


Giseli Petrone; Marcio Serra
Financial support: None.
Conflict of interest: None.
Submitted on: 04/25/2023
Approved on: 02/15/2024
How to cite this article: Petrone G, Serra M. Evaluation of depressions and projections of facial aging, correlating them with anatomical structures, to help in volumization. Surg Cosmet Dermatol. 2024;16:e20240256.
Facial volumization techniques have been widely discussed by several authors. However, there is a dearth of publications on techniques for patient assessment. In this article, we describe how we assess, in our clinical practice, the anatomical changes associated with facial aging in a practical and didactic way, as it is a fundamental step when choosing products and filling techniques.
Keywords: Dermal fillers; Skin; Collagen; Inflammation; Blindness; Necrosis.
Diagnosing and identifying which areas should be treated, projected, and volumized is a major difficulty for the novice injector. We have noticed that literature is missing a step-by-step didactic approach to assessing the face, allowing for the development of clinical reasoning and an accurate diagnosis. We suggest that this diagnosis should be based on three pillars: loss of volume, loss of thickness and sagging, and loss of skin texture, or a combination of these. Therefore, treatment can only be indicated after evaluation and diagnosis of each case.
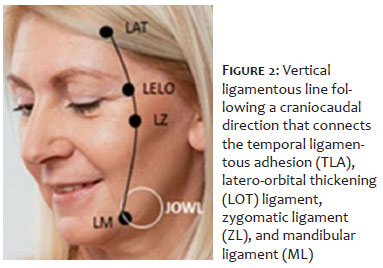
In 2012, Carruthers et al. defined an evaluation scale and the limits of the lower 2/3 of the face, dividing it into the upper cheek (UC) and lower cheek (LC) using a line that extends from the labial commissure to the upper edge of the tragus.1 The UC is limited superiorly by the infraorbital concave and extends from the lateral epicanthus of the eye to join the upper part of the helix of the ear; medially, it is limited by the nasal border and nasolabial fold to the labial commissure. Below the dividing line, the LC is limited medially by the mentolabial sulcus and inferiorly by the body of the mandible up to the earlobe. And the lateral limit of the LC extends from the upper part of the tragus to the earlobe (Figure 1).
More recent studies have attempted to establish anthropometric measurements in the quest for the aesthetically ideal and standardized face. However, the concept of beauty is highly variable and often Caucasian standards are used to determine therapeutic approaches, which we believe is not appropriate due to the great cultural and racial variety of the population.
These standards are therefore useful to help assess pre- and post-treatment results, but not to guide the start of treatment.2
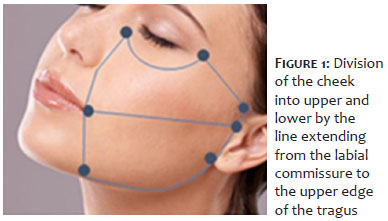
In our approach, we propose, in addition to the division into superior and inferior, to also define and limit this region into medial and lateral. This division may not have been proposed because of the absence of current anatomical knowledge about the vertical ligament line (VLL), which was recently described by Casabona et al. who, when comparatively evaluating fillers in the middle 1/3 in 12 patients, noted that the lifting effect obtained when filling the face laterally is due to the difference in the arrangement of the medial versus lateral subcutaneous layers.3 They showed that these layers are delimited by an imaginary VLL, which connects the temporal ligamentous adhesion (TLA) to the lateral orbital thickening (LOT) ligament, zygomatic ligament (ZL) and mandibular ligament (ML) of the face, following a craniocaudal direction, laterally to the orbital rim, up to the mandible. They concluded that when injected medially to this line, the aesthetic result is volumization, while laterally, the effect is to lift the middle and lower third of the face, thus requiring less material for volumization and facial lifting (Figure 2). Recently, Braz et al. reviewed this VLL based on the mobile and fixed areas of the face, suggesting that it should end in the mandible, post-jowl, considering the masseteric ligament and not the mandibular ligament.4 Therefore, dividing the cheek region into medial and lateral is necessary when assessing the patient.
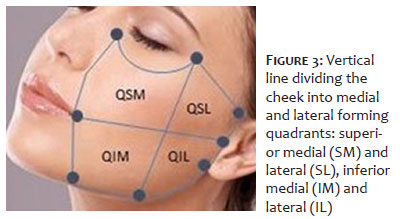
Didactically, the authors suggest adding a vertical imaginary line to the horizontal imaginary line already described,1 dividing the cheeks into medial and lateral. Associating this study by Braz et al. with an analysis by Nechala et al., who compared various techniques for locating the malar eminence,5 we propose a division that would start from the orbital bone ridge, where the LOT is located, passing through the ZL and descending perpendicularly to the medial pre-masseteric region of the mandible, thus dividing the face into quadrants: superior medial (SM) and lateral (SL), inferior medial (IM) and lateral (IL) (Figure 3).
