


Cíntia Ávila Souza1; Isabella Prado Motta1; Rodrigo Leite Azevedo1; Eliane Maria Ingrid Amstalden2; Thais Helena Buffo1
Financial support: None.
Conflicts of interest: None.
Submitted on: 20/09/2023
Approved on: 22/10/2023
How to cite this article: Souza CA, Motta IP, Azevedo RL, Amstalden EMI, Buffo TH. Fibromyxosarcoma mimicking a benign cystic lesion: a case report of a high-grade mesenchymal tumor in an atypical site. Surg Cosmet Dermatol. 2023;15:e20230305.
Fibromyxosarcoma is a rare subtype of soft tissue sarcoma characterized by the presence of spindle cells and myxoid matrix. We report the case of an older patient who presented with progressive growth of a nodule in the interscapular region, and further investigation confirmed the diagnosis of high-grade fibromyxosarcoma. Notably, this neoplasm more commonly occurs in the lower limbs and may exhibit recurrence associated with increased histological grade. Therefore, early diagnosis and treatment are crucial for mitigating morbidity and mortality. We emphasize the significance of diagnosing an atypical case and providing timely therapeutic intervention, contributing to the optimization of clinical outcomes.
Keywords: Sarcoma; Neoplasms, Connective and Soft Tissue; Solitary Fibrous Tumors
Fibromyxosarcoma is a rare subtype of soft tissue sarcoma, composed of spindle cells and myxoid stroma. It is the most common mesenchymal neoplasm in older patients, presenting as painless, slow-progressing nodules, common in the lower extremities.1 Histologically, according to cellularity and atypia, they can be classified as low, intermediate, or high grade. This classification has no correlation with the high risk of recurrence (between 50-60% for all subtypes), but it is a predictor of metastases, which are present in 20-35% of intermediate and high grades, and are uncommon in low-grade sarcomas.2 Unlike other sarcomas, myxofibrosarcomas tend to gradually present with a higher histological grade with each recurrence.3 This highlights the importance of early diagnosis, staging, and treatment, with a view to lower morbidity and mortality. We report the case of an older patient with high-grade myxofibrosarcoma in the interscapular region.
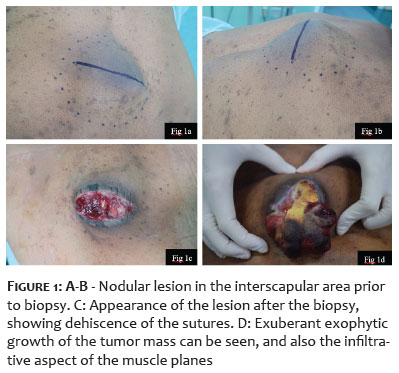
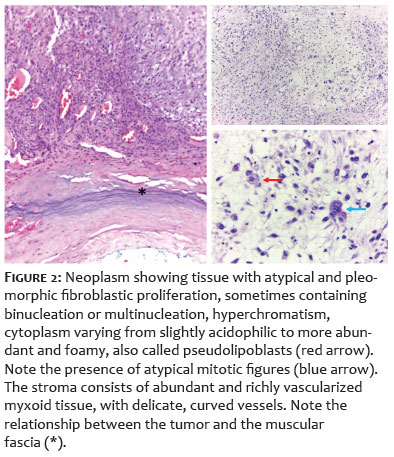
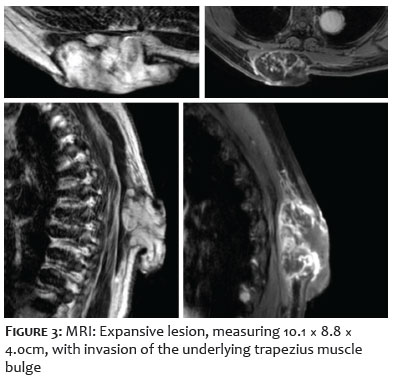
A 68-year-old female patient presented with a one-year-old, painless nodular lesion in the interscapular region. The initial dermatological physical examination revealed a painless, mobile nodular lesion measuring 6 × 4cm. She had a previous soft tissue USG at the beginning of the condition, compatible with an epidermal cyst with free muscle planes Figures 1A-1B). As the clinical picture was not consistent with the imaging exam, a CT scan was requested, which showed that it was a 7 × 3cm cystic lesion, and excision was scheduled. Following incision, amorphous, gelatinous, blackened tissue could be seen, not corresponding to the initial hypothesis (Figures 1C-1D). A deep biopsy of the lesion was then performed, with histopathological results showing a high-grade myxofibrosarcoma (Figure 2). Magnetic resonance imaging of the spine was requested, showing the presence of an expansive lesion measuring 10.1 × 8.8 × 4.0cm, invading the muscle bulge of the underlying trapezius, with no signs of invasion of other muscle planes or adjacent bone structures (Figure 3). For staging, a PET-CT scan was performed, which showed hypermetabolism in bilateral axillary lymph nodes, suggestive of metastases, not confirmed through biopsy of the hypercapturing lymph nodes (Figure 4). The patient was referred to the Orthopedics team and the lesion was excised with wide margins. The patient was then referred to Oncology for clinical follow-up, and no adjuvant treatments were indicated. The patient is being followed up by a multidisciplinary team six months after excision, with no recurrence (Figure 5).
