


Ana Claudia Rolim Branco; Bruna Mendes Almeida; Clóvis Antônio Lopes Pinto; Célia Antônia Xavier de Moraes Alves
Financial support: None.
Conflicts of interest: None.
Submitted on: 12/14/2023
Approved on: 05/09/2024
How to cite this article: Branco ACR, Almeida BM, Pinto CAL, Alves CAXM. Cylindroma: a rare tumor in a typical site. Surg Cosmet Dermatol. 2024;16:e2024160332.
Cylindroma is a rare benign neoplasm of probable origin in the eccrine sweat glands and is characterized by papular and nodular, painless, slow-growing lesions, generally located on the head, neck and scalp. When multiple, they can be part of hereditary syndromes. The authors report the case of a patient with a solitary nodulation on the scalp, presenting pathological examination compatible with cylindroma. The lesion was excised, with satisfactory results and no recurrence.
Keywords: Sweat Gland Neoplasms; Skin Neoplasms; Deubiquitinating Enzyme CYLD.
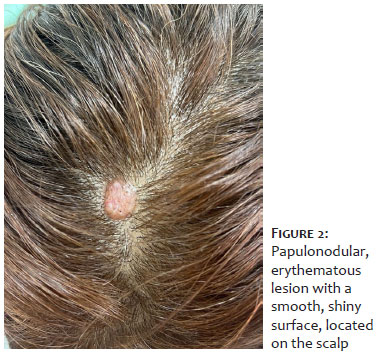
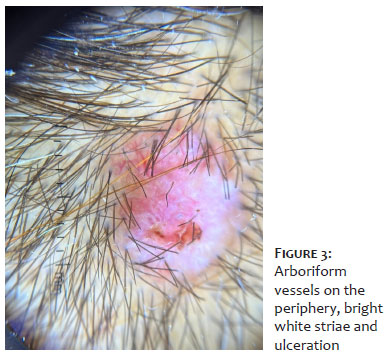
A 48-year-old female patient came to the Dermatology Department complaining of the appearance of an erythematous papule on her scalp about a year ago, which had progressed and became a painless nodule. No other associated skin lesions were reported. Her personal history included schistosomiasis and regular follow-up. There was no family history of the same condition or use of continuous medication. Dermatological examination revealed a papulonodular, erythematous lesion with a fibroelastic consistency and a smooth, shiny surface in the parietal region of the scalp (Figures 1 and 2). Dermoscopy showed arboriform vessels on the periphery of the lesion, and bright white striae and ulceration (Figure 3).
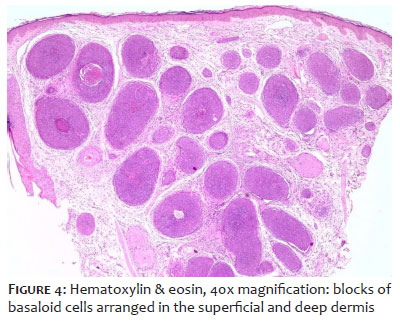
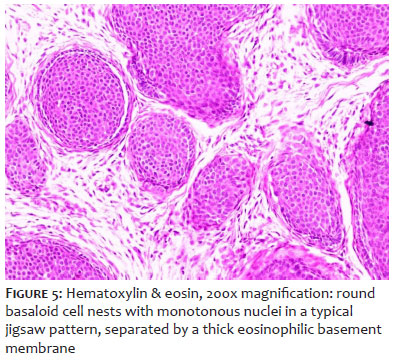
The anatomopathological examination showed basaloid neoplasia, forming cell blocks of different sizes, arranged in the superficial and deep dermis, permeated by collagen matrix and stromal fusocellular proliferation. The cell blocks were well delimited, resembling pieces of a jigsaw puzzle. In addition, the cells were round with monotonous nuclei, no atypia, and a palisade arrangement was identified on the periphery. Sometimes ductal differentiation was seen in the center of the cell blocks (Figures 4 and 5).
The diagnosis of cylindroma was then confirmed, and a decision to completely excise the lesion was made, with closure using a double rhomboidal flap, with an excellent final aesthetic result.
