, followed by livedo reticularis, corresponding to stage two of vascular occlusion. This was promptly identified and treated with hyaluronidase. However, despite early intervention, the condition worsened, reinforcing the importance of frequent reassessments to monitor treatment effectiveness in vascular occlusion cases. Dermatological ultrasound is a valuable tool for detecting, describing, and assessing complications of exogenous materials.9 However, its effectiveness relies on the sonographer's expertise. In this case, the initial ultrasound did not reveal an obstruction.
In cases of vascular events induced by facial fillers, the duration of ischemia directly correlates with the extent of tissue damage. Prompt recognition and understanding of occlusion stages are crucial for effective treatment and clinical management. Regular patient reassessment is essential to monitor treatment response and ensure timely adjustments to therapeutic strategies.
Isabelle Ary Duque
ORCID: 0009-0002-6381-1524
Final approval of the manuscript; study conception and planning; intellectual contribution to the diagnostic and/or therapeutic management of studied cases; critical literature review.
Francisco Jefferson Araújo Elias
ORCID: 0009-0008-9515-3750
Manuscript drafting and writing; critical literature review; critical manuscript review.
Matheus Morais Lima
ORCID: 0000-0002-3722-963X
Manuscript drafting and writing; critical literature review; critical manuscript review.
1. Alam M, Kakar R, Dover JS, Harikumar V, Kang BY, Wan HT, et al. Rates of vascular occlusion associated with using needles vs cannulas for filler injection. JAMA Dermatol. 2021;157(2):174–180.
2. Murray G, Convery C, Walker L, Davies E. Guideline for the management of hyaluronic acid filler-induced vascular occlusion. J Clin Aesthet Dermatol. 2021;14(5):E61-E69.
3. Urdiales-Gálvez F, Delgado NE, Figueiredo V, Lajo-Plaza JV, Mira M, Moreno A, et al. Treatment of soft tissue filler complications: expert consensus recommendations. Aesthetic Plast Surg. 2018;42(2):498-510.
4. Garvier MH, Bass LM, Fitzgerald R, Golberg DJ, Gottfried L. Differentiating nonpermanent injectable fillers: prevention and treatment of filler complications. Aesth Surg J. 2018;38(Suppl 1):S29-S40.
5. Tamura BM. Facial anatomy and the application of fillers and botulinum toxin – part 2. Surg Cosmet Dermatol.2010;2(4):291-303.
6. Rodriguez-Valera A, Nieto-Lopez F. Hyperbaric oxygenation therapy improve recovery in early or late vascular occlusion generates by tissue fillers. J Cosmet Dermatol. 2023;22(7):1969-1972.
7. Oranges CM, Brucato D, Schaefer DJ, Kalbermatten DF, Harder Y. Complications of nonpermanent facial fillers: a systematic review. Plast Reconstr Surg Glob Open. 2021;9(10):e3851.
8. Daskalopoulou D, Matsas A, Chrysikos D, Troupis T. The superficial temporal artery: anatomy and clinical significance in the era of facial surgery and aesthetic medicine. Acta Med Acad. 2022;51(3):232-242.
9. Díaz CPG. High resolution ultrasound of soft tissues for characterization of fillers and its complications. Rev Colomb Radiol. 2019;30:5064-5068.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}