


Ana Gabriella Bandeira Freire Andrade; Rossana Cantanhe de Farias de Vasconcelos; João Guilherme Finizola de Vasconcelos; Ana Maria Bertelli Antonio Gallotti; Caroline Costa de Mendonça
Funding: None
Conflict of Interest: None
Submission Date: 02/16/2024
Final Decision: 03/02/2024
How to cite this article: Andrade AGBF, Vasconcelos RCF, Vasconcelos JGF, Gallotti AMBA, Mendonça CC. Histological comparison of the action of CO2 laser and plasma in abdominal skin. Surg Cosmet Dermatol. 2024;16:e20240348.
Histological data on microscopic treatment zones are essential for evaluating procedure safety and effectiveness. To date, no studies have histologically compared low-temperature plasma with other techniques. In this study, two square areas on the patient's abdomen, referred to as area A and area B, were with low-temperature plasma and fractional CO2 laser, respectively. A biopsy was taken immediately after treatment. When applied to thinner skin regions, plasma technology appears to result in fewer complications, a faster recovery, and fewer side effects during the application period. However, further studies are needed to confirm these findings.
Keywords: Laser Therapy; Histology Comparative; Plasma Skin Regeneration; Gas Lasers.
CO2 laser (CO2L) is one of the most widely used treatments in dermatology. However, due to its associated complications, nonablative fractional lasers (NAFL) were introduced.1,2 Following NAFL, ablative fractional lasers (AFL) were developed, emitting narrow, high-energy beams that destroy columns of tissue. Around these ablated columns, an adjacent ring of thermal damage forms, known as microscopic treatment zones (MTZs).3 Within the MTZs, columns of uninjured tissue contribute to the clinical response to treatment.
The skin retraction and neocollagenesis observed with AFL result from two primary effects—ablation and injury.3,4 AFLs allow greater control over treatment depth, more selective thermal damage, and consequently, a significant reduction in side effects.1
Over the past decade, medicinal plasma has emerged as a powerful tool for biomedical applications, particularly in therapies for delicate tissues.5 Low-temperature plasma (LTP), which operates below 40°C, has been evaluated for treating conditions requiring tissue retraction, such as blepharochalasis syndrome, tissue laxity, and scarring. Additionally, LTP has demonstrated effectiveness in treating cutaneous neoplasms, viral infections, and biofilm-related infections.5
Histological data on MTZ dimensions—depth, diameter of ablation, coagulation, and necrosis—are crucial for assessing procedure safety and effectiveness, as well as for optimizing treatment combinations based on individual patient needs.6 However, no studies have yet histologically compared LTP with other techniques. According to Baroni, compared to conventional radiofrequency and ablative treatments, LTP promotes better healing and superior aesthetic outcomes.
A woman scheduled for abdominoplasty in 3 months consented to participate in this study. Two squared areas of approximately 4 cm2 were selected on her abdomen, designated as Area A and Area B, where plasma application and fractional CO2L were performed, respectively.
In Area A, LTP was applied using the Surgical Derm device from the SOLON® platform (LMG – Laser Medical Group Ltda., Guaxupé, MG, Brazil). In Area B, Dual Deep® fractional CO2L (Lutronics, Gyeonggi-do, South Korea) was applied with the following parameters: wavelength 10,600 nm, pulse energy 50 mJ, and static mode.
Immediately after the procedures, a 4 mm punch biopsy was performed. The two tissue samples were fixed in a 10% formaldehyde solution before processing for light microscopy, which included dehydration, paraffin embedding, and sectioning. Hematoxylin and eosin stains were used to visualize and analyze the depth and diameter of the coagulation channel. Histological sections were examined under 100× magnification with a polarized light source, using an Olympus BX41 trinocular microscope coupled to an Olympus C-35DA-2 camera.
