


José Antonio Jabur1; Selma Schuartz Cernea2; Bianca Spina Papaleo1; Rute Facchini Lellis3
Financial support: None.
Conflicts of interest: None.
Submitted on: 07/19/2023
Approved on: 11/01/2023
How to cite this article: Jabur JA, Cernea SS, Papeleo BS, Lellis RF, Rêgo LC. Recurrent extramammary Paget's disease successfully treated with peripheral Mohs micrographic surgery associated with rapid immunohistochemistry. Surg Cosmet Dermatol. 2023;15:e20230280.
Extramammary Paget's disease is a slow-progressing, cutaneous adenocarcinoma of the apocrine glands with an uncertain etiology. The standard treatment is surgical removal of the tumor. However, the usual surgical methods - wide local excision and Mohs micrographic surgery - pose challenges and high recurrence rates. Often, these are extensive lesions with poorly defined boundaries located in critical anatomical regions. Additionally, they exhibit unpredictable subclinical intraepithelial spread. We present a case of a recurrent extramammary Paget's disease successfully treated with peripheric Mohs micrographic surgery associated with rapid immunohistochemistry for CK8/18.
Keywords: Paget Disease, Extramammary; Mohs Surgery; Immunohistochemistry
Extramammary Paget's disease (EMPD) is a rare, slow-progressing cutaneous adenocarcinoma of the apocrine glands with an unclear etiology.1 Raising awareness of this disease is crucial, since diagnosis is often late, and recurrence rates tend to be high.2
Desquamative and erythematous plaques affect older people and are common on the vulva, perianal region, pubis, penis, scrotum, and inguinal region.3 Dermatologists should suspect EMPD in unilateral, chronic lesions located in typical areas, in older patients, and refractory to treatment. Diagnosis is based on pathological examination, with the presence of Paget's cells, associated with positive immunohistochemistry (IHC) for cytokeratin 7 (CK7) or cytokeratin 8/18 (CK8/18).1,3
The standard treatment for EMPD is to remove the tumor surgically. This can basically be a wide local excision (WLE) with a predetermined margin or through techniques that evaluate 100% of the operative margins, such as staged surgeries or Mohs micrographic surgery (MMS).
Alternatively, some patients can also be treated with topical application of imiquimod, with good results.4
Advanced age, tumor extension, poorly defined boundaries, and an affected anatomical region often hinder the use of wide margins. Although the margin to be applied in these patients is unclear in the literature, some authors agree on 2 to 3cm.2 In addition, WLE has high recurrence rates, which vary from 22% to 60%, depending on the study and characteristics of the tumor.5,6
The typical subclinical spread and high recurrence rates favor the use of MMS or staged surgeries.5 In the case of MMS, however, it is difficult to identify subtle intraepithelial neoplastic proliferations using hematoxylin & eosin (HE) stain for fresh frozen sections.5
On the other hand, this can be overcome in staged surgeries, in which the margins are analyzed in paraffin, possibly using IHC, at the cost of several surgical times until the lesion has been cleared up.
Therefore, rapid IHC techniques have been described to aid the intraoperative assessment of the margins of intraepithelial tumors with extensive subclinical spread.7 This report describes the case of a patient with recurrent EMPD, successfully treated with MMS associated with rapid IHC for CK8/18.
A 73-year-old male patient presented with recurrent EMPD located in the inguinal region and pubis (Figure 1) for years. The patient had coronary insufficiency and was taking warfarin. He was initially treated with imiquimod, administered five times a week for 15 weeks. He was treated once again with imiquimod with no success. He then underwent two surgical resections with a 10mm margin at an interval of 1 year, with a persistent local recurrence. There was no evidence of invasion or involvement of internal organs at any time.
