


Célia Luiza Petersen Vitello Kalil1; Valéria Campos2; Analupe Webber3; Laura de Mattos Milman4; Mariana Silveira Ferreira Mylius4; André Cartell5
Submitted on: 26/06/2023
Approved on: 26/09/2023
Financial support: None.
Conflict of interest: Célia Kalil, Valéria Campos, and Analupe Webber have received speakers' fees from Vydence Medical.
Ethics committee opinion: 79006717.0000.5335
How to cite this article: Kalil CLPV, Campos V, Webber A, Milman LM, Mylius MSF, Cartell A. Combination of Q-switched and micropulsed 1064-nm Nd:YAG laser for global facial improvement. Surg Cosmet Dermatol. 2023;15:e20230270.
The 1064-nm Nd:YAG laser in Q-switched and micropulsed modes has been used in rejuvenation, pore reduction, skin texture improvement, and wrinkle reduction. The aim of this study is to evaluate the combination of 1064-nm Nd:YAG laser in micropulsed and Q-switched modes in the same session for global facial treatment. Thirty female patients underwent six treatment sessions every two weeks. Three blinded dermatologists evaluated the results through clinical photographs and Visia® or Focco® images obtained before and 30 days after the last treatment session. The parameters of interest were solar melanosis, telangiectasias, wrinkles, dilated pores, melasma and skin texture. Three patients had face biopsies before and 30 days after the end of treatment. Most patients showed improvement in all evaluated parameters, except for two patients who had worsening of melasma. An increase in collagen was observed in two of the three histological examinations performed after treatment. The combination of laser modes studied herein offers a safe treatment that can improve wrinkles, skin texture, and laxity with minimal downtime.
Keywords: Lasers; Skin Aging; Rejuvenation
The use of non-ablative lasers for facial rejuvenation has increased in recent years. The neodymium:yttrium-aluminum-garnet (Nd:YAG) laser, in both nanosecond (Q-switched) and millisecond (LongPulse®) modes and, more recently, in microsecond mode, has been used for this purpose.1
The 1064-nm Nd:YAG laser has been widely used in dermatology for removal of hair, tattoos, pigmented and vascular lesions and has also gained popularity in dermal remodeling for rejuvenation.2,3 The micropulsed and Q-switched modes of Nd:YAG have potentially different effects due to differences in exposure time, pulse energy, and peak power. Pulse duration is related to the depth of dermal coagulation; in theory, the micropulsed mode would penetrate deeper into the dermis compared to the Q-switched mode, leading to greater skin remodeling.2
In the present study, 1064-nm Nd:YAG laser was applied in both micropulsed and Q-switched modes in the same session, seeking to combine the benefits of both techniques for global facial treatment while reducing downtime.
Thirty patients were selected from three study centers. Patients had to be female, between 30 and 55 years old, and have solar melanosis, telangiectasias, wrinkles, and/or enlarged pores. Pregnant or lactating women, patients with collagen disorders, those treated with photosensitizing drugs or oral or topical isotretinoin, those who had undergone a facelift less than one year ago, and those who received chemical peels or laser treatments (ablative or non-ablative) in the last four months were excluded from the study.
Three patients were voluntarily selected to undergo a 3-mm punch biopsy at the angle of the mandible before (baseline) and 30 days after the end of treatment. Treatments were only performed once the patient demonstrated understanding and signed an informed consent form (ICF). This study was approved by the relevant Ethics Committee.
Digital photographic evaluation of the patients' faces was performed using the Visia® (Canfield Imaging Systems, USA) and Focco® (Focco Photographs, Fabinject, Taubaté, São Paulo, Brazil) systems before and 30 days after the last treatment session.
Patients underwent six treatment sessions, every two weeks, with two Etherea® platform handpieces (Vydence Medical, São Carlos, São Paulo, Brazil): LongPulse® (1064-nm Nd:YAG, in Dynamics® mode) and Acroma-QS® (1064-nm Nd:YAG, Q-switched mode) belonging to the investigators. Both were used in the same session, at every session. All laser applications were performed by dermatologists.