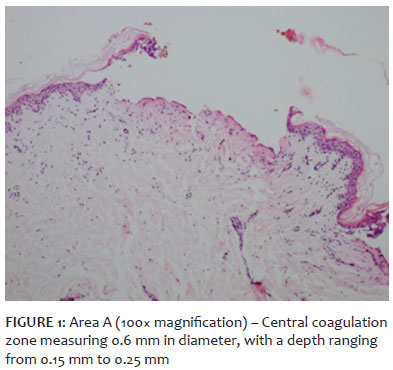
The histopathological analysis of Area A (Figure 1), subjected to LTP, revealed a central coagulation zone measuring 0.6 mm in diameter, with a depth ranging from 0.15 mm to 0.25 mm, excluding the epidermis. The papillary dermis surrounding this area exhibited edema and a reduction in elastic tissue, confirmed by Verhoeff stain. Masson's trichrome staining did not reveal any significant findings.
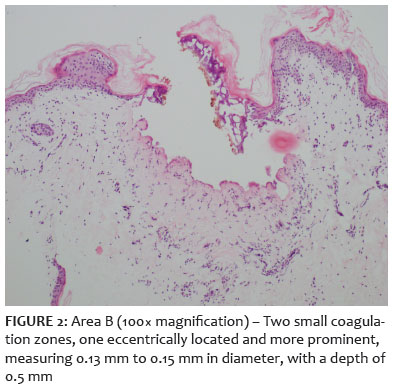
In Area B (Figure 2), two small coagulation zones of similar dimensions were observed. One, located eccentrically, was more prominent, measuring 0.13 mm to 0.15 mm in diameter, with a depth of 0.5 mm, excluding the epidermis. In the surrounding papillary dermis, a slight reduction in elastic tissue was noted.
Since its first description, CO2L has gained considerable recognition in the aesthetic field, stimulating neocollagenesis depending on the amount of heat supplied and the depth of its dermal and epidermal penetration.7,8 Additionally, the longer the ablation column, the greater the stimulus for dermal remodeling in deeper scar regions, resulting in improved outcomes for fine lines, acne scars, and photodamaged skin.9,10 Fractionated CO2L pulse energy has been identified as a critical factor in determining the extent and depth of ablation, thermal damage, and collagen remodeling.11,12 Baumann et al. concluded differences in the properties of ablative zones are not directly proportional to the total amount of energy applied.12 Thus, studies evaluating ablation columns resulting from different therapeutic methods are of great interest.
Arisa and Ortiz et al.2 demonstrated treatment with fractionated CO₂L produced greater ablation columns compared to the surgical method. The increased ablation depth led to more significant skin retraction, resulting in better final aesthetic outcomes for scars.4 In contrast, LTP technology has gained prominence, particularly in noninvasive blepharoplasty. Its mechanism of action involves inducing the expression of key genes such as type I collagen, transforming growth factors (TGF-β1 and TGF-β2), and alpha-smooth muscle actin (α-SMA). Plasma treatment triggers a coordinated response of transcription factors essential for wound healing, promoting re-epithelialization, angiogenesis, and oxidation of the lipid layer.13
The plasma spark generated by LTP sublimates the superficial skin layers without causing excessive thermal damage by coagulating dermal vessels, maintaining controlled heating. The energy is concentrated in small areas (~1 mm in diameter), allowing for precise and targeted tissue action while minimizing damage to deeper layers.14
Our findings revealed variations in coagulation column measurements: the diameter produced by LTP was approximately four times larger than that achieved with CO2L, whereas CO2L reached an ablation depth twice that of plasma. Considering areas with low dermal thickness, such as the eyelids, this shallower penetration combined with greater surface coverage may explain the increasing popularity of LTP in nonsurgical blepharoplasty. Such histological differences suggest each technology offers distinct yet complementary therapeutic possibilities, supporting individualized treatment approaches.
According to Baroni, the advantages of LTP include high precision, short procedure time, absence of bleeding, minimal collateral tissue damage, rapid formation of a postoperative protective layer, fast wound healing, and an immediate return to daily activities, with fewer unwanted effects.14 Our findings suggest when applied to thinner skin regions, LTP provides greater protection for deeper layers, more precise and controlled heating, fewer complications during application, faster recovery, and fewer side effects compared to CO2L.
However, further studies comparing the histological characteristics of MTZs across these techniques, along with their clinical outcomes, are necessary to validate these findings.
Studies on CO2L ablation layers associate greater depth with improved results. However, there is a lack of studies comparing CO2L with LTP. Our findings suggest that the greater diameter and shallower depth of the ablation column are key characteristics that support the use of plasma, particularly in areas with delicate skin. These properties contribute to fewer complications during and after the procedure, faster recovery, and excellent aesthetic outcomes. Nonetheless, further studies are required to confirm this relationship.
