


Carlos Roberto Antonio; Lívia Arroyo Tridico
Submitted on: 11/22/2023
Approved on: 02/07/2024
Funding: None.
Conflict of interest: None.
How to cite this article: Antonio CR, Trídico LA. Exosomes in dermatology: A review of their role in skin diseases and rejuvenation. Surg Cosmetic Dermatol. 2024;16:e20240324.
Exosomes are small extracellular vesicles, released by different types of cells, that play roles in intercellular communication. In the skin, exosome-mediated information transfer and intercellular communication are necessary for the maintenance of cellular function and tissue homeostasis. Recently, several studies have demonstrated the involvement of exosomes in skin diseases and rejuvenation, including potential therapeutic uses. In this context, we address recent research on exosomes in dermatology by reviewing the role of exosomes in skin diseases and rejuvenation.
Keywords: Exosomes; Skin; Rejuvenation.
The skin is the physical, chemical, and immune barrier of the human body, preventing loss of substances to the environment. However, it has several other functions, such as tissue repair, perspiration, and temperature and pressure detection, in addition to promoting structural support. The performance of these multiple functions is affected by several factors, ranging from environmental to hormonal. Recent studies have indicated a role of exosomes in physiological and pathological processes of the skin. Their findings have brought a new perspective to understanding the molecular mechanisms involved in these processes.1
Exosomes are small extracellular vesicles, released by different types of cells, that effect intercellular communication through the delivery of bioactive proteins, lipids, RNAs, and DNA from donor cells to recipient cells, being able to both regulate cellular physiological events and participate in pathological processes.2 The recognition of exosomes by cellular targets is specific and involves the following events: recognition between receptor surfaces, direct fusion of the exosome with its target on the cell membrane, and absorption into the target cell by endocytosis. Given their abilities, exosomes are important mediators of intercellular communication and are involved in multiple processes, including immune response, angiogenesis, and inflammation. Cells secrete exosomes as a means of presenting signaling molecules to tissues or to other cells with regulatory functions.3
In the skin, exosome-mediated information transfer and intercellular communication are necessary for the maintenance of cell functions and tissue homeostasis. Studies have shown that transport of endogenous exosomes occurs in multiple types of skin cells and is implicated in the molecular mechanisms of cutaneous diseases.4 Furthermore, the content of exosomes (known as cargo) can be a potent biomarker for the diagnosis and treatment of cutaneous disorders and diseases. Exosomes secreted by stem cells can be used for therapeutic purposes in regenerative and aesthetic medicine.5 Within this context, in the following sections, we will address recent research on exosomes and the skin by reviewing the literature on the interactions of skin exosomes and their roles in skin diseases and rejuvenation.
The first evidence of the existence of extracellular vesicles was recorded in the early 1960s, but little was known on the subject.6 Major discoveries occurred in the late 1980s, when a study on the maturation of sheep reticulocytes revealed the mechanism of exosome formation. These investigators demonstrated that small vesicles were formed within endosomes and then released into the extracellular environment by exocytosis (hence exosomes).7 Years later, a study proposed that exosomes were small transporters carrying mRNA and microRNA that enabled remote genetic communication.8 Developments in exosome research since then have led to a new paradigm in several fields of medicine. Because they are derived from different cells or tissues, exosomes exert multiple actions and may be associated both with physiological cellular functions and with disease states.9
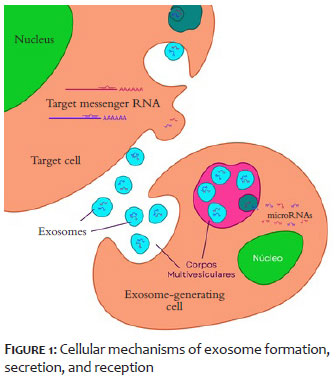
Extracellular vesicles (EVs) play an important role in intercellular communication. They are stratified by size into exosomes (60 to 180 nm in diameter), microvesicles (50 to 1000 nm), or apoptosomes (50 to 5000 nm). Exosomes are secreted by most cells and contain a variety of proteins and nucleotides.10 Damaged organs secrete signals that induce stem cells to produce RNA and protein-containing exosomes, in order to facilitate the maintenance of tissue homeostasis. The composition of exosomes is influenced by inflammatory signals such as lipopolysaccharides, tumor necrosis factor-alpha, interferon gamma, and hypoxia. In addition, other physiological factors and cellular conditions also affect exosome release, such as intracellular calcium levels, cellular energy, membrane phospholipids, membrane-associated enzymes, cytoskeleton-membrane interactions, and other effects of exocytosis, hypoxia, and oxidative stress.11 Exosomes are loaded with bioactive components for intercellular communication and gradually mature as they are delivered to multivesicular bodies by internal budding. This process prevents the cytoplasmic degradation of exosomes by lysosomes. Multivesicular bodies then fuse with the plasma membrane and are secreted into the microenvironment (extracellular space or bodily fluids), carrying RNAs and proteins depending on the type of cell which secreted them.13 The cargo of exosomes consists of biologically active substances, including proteins, mRNA, microRNA, cytokines, and transcription factors. Circulating exosomes are recognized by multiple receptors on cells, which then receive their cargo (Figure 1). Exosome uptake occurs by three mechanisms: endocytosis, ligand-receptor uptake, and fusion.14