Prior to treatment, subjects had their skin cleansed and were fitted with safety goggles for eye protection. Laser shots were applied to orbital-adjacent skin, but never within the orbital rim. The LongPulse® mode was applied with a 6-mm spot, fluence ranging from 8 to 10mJ/cm2, and pulse duration of 650μs, in a continuous motion until 2,000 shots had been completed on each hemiface and 1,000 shots on the forehead. The Acroma-QS® mode was applied with a 7-mm spot and fluence of 1200mJ/cm2, for a total of 2 to 3 passes across the face. The endpoint was defined by the number of shots, but the applicator was attentive and could stop the treatment earlier if the patient developed significant erythema or had experienced side effects in the previous session. No cooling was performed, nor was topical anesthetic applied before the sessions; these were considered superfluous due to the excellent tolerability of the treatment among our patients.
Patients were instructed to apply daily UVA/B sunscreen with a sun protection factor (SPF) greater than or equal to 30, which should be continued throughout the treatment and follow-up period. At each visit, patients were asked whether they had any adverse events between visits.
At the end of treatment, patients completed a questionnaire evaluating the following factors: spots, erythema, wrinkles, dilated pores, and skin texture, and described any transient (up to 5 days after the procedure) and persistent (up to 30 days after the procedure) adverse effects which may have occurred.
Results were evaluated jointly by three experienced dermatologists using clinical photographs as well as Visia® and Focco® images. The parameters solar melanosis, telangiectasias, wrinkles, enlarged pores, melasma and skin texture were evaluated on a five-point scale, scored as follows: worsening, slight improvement (1-25%), moderate improvement (26-50%), good improvement (51-75%) excellent improvement (>76%). Collagen analysis of biopsy specimens was performed by a blinded pathologist.
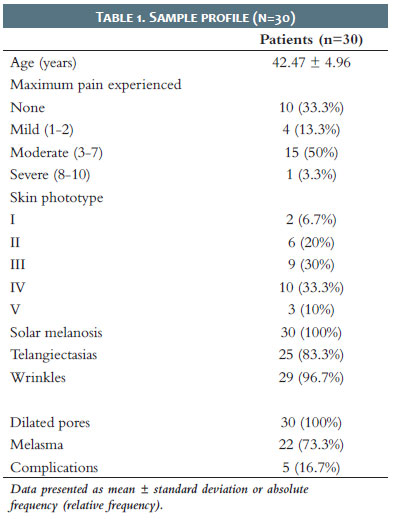
The sample consisted of 30 female patients aged 33 to 52 years (mean 42.47 ± 4.96 years). Skin phototypes I to V were represented, with III and IV being most frequent. All patients had melanosis and dilated pores, and most had wrinkles (96.7%), telangiectasias (83.3%), and melasma (73.3%) (Table 1).
All patients completed the study and treatment was well tolerated. At each visit, patients were asked about adverse effects after the sessions or complications between them. Although most patients experienced mild discomfort during the sessions, this did not prevent treatment continuity. Three patients had complications: one developed erythematous papules after one session, treated with low-potency topical corticosteroids; one had worsening of acne; and another had two episodes of facial edema which resolved spontaneously in less than 24 hours. Lower laser energy (Dynamics LongPulse® mode, fluence 8mJ/cm2; Acroma-QS®, 900mJ/cm2) was used in this patient's subsequent sessions, progressively increasing in each session.