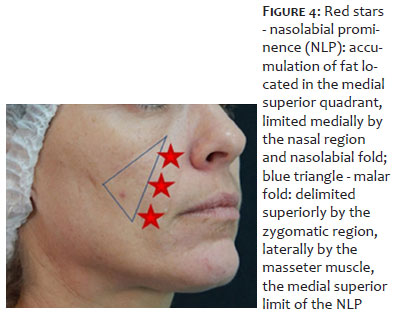
The authors follow their observation based on Maio et al.6 Cheeks in young people are convex and progressively become flat or concave with age. This is due to the loss of bone support (orbital and zygomatic) and the redistribution of mid-facial fat, resulting in an accumulation of fat located in the SM quadrant of the cheeks, which is limited medially by the nasal region and nasolabial fold, which remains unnamed in the bibliography studied, and we therefore suggest the name nasolabial prominence (NLP). This NLP can progressively evolve towards the IM quadrant, forming a projection in the medial region of the mandible, the jowl, which is limited anteriorly by the ML, determining a so-called buccomental crease (Figure 4).
Maio et al. also described the appearance of a triangular area of depression that extends inferolaterally to the lower eyelid for 2 to 3 cm, called the malar furrow, delimited superiorly by the zygomatic region of the malar and laterally by the masseter muscle. The authors suggest using the NLP described in this article as the superomedial limit, which, with the progression of aging, joins the jowl inferomedially, forming a single structure (Figure 4).
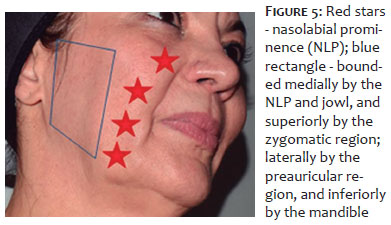
According to the authors, this triangular area can progressively evolve or merge into a rectangular depression due to the depletion of deep fat in the lateral-superior region of the submalar, pre-auricular and masseteric regions, limited medially by the NLP and jowl, superiorly by the zygomatic region, laterally by the pre-auricular region and inferiorly by the mandible (Figure 5).
The authors then refer to these depressed areas as "valleys," and the elevated areas of the face, such as the bony projections, the jowl itself and now the NLP, as "peaks," which should be used as a parameter for leveling the skin surface and repositioning the face, which can be done using various facial volumization techniques and products.
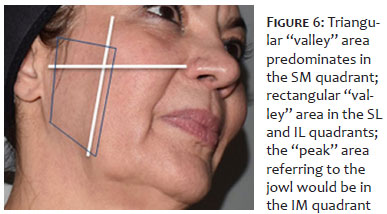
Initially assessing the patient by marking "valleys" and "peaks" and then applying the facial quadrant division, the triangular "valley" area predominates in the SM quadrant and the rectangular "valley" area in the SL and IL quadrants. The "peak" area referring to the jowl would be in the IM quadrant (Figure 6). Therefore, we will start the volumization in the SL and IL quadrants (post-ligament line) for the effect of lifting and correcting the loss of volume, followed by the SM quadrant. On the other hand, the IM quadrant should not be approached during volumization techniques. In this region, it is preferable to use other techniques to reduce volume and to use tissue contraction to reduce sagging.7-9
There is no unique, optimal method for assessing and treating facial aging. Therefore, when we use the areas of volume loss and the areas of projection, we are often able to treat the patient while maintaining their identity and natural appearance, without trying to transform them into someone else using only anthropometric measurements of what would theoretically be an ideal face, which is very subjective and culturally diverse.2
Therefore, facial perception in quadrants, together with the identification of "valleys and peaks," would facilitate diagnosis and a customized treatment plan, with a smaller amount of material, since "peaks" would be avoided when performing facial volumization. l
Giseli Petrone
ORCID: 0000-0003-2853-2001
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis and interpretation; effective participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Marcio Serra
ORCID: 0000-0002-0101-520X
Approval of the final version of the manuscript; critical literature review; critical review of the manuscript.
1. Carruthers J, Flynn TC, Geister TL, Görtelmeyer R, Hardas B, Himmrich, et al. Validated assessment scales for the mid face. Dermatol Surg. 2012;38:320-32.
2. Armengou X, Frank K, Kaye K, Brénant V, Möllhoff N, Cotofana S, et al. Facial anthropometric measurements and principles – overview and implications for aesthetic treatments. Facial Plast Surg. 2023.
3. Casabonas G, Frank K, Koban KC, Freytag DL, Schenck TL, Lachman N, et al. Lifting vs volumizing – the difference in facial minimally invasive procedures when respecting the line of ligaments. J Cosmet Dermatol. 2019;18(5):1237-43.
4. Braz A, Palermo E, Issa MC. Revisiting the ligament line of the face a new understanding for filling the fixed and mobile face. Dermatol Clin. 2024;42(1):97-102.
5. P Nechala, J Mahoney, L Farkas. Comparison of techniques used to locate the malar eminence. Can J Plast Surg 2000;8(1):21-4.
6. Maio M, DeBoule K, Braz A, Rohrich RJ. Facial assessment and injection guide for Botulinum Toxin and injectable Hyaluronic Acid fillers: focus on the midface. Plast Reconstr Surg. 2017;140:540e.
7. Montes JR, Santos E, Chillar A. Jowl jeduction with Deoxycholic Acid. Dermatol Surg. 2020;46(1):78-85.
8. Bellote TPC, Miot HA. Microfocused ultrasound with visualization for face slimming: preliminary results in four women. Clin Cosmet Investig Dermatol. 2021;14:1613-9.
9. Yoon JH, Kim SS, Oh SM, Kim BC, Jung W . Tissue changes over time after polydioxanone thread insertion: an animal study with pigs. J Cosmet Dermatol. 2018;1-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}