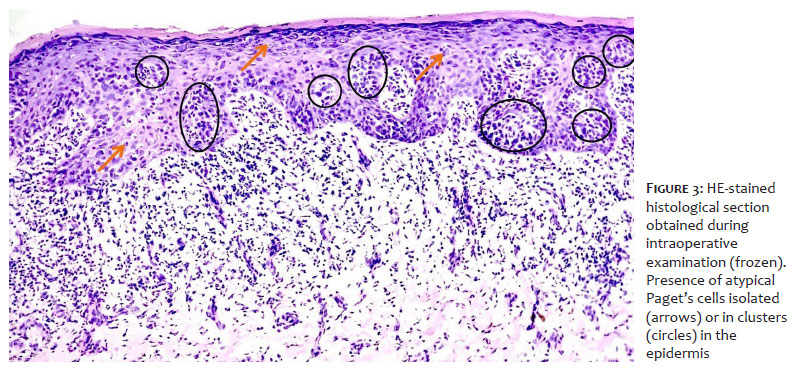
The patient was then submitted to peripheral MMS associated with rapid IHC for CK8/18 (Novodiax ihdDirect®). For debulking, the tumor was marked and excised in the superficial subcutaneous plane. We decided to include the perilesional hypochromic area in this stage of the surgery (Figure 2). Debulking was assessed using vertical HE sections, in which Paget's cells were observed between the keratinocytes in all layers of the epidermis (Figure 3). The first phase of MMS was then marked with a 5 to 8mm margin (Figure 4).
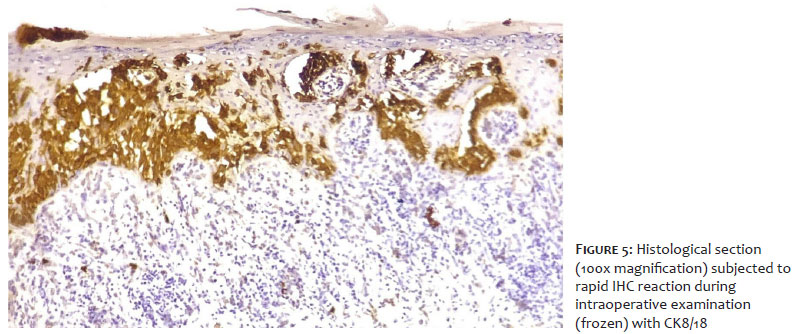
The peripheral margin was incised at 90º, processed using en face sections, initially stained with HE, and the slides were examined by an experienced dermatopathologist. Margins that were negative or doubtful on HE were submitted to rapid IHC for CK8/18. In this case, no HE-negative margins were positive on IHC. However, in the margins suspected of being positive, Paget's cells were stained brown on the IHC, confirming their presence in the keratinocytes (Figure 5).
The lesion required two phases and 14 fragments to clear, creating a surgical defect measuring 90 x 75mm. Reconstruction by approximation of the edges, associated with second intention, was then performed after the margins had been cleared. The patient was followed up in the outpatient clinic for 9 months with no recurrence (Figures 6 and 7). Due to the Covid-19 pandemic, medical interviews were conducted by telephone, the last of which took place 35 months after surgery, when no recurrence was reported. The patient died of other causes 36 months after surgery.
The case studied illustrates a frequent situation in EMPD. An older patient with an extensive lesion in the perigenital region and a history of multiple recurrences to treatment. Due to associated comorbidities, treatment was initially attempted with topical treatment with imiquimod. Non-invasive therapies, such as imiquimod, may be indicated for patients in whom surgical morbidity may be considered high. A recent review identified 276 patients treated with imiquimod, in which a complete response was observed in 30% of cases and a recurrence rate of 35.4%.8 In our experience, in addition to recurrence rates, prolonged exposure time to the drug and intense local inflammatory reaction also add morbidity and should be considered when choosing a therapy.