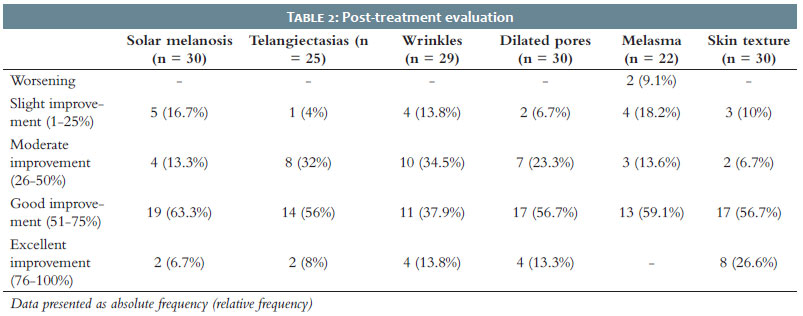
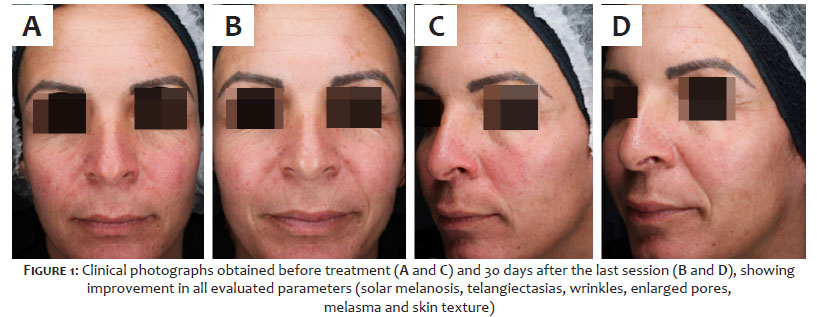
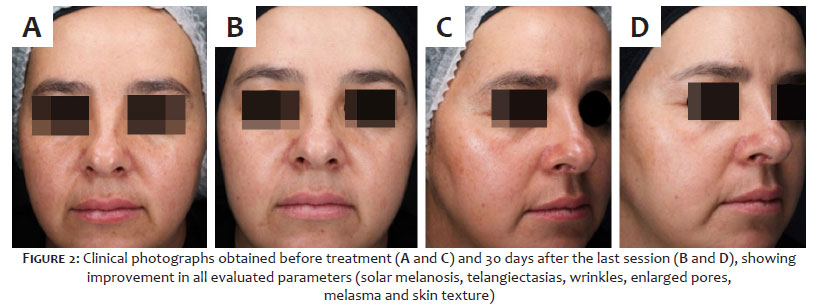
Most patients showed good or excellent improvement in all parameters of interest (Table 2). Except for two patients who had worsening of melasma, all other parameters, such as enlarged pores, telangiectasias, wrinkles, and solar melanosis, improved (Figures 1 and 2).
Histological examinations performed before treatment revealed fine collagen fibers in the dermis. Of the three patients who underwent biopsy, two (43 and 47 years old respectively) had an increase in collagen thickness on histology 30 days after the end of treatment. The youngest of the three patients (33 years old) showed no change in biopsy findings compared to the pre-treatment baseline.
The aging process is characterized by a reduction in collagen synthesis and an increase in its degradation due to increasing levels of metalloproteinases, which leads to a reduction in dermal thickness. Collagen fibers become disorganized, more compact, and granular; elastic fibers decrease in number and diameter.4 Clinically, cutaneous photoaging manifests as dyschromia, erythema, telangiectasias, wrinkles, changes in texture, and pore dilation.2
Several studies in the literature have documented the effects of 1064-nm Nd:YAG lasers in Q-switched and micropulsed modes on rejuvenation, pore reduction, skin texture improvement, and wrinkle reduction.2,5,6,7
The application of Nd:YAG laser at different pulse durations seems to be safe when used within the recommended parameters and can be useful to improve signs of photoaging with shorter recovery time and a lower risk of complications.8
Choi et al compared the effectiveness and safety of combination therapy using dual toning (low-fluence Q-switched and long-pulse Nd:YAG laser) in the treatment of melasma, and concluded that dual toning could represent a safe and effective treatment, as it is associated with minimal adverse events and improved treatment efficacy compared with Q-switched toning monotherapy.8,9
Laser treatment for photorejuvenation usually involves ablation of the superficial layers of the epidermis, with 10600-nm CO2 and 2940-nm Er:YAG being the most traditional lasers used for this purpose. Although effective, potential risks include a recovery period of up to 2 weeks, persistent erythema, bleeding, pain, infection, crusting, unwanted changes in texture, and scarring, with the greatest risk in patients with high skin phototype.5 As patients increasingly seek procedures that do not take them away from their activities, lasers associated with shorter downtime are gaining ground.