Cylindroma is a rare benign neoplasm of the cutaneous adnexa, probably originating in the eccrine sweat glands, although the literature still differs as to its histogenesis.1,2 Clinically, it presents as papulonodular, firm, fibroelastic, well-circumscribed, painless, slow-progressing, pinkish to reddish or even bluish lesions, measuring from a few millimeters to a few centimeters in size, and may have arboriform telangiectasias on their surface. In general, cylindroma develops as solitary lesions on the head, neck, and scalp.3-6 The confluent growth of multiple cylindromas covering the entire scalp is historically known as a turban tumor.3,4 These tumors are frequently seen in middle-aged and older women, and no racial disparity has been reported.1,6 Although they can rarely be found solitarily and sporadically, cylindromas, especially when multiple or with an early onset, are observed in autosomal dominant hereditary syndromes with mutations in the CYLD gene.1,2,4,6 Familial cylindromatosis is characterized by multiple cylindromas usually located on the scalp. Cylindromas associated with multiple trichoepitheliomas are found in familial multiple trichoepithelioma syndrome. Brooke-Spiegler syndrome is considered an overlap of these two conditions, characterized by the presence of numerous adnexal tumors, mainly located on the scalp and face, including cylindromas, spiradenomas, and trichoepitheliomas.3,4,5,7 Genetic counselling may be indicated in patients with multiple cylindromas, spiradenomas, or trichoepitheliomas or in the presence of a single cylindroma in a first-degree relative with a history of cylindroma.4,5 Dermoscopy shows the presence of arboriform telangiectasias, more prominent in the periphery of the tumor, and a homogeneous pinkish-white background and linear white striae.8 Histologically, cylindromas consist of dermal nodules, not encapsulated, formed by nests of basaloid cells in a typical puzzle pattern, separated by a thick eosinophilic basement membrane. The peripheral cells are generally small, hyperchromatic, and palisade-shaped. The central cells are larger, pale and have vesicular nuclei.3,4,6,9 The histological appearance of clusters of basaloid cell nests similar to cylinders when cut transversely has led to the descriptive term cylindroma.4,5 Cellular pleomorphism and mitoses are generally absent.3 Although rare, malignant transformation can occur in around 5-10% of patients, being more frequent in those with a mutation in the CYLD gene, given the presence, in general, of multiple lesions.1,3,4,9,10 Suspicious clinical features for malignancy include rapid growth, bleeding, ulceration and changes in color.2,3,4,9 In suspicious cases, radiological imaging, preferably MRI, should be considered, given the possibility of local invasion.5,6 Standard treatment consists of surgical excision and is recommended in cases of suspected malignant transformation, functional impairment, or for aesthetic reasons.1 For solitary lesions, curettage and cryotherapy are therapeutic options, while for small lesions, CO2 laser can be a tool.2,6 Finally, recurrence rates are relatively high, so extensive and complete removal of the tumor is recommended.2,5
Ana Claudia Rolim Branco
ORCID: 0009-0006-9564-1813
Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical review of the manuscript.
Bruna Mendes Almeida
ORCID: 0000-0002-0804-5401
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical review of the manuscript.
Clóvis Antônio Lopes Pinto
ORCID: 0000-0003-1711-0081
Approval of the final version of the manuscript; active participation in research orientation; critical review of the manuscript.
Célia Antônia Xavier de Moraes Alves
ORCID: 0000-0002-8421-8837
Author's contribution: Approval of the final version of the manuscript; active participation in research orientation; critical review of the
manuscript.
1. Cunha RA, Batista CB, Pinto FM, Issa MC, Rochael MC, Duraes SMB. Cylindroma: typical presentation of uncommon tumor. J Am Acad Dermatol. 2013;68(4):AB160.
2. Singh DD, Naujoks C, Depprich R, Schulte KW, Jankowiak F, Kubler NR, et al. Cylindroma of head and neck: review of the literature and report of two rare cases. J Craniomaxillofac Surg. 2013;41(6):516-521.
3. Russo R, Herzum A, Cozzani E, Paudice M, Guadagno A, Parodi A. Multiple rubbery nodules on the scalp. J Am Acad Dermatol. 2021;8:80-82.
4. Dubois A, Hodgson K, Rajan N. Understanding inherited Cylindromas: clinical implications of gene discovery. Dermatol Clin. 2017;35(1):61-71.
5. Rajan N, Ashworth A. Inherited cylindromas: lessons from a rare tumor. Lancet Oncol. 2015;16(9):460-469.
6. Massoumi R, Paus R. Cylindromatosis and the CYLD gene: new lessons on the molecular principles of epithelial growth control. Bioessays. 2007;29(12):1203-1214.
7. Jordao C, Magalhaes TC, Cuzzi T, Silva MR. Cylindroma: an update. Int J Dermatol. 2015;54(3):275-278.
8. Neema S, Sandhu S, Kashif A W. Dermoscopy of cylindroma. Indian Dermatol Online J. 2022;13(6):818–819.
9. Kazakov DV. Brooke-Spiegler syndrome and phenotypic variants: an update. Head Neck Pathol. 2016;10(2):125-130.
10. Mataix J, Banuls J, Botella R, Laredo C, Lucas A. Brooke-Spiegler syndrome: an heterogeneous entity. Actas Dermosifiliogr. 2006;97(10):669-672.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}