Ana Gabriella Bandeira Freire Andrade
ORCID: 0000-0002-8023-0134
Statistical analysis; approval of the final version of the manuscript; study conception and design; manuscript drafting and writing; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the propaedeutic and/or therapeutic management of studied cases; critical literature review; critical manuscript review.
Rossana Cantanhe de Farias de Vasconcelos
ORCID: 0000-0002-6185-1840
Statistical analysis; approval of the final version of the manuscript; data collection, analysis, and interpretation; active participation in research supervision; intellectual contribution to the propaedeutic and/or therapeutic management of studied cases; critical manuscript review.
João Guilherme Finizola de Vasconcelos
ORCID: 0000-0003-1588-4083
Statistical analysis; data collection, analysis, and interpretation; intellectual contribution to the propaedeutic and/or therapeutic management of studied cases.
Ana Maria Bertelli Antonio Gallotti
ORCID: 0000-0003-3113-0564
Author contributions: Study conception and design; active participation in research supervision; critical manuscript review.
Caroline Costa de Mendonça
ORCID: 0000-0003-3308-6093
Statistical analysis; study conception and design; manuscript drafting and writing; data collection, analysis, and interpretation; active participation in research supervision; critical literature review.
1. Costa FB, El Ammar ABPC, Campos VB, Kalil CLPV. Complications in laser dermatologic surgery. Part II: fractional and non-fractional ablative laser and fractional non-ablative laser. Surg Cosmet Dermatol 2011;3(2):135-46.
2. Pozner JN, DiBernardo BE. Resurfacing a laser. Clin Plast Surg. 2016;43(3):515-25.
3. Franck P, Henderson PW, Rothaus KO. Basics of lasers. Clin Plast Surg. 2016;43(3):505-13.
4. Ortiz AE, Goldman MP, Fitzpatrick RE. Ablative CO2 lasers for skin tightening: traditional versus fractional. Dermatol Surg. 2014;(40 Suppl)12:S147-51.
5. Duarte S, Panariello BHD. Comprehensive biomedical applications of low temperature plasmas. Arch Biochem Biophys. 2020;693:108560.
6. DeBruler DM, Blackstone BN, Baumann ME, McFarland KL, Wulff BC, Wilgus T, et al. Inflammatory responses, matrix remodeling, and re-epithelialization after fractional CO2 laser treatment of scars. Lasers Surg Med. 2017; 49(7), 675–685.
7. Bentkover SH. Plasma skin resurfacing: personal experience and long-term results. Facial Plast Surg Clin North Am. 2012; 20(2):145–162.
8. Omi T, Numano K. The role of the CO2 laser and fractional CO2 laser in dermatology. Laser Ther. 2014; 23(1):49–60.
9. Tierney EP, Hanke CW, Petersen J. Ablative fractionated CO 2 laser treatment of photoaging: a clinical and histologic study. Dermatologic Surg. 2012; 38(11):1777–1789.
10. Anderson RR, Donelan MB, Hivnor C, Greeson E, Ross EV, Shumaker PR, et al. Laser treatment of traumatic scars with an emphasis on ablative fractional laser resurfacing: consensus report. JAMA Dermatol. 2014;150:18793.
11. Schmitt L, Huth S, Amann PM, Marquardt Y, Heise R, Fietkau K, et al. Direct biological effects of fractional ultrapulsed CO2 laser irradiation on keratinocytes and fibroblasts in human organotypic full-thickness 3D skin models. Lasers Med Sci. 2018;33(4):765-772.
12. Baumann ME, Blackstone BN, Malara MM, Clairmonte IA, Supp DM, Bailey JK, et al. Fractional CO2 laser ablation of porcine burn scars after grafting: is deeper better? Burns. 2020;46(4):937-948.
13. Gan Lu, Jiang J, Duan JW, Wu XJZ, Zhang S, Duan XR, et al. Cold atmospheric plasma applications in dermatology: a systematic review. J Biophotonics. 2021;14(3):e202000415.
14. Baroni A. Non - surgical blepharoplasty with the novel plasma radiofrequency ablation technology. Skin Res Technol. 2020; 26(1):121-124.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}