The Q-switched Nd:YAG laser emits a nanosecond pulse-width beam that selectively destroys melanosomes without affecting surrounding tissue. The high energy peak instantly increases the temperature of the chromophore, leading to changes in pressure and vibration, which then effectively destroys it in the form of a shock wave (photoacoustic effect).3,10 This laser is widely used for removal of hair, tattoos, and pigmented and vascular lesions.3,6 Goldberg and Metzler first suggested the concept of laser toning in 1999, in which multiple passes with a low-fluence Q-switched Nd:YAG laser produced beneficial changes in photoaging skin, such as improved skin tone and texture, reduction of pores, sebaceous secretion, rhytids, and dyschromia.5 Adverse events, including mottled hypopigmentation (MH) and rebound hyperpigmentation (RH), have been reported.3,8
The absorption of the 1064-nm wavelength of the laser by water is very low and the mechanism by which the Q-switched Nd:YAG laser can improve rhytids is not well established. It is believed to involve nonspecific dermal heating with subsequent collagen contraction.5
In 2001, in an anatomopathological study, Goldberg et al found mild fibrosis of the superficial papillary dermis with improvement in the organization of collagen fibers in four of six patients, suggesting that the Q-switched Nd:YAG laser would produce similar morphological changes, but to a lesser degree, than those observed with CO2 and Er:YAG ablative laser resurfacing.5 Berlin et al documented a slight decrease in elastosis, as well as increased vascularization and collagen deposition, in biopsies obtained 3 months after treatment with Q-switched Nd:YAG laser.11
Karabudak et al studied the use of Q-switched Nd:YAG laser in periorbital wrinkles in eight patients, finding an increase in collagen density in histopathological specimens from all patients. However, clinical improvement in rhytids was only observed in half of these individuals. The authors considered the treatment to be safe and effective in reducing periorbital wrinkles, especially in younger individuals.12 Tian reported the use of low-fluence Q-switched Nd:YAG laser in the treatment of post-blepharoepicantoplasty scars. Although the exact mechanism of scar remodeling by this laser is unclear, it is postulated that microscopic damage occurs repeatedly rather than actual tissue destruction. Heating of the scar leads to disruption of disulfide bonds, with subsequent collagen breakdown and remodeling.13
Micropulsed Nd:YAG, with pulse widths in the microsecond domain, would also lead to rejuvenation while maintaining a short downtime when applied in multiple passes. In this case, the formation of controlled zones of mild photothermal damage is believed to induce neocollagenous wound healing mechanisms.2,7 This laser can also be useful in reducing facial erythema, improving the appearance of keloid and hypertrophic scars, and enhancing skin texture.1,4
Schmults et al, in a study of nine patients, concluded that 1064-nm microsecond Nd:YAG lasers can produce new collagen formation in the papillary dermis, as demonstrated by a decrease in the overall diameter of collagen fibers, and suggest that these lasers can be also useful in reducing facial erythema and improving skin texture. Younger patients may form new collagen in greater amounts compared to older patients with photodamage.1
Roh et al, in a split-face controlled study with 20 patients, evaluated and compared the efficacy of the micropulsed and Q-switched modes of the 1064-nm Nd:YAG laser in the treatment of enlarged pores, finding that both had similar efficacy in reducing pore size and sebum level. They suggest that deposition of dermal collagen and remodeling of the perifollicular area could result in pore size reduction. The photothermal effect of the laser would result in a reduction of the sebaceous gland, which would account for the long-term maintenance of both reduced pore size and sebum level.2 In a similar study, Chung et al showed that the combination of micropulsed Nd:YAG with Q-switched mode improved enlarged pores, and the result could be optimized with the use of carbon lotion.7 In our study, all patients showed improvement in their enlarged pores; in 70% of patients, this improvement was greater than 50%.
Kang et al treated 30 female patients with melasma with the 1064-nm Nd:YAG laser in Q-switched mode, immediately followed by micropulsed mode. Patients received a total of 10 to 12 treatments repeated every 2 weeks. Overall, 67% had a fair to excellent degree of improvement and 7 (23%) had visible improvement, while little or no improvement was seen in 3 (10%) patients. There were no unexpected side effects. The dual toning technique using the 1064-nm Nd:YAG laser was safe, effective, and well tolerated.14
In the study, all patients had an improvement greater than 50% in wrinkles, telangiectasias, and solar melanosis, in addition to the aforementioned improvement in pores. Two patients (skin phototypes II and IV) had worsening of melasma, possibly secondary to micropulsed Nd:YAG, which causes greater thermal damage. The use of Nd:YAG laser in Q-switched mode for melasma is well established. The energy suggested by the company protocol for this treatment would be 600-900mJ/cm2. In our study, however, we used an energy density of 1200mJ/cm2 aiming at better photorejuvenation outcomes; this higher energy may have played a role in this complication. Nevertheless, it bears stressing that the other 20 patients with melasma included in the study showed improvement, which was scored as greater than 50% in 59.1% of these patients. Although clinical improvement was observed in all three patients who underwent before-and-after biopsies, collagen thickening was found in only two of them. As found by Goldberg et al, clinical improvement does not always correlate with histological findings.2
It is worth noting that the treatment protocol tested in the study was associated with a high level of patient satisfaction; a feeling that the skin was "fresher" was frequently reported by patients throughout the treatment. There were no serious adverse events.