Local surgical excision was unsuccessfully attempted after imiquimod proved unsuccessful. In this technique, the vertical processing of the surgical specimen limits the assessment of the margins to less than 0.1%,5 which is reckless in lesions with poorly defined boundaries, an irregular growth pattern and extensive subclinical dissemination.7
In a meta-analysis evaluating the efficacy of MMS in the treatment of EMPD, the recurrence rate observed was 12.2% over a mean follow-up of 27.5 months.9 This rate is considered high when compared to other skin tumors routinely treated with MMS. Part of these recurrences are believed to be due to the difficulty in visualizing intraepithelial malignant cells in HE frozen sections.5 In these cases, rapid IHC is useful, as it highlights the malignant cells and can facilitate adequate control of the margins.7
In this case, IHC did not change the interpretation of the margins. However, it was performed by an experienced dermatopathologist, which does not reflect the Mohs surgeon's routine. Damavandy et al. in their 2018 study evaluated the use of IHC to interpret margins in EMPD treated with MMS. In this study, the authors reported a recurrence rate of 5.6% in recurrent tumors treated with staged surgery associated with IHC for CK7, compared to a 50% recurrence rate in patients in whom IHC was not used. However, surgical treatment required up to 5 days to complete.8
In our experience, peripheral MMS associated with rapid IHC provided prolonged remission of a recurrent tumor; it was performed in an outpatient setting and in a single surgical procedure. It also avoided the use of extensive margins, which reduced the morbidity of the surgery. However, the high cost and low availability of reagents in our setting are still an obstacle to the diffusion of this technique. Future studies will be useful in proving the real value of rapid IHC in the surgical treatment of EMPD.
José Antonio Jabur
ORCID: 0000-0002-5780-0653
Study design and planning; writing of the manuscript; critical review of the manuscript.
Selma Schuartz Cernea
ORCID: 0000-0002-0710-5935
Approval of the final version of the manuscript.
Bianca Spina Papaleo
ORCID: 0000-0002-8380-9088
Preparation and writing of the manuscript; data collection, analysis, and interpretation.
Rute Facchini Lellis
ORCID: 0000-0001-7690-0513
Intellectual participation in the propaedeutic and/or therapeutic conduct of the studied cases.
1. Extramammary Paget's disease [Internet]. Available from: www.blackwellpublishing.com/bjog
2. Wollina U, Goldman A, Bieneck A, Abdel-Naser MB, Petersen S. Surgical treatment for Extramammary Paget's disease. Curr Treat Options Oncol. 2018;19(6).
3. Kanitakis J. Mammary and extramammary Paget's disease. J Eur Acad Dermatology Venereol. 2007;21(5):581–90.
4. Dogan A, Hilal Z, Krentel H, Cetin C, Hefler LA, Grimm C, et al. Paget's disease of the vulva treated with imiquimod: case report and systematic review of the literature. Gynecol Obstet Invest. 2017;82(1):1–7.
5. Hendi A, Brodland DG, Zitelli JA. Extramammary Paget's disease: surgical treatment with Mohs micrographic surgery. J Am Acad Dermatol. 2004;51(5):767–73.
6. Damavandy AA, Terushkin V, Zitelli JA, Brodland DG, Miller CJ, Etzkorn JR, et al. Intraoperative immunostaining for cytokeratin-7 during Mohs micrographic surgery demonstrates low local recurrence rates in extramammary Paget's disease. Dermatol Surg. 2018;44(3):354–64.
7. Trimble JS, Cherpelis BS. Rapid immunostaining in Mohs: current applications and attitudes. Dermatol Surg. 2013;39(1 Pt 1):56–63.
8. Kibbi N, Owen JL, Worley B, Wang JX, Harikumar V, Downing MB, et al. Evidence-based clinical practice guidelines for Extramammary Paget disease. JAMA Oncol. 2022;8(4):618–28.
9. 9. Bae JM, Choi YY, Kim H, Oh BH, Roh MR, Nam K, et al. Mohs micrographic surgery for Extramammary Paget disease: a pooled analysis of individual patient data. J Am Acad Dermatol. 2013;68(4):632–7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}