Fibromyxosarcoma is a rare subtype of soft tissue sarcoma, first described by Enzinger and Weiss in 1977.1 Previously called malignant fibrous histiocytoma myxoid variant, it has a mesenchymal origin and is composed of spindle cells and myxoid stroma. It is the most common malignant mesenchymal neoplasm in older patients, predominantly affecting males in the 50s to 70s.1-3
The most common site is the lower limbs, with lesions rarely occurring in the trunk, upper limbs, or cephalic segment. In general, it presents as painless, slow-progressing, normochromic, or slightly erythematous nodules or tumors. It occurs more frequently in subcutaneous soft tissues than in deep tissues.1,4,5
Histopathological examination is the gold standard for diagnosing the disease. The sample must be deep to guarantee a reliable assessment of the material. Superficial biopsies can show benign characteristics or even subclassify a high-grade tumor.6 Histologically, it is classified as low, intermediate, or high grade, according to cellularity and atypia. Immunohistochemistry shows low specificity in myxofibrosarcoma and is generally positive for vimentin and rarely for smooth muscle actin, S100, and desmin.6,7
The treatment of choice is excision of the lesion with wide margins. Local recurrence occurs in 50-60% of cases, and this risk is apparently not related to the depth of the lesions or the histological grade.8 However, there is a tendency for the myxofibrosarcoma to gradually become more cellular, more pleomorphic, more mitotically active, and thus have a higher histological grade with each recurrence. This characteristic is not observed in other sarcomas. Metastases are rare in low histological grade tumors, but occur in 20-35% of intermediate and high grade tumors, especially to the lungs and bones. The differential diagnosis includes other myxoid tumors.1,2,8
The ability of the tumor to present high rates of recurrence and advance in histological grade supports the need for early diagnosis and treatment, so as to reduce morbidity and mortality.
Cíntia Ávila Souza
ORCID: 0000-0001-8116-010X
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in the propaedeutic and/or therapeutic conduct of the cases studied; critical literature review; critical review of the manuscript.
Isabella Prado Motta 0009-0001-2858-578X
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in the propaedeutic and/or therapeutic conduct of the cases studied; critical literature review.
Rodrigo Leite Azevedo
ORCID: 0000-0001-8541-0591
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of the cases studied; critical literature review.
Eliane Maria Ingrid Amstalden
ORCID: 0000-0001-7958-2426
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of the cases studied.
Thais Helena Buffo
ORCID: 0000-0002-6833-7596
Author's contribution: Statistical analysis; approval of the final version of the manuscript; study design and planning; active participation in research orientation; critical review of the manuscript.
1. Mentzel T, Calonje E, Wadden C, Camplejohn RS, Beham A, Smith MA, et al. Myxofibrosarcoma. Clinicopathologic analysis of 75 cases with emphasis on the low-grade variant. Am J Surg Pathol. 1996;20(4):391–405.
2. Mentzel T, Fletcher CDM. Low-Grade Myxofibrosarcoma. Pathology Case Reviews. 1998;3(3):139–42.
3. Mentzel T. Sarcomas of the skin in the elderly. Clin Dermatol. 2011;29(1):80–90.
4. Dore A, Robertson I, Williamson R, Weedon D. Progression of a myxoid pleomorphic fibroma to myxofibrosarcoma. Australas J Dermatol. 2003;44(4):287–90.
5. Nascimento AF, Bertoni F, Fletcher CDM. Epithelioid variant of Myxofibrosarcoma: expanding the clinicomorphologic spectrum of Myxofibrosarcoma in a series of 17 cases. Am J Surg Pathol. 2007;31(1):99–105.
6. Kosemehmetoglu K, Vrana JA, Folpe AL. Tumors of the soft tissues. In: Kumar V, Abbas AK, Aster JC, editors. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Philadelphia: Elsevier; 2015. p. 1353-5.
7. Enzinger FM, Weiss SW. Soft tissue tumors. 3rd ed. St. Louis: CV Mosby, 1995.
8. Maretty-Kongstad K, Aggerholm-Pedersen N, Keller J, Safwat A. Recurrence and treatment outcome in 92 patients with fibromyxoid sarcoma from a single institution. Clin Orthop Relat Res. 2016;474(11):2523-2530.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}