The combined application of Nd:YAG laser in Q-switched and micropulsed modes provides a safe and effective treatment for sun-damaged skin. This technique can improve wrinkles, skin texture, and laxity with minimal downtime.
1. Schmults CD, Phelps R, Goldberg DJ. Nonablative facial remodeling: erythema reduction and histologic evidence of new collagen formation using a 300-microsecond 1064-nm Nd:YAG laser. Arch Dermatol. 2004;140(11):1373–6.
2. Roh M, Goo B, Jung J, Chung H, Chung K. Treatment of enlarged pores with the quasi long-pulsed versus Q-switched 1064 nm Nd:YAG lasers: split-face, comparative, controlled study. Laser Ther. 2011;20(3):175–80.
3. Lee SL, Lee YJ, Lee JM, Han TY, Lee JH, Choi JE. The Low-Fluence Q-Switched Nd:YAG laser treatment for melasma: a systematic review. Medicina (Kaunas). 2022;58(7):936.
4. Koike S, Akaishi S, Nagashima Y, Dohi T, Hyakusoku H, Ogawa R. Nd:YAG laser treatment for keloids and hypertrophic scars: an analysis of 102 cases. Plast Reconstr Surg Glob Open. 2015;2(12):e272.
5. Goldberg D, Metzler C. Skin resurfacing utilizing a low-fluence Nd:YAG laser. J Cutan Laser Ther. 1999;1(1):23–7.
6. Goldberg DJ, Silapunt S. Histologic evaluation of a Q-switched Nd:YAG laser in the nonablative treatment of wrinkles. Dermatol Surg. 2001;27(8):744–6.
7. Chung H, Goo B, Lee H, Roh M, Chung K. Enlarged pores treated with a combination of Q-switched and micropulsed 1064 nm Nd:YAG laser with and without topical carbon suspension: a simultaneous split-face trial. Laser Ther. 2011;20(3):181–8.
8. Choi CP, Yim SM, Seo SH, Ahn HH, Kye YC, Choi JE. Retrospective analysis of melasma treatment using a dual mode of low-fluence Q-switched and long-pulse Nd:YAG laser vs. low-fluence Q-switched Nd:YAG laser monotherapy. J Cosmet Laser Ther. 2015;17(1):2-8.
9. Choi CP, Yim SM, Seo SH, Ahn HH, Kye YC, Choi JE. Retreatment using a dual mode of low-fluence Q-switched and long-pulse Nd:YAG laser in patients with melasma aggravation after previous therapy. J Cosmet Laser Ther. 2015;17(3):129-34.
10. Kim JY, Choi M, Nam CH, Kim S, Kim MH, Park BC, Hong SP. Treatment of melasma with the photoacoustic twin pulse mode of low-fluence 1,064 nm Q-Switched Nd:YAG laser. Dermatol Surg. 2016;28(3):290–6.
11. Berlin AL, Dudelzak J, Hussain M, Phelps R, Goldberg DJ. Evaluation of clinical, microscopic, and ultrastructural changes after treatment with a novel Q-switched Nd:YAG laser. J Cosmet Laser Ther. 2008;10(2):76–9.
12. Karabudak O, Dogan B, Baloglu H. Histologic evidence of new collagen formation using a Q-switched Nd:YAG laser in periorbital rhytids. J Dermatolog Treat. 2008;19(5):300–4.
13. Tian WCBA. Savior of post-blepharoepicanthoplasty scarring: novel use of a low-fluence 1064-nm Q-switched Nd:YAG laser. J Cosmet Laser Ther. 2016;18(2):69–71.
14. Kang H, Kim J, Goo B. The dual toning technique for melasma treatment with the 1064 nm Nd: YAG laser: a preliminary study. Laser Ther. 2011;20(3):189–94.
Célia Luiza Petersen Vitello Kalil
ORCID: 0000-0002-1294-547X
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in research guidance; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript.
Valéria Campos
ORCID: 0000-0002-3350-8586
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in research guidance; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript.
Analupe Webber
ORCID: 0000-0002-8781-743X
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in research guidance; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript
Laura de Mattos Milman
ORCID: 0000-0002-3249-0396
Preparation and writing of the manuscript; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript
Mariana Silveira Ferreira Mylius
ORCID: 0000-0002-1741-8652
Preparation and writing of the manuscript; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript
André Cartell
ORCID: 0000-0003-1436-9418
Collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}