The skin, known for being the largest organ in the body, is composed of the epidermis, the dermis, and the subcutaneous tissue. The outermost layer of the skin, the stratum corneum, is 10 to 20 µm thick and consists of 10 to 15 layers of dead cells. The second layer, the viable epidermis, is 100 to 150 µm thick and is composed predominantly of keratinocytes at various stages of differentiation, in addition to melanocytes, Langerhans cells, and several other types of cells.14 The third layer, the dermis, is rich in extracellular matrix (ECM) proteins and growth factors, due to the presence of several fibroblast lineages. The deepest layer, the hypodermis or subcutaneous tissue, is composed of adipocytes, mesenchymal stem cells (MSCs), and connective tissue.15 The different cell types present in the skin layers, including keratinocytes, fibroblasts, and macrophages, have the ability to communicate with the environment and mount complex responses to internal and external stimuli.16 Thus, different types of skin cells secrete exosomes to other cells or bodily fluids in order to participate in biological activities.4
The development of the skin, especially the epidermis, is essential for survival. The balance between cell renewal and differentiation must be regulated by stem and progenitor cells.17 Exosomes are abundantly loaded with epidermal progenitor cells and are essential to preventing premature differentiation of progenitor cells. Wnt signaling pathways play an important role in skin development and renewal processes. In a prior study, Wnt protein transport was found to be mediated by exosomes.18
Skin pigmentation is also regulated by keratinocyte-derived exosomes that carry specific mRNA and bind to melanocytes. In addition, exosomes are capable of affecting angiogenesis, cell proliferation and differentiation, apoptosis, and inflammation.5 Fibroblast-derived exosomes have been shown to increase collagen and elastin synthesis, and may act in rejuvenation and wound-healing processes.19 They have also been implicated in the regulation of skin inflammation, since exosomes from adipose tissue-derived mesenchymal stem cells downregulate the expression of inflammatory cytokines such as IL-4, IL-23, IL-31, and TNF-α. It has also been suggested that exosomes secreted by mesenchymal stem cells can balance the Th1 and Th2 immune responsess.20
Mesenchymal stem cells (MSCs) are multipotent stem cells defined by their ability for self-renewal, multilineage differentiation potential, and paracrine regulation. Due to their ease of isolation, in vitro expansion, and multipotent origin, MSCs have become established as a particularly important stem cell type in the field of regenerative medicine, including tissue repair.21 In addition to their classic origin in the bone marrow, MSCs are also present in adipose tissue, muscle, umbilical cord blood, and various other organs and tissues. Stem cells have excellent therapeutic effects in promoting tissue remodeling, neovascularization, soft-tissue regeneration, bone and cartilage repair, rejuvenation of various tissues, and hair-follicle regeneration. Currently, stem cells are mainly used to facilitate the healing of skin wounds via their multifactorial paracrine effects. However, therapeutic use of stem cells in wound healing is limited by difficulties in storage, potentially tumorigenic mutations, immune rejection, and ethical issues.22
Since exosomes are the products of their parent cells, MSC-derived exosomes (MSC-exos) have unique biological functions similar to those of MSCs. Indeed, stem cell-derived exosomes are essential mediators of the paracrine effects of stem cells.23 MSC-exos also contain cytokines such as vascular endothelial growth factor (VEGF), transforming growth factor β1 (TGF-β1), interleukin-6 (IL-6), interleukin-10 (IL-10), and hepatocyte growth factor (HGF), which facilitate angiogenesis and immunomodulation.24 The main packaging components of MSC-exos, including metabolites, proteins, DNA, and non-coding RNAs (ncRNAs), can be internalized by recipient cells such as fibroblasts, keratin-forming cells, immune cells, and endothelial cells (ECs) and further promote improved tissue repair. Furthermore, the efficacy of repair mediated by MSC-exos can be improved by targeted editing of exosome content, pretreatment of MSCs, or artificial modification of exosome surface receptors.25
In summary, MSC-exos may have specific advantages over MSCs for dermatological applications. Adipose-derived stem cells (AD-MSCs), bone marrow-derived MSCs (BD-MSCs), and human umbilical cord MSCs (hUC-MSCs) are the most frequently used exosome-producing cells. However, MSC-exos have specific mechanisms which make their use a promising cell-free therapeutic strategy for skin regeneration.26
Given the various effects of exosomes in skin cells, we will now address its action on cutaneous diseases and rejuvenation.
Several studies have demonstrated the therapeutic role of exosomes at various stages of wound healing. During the inflammatory phase, exosomes have been shown to modulate immune cells and local tissue cells, helping prevent an uncontrolled inflammatory response. During the proliferation phase, exosomes act to close up the scar by activating endothelial cells and fibroblasts. This activation promotes a proangiogenic milieu and initiates extracellular matrix deposition. Finally, during the remodeling phase, exosomes influence the balance between matrix metalloproteinases and tissue inhibitors of matrix metalloproteinases, which facilitates the achievement of excellent tissue healing. Exosome therapy also increases tissue healing by stabilizing and stimulating a wide variety of mediators involved in each of these phases.27
In a systematic review, Sousa et al. (2023) highlighted the great potential of exosomes as therapeutic options for chronic nonhealing wounds. In summary, exosome therapy has shown consistent positive results, including increased wound closure rates, stimulation of local angiogenesis and re-epithelialization, and increased collagen deposition. Furthermore, exosomes have demonstrated the ability to reduce scar formation, alleviate local inflammation, promote increased formation of granulation tissue, and increase the proliferation and migration of dermal fibroblasts. These findings highlight the therapeutic efficacy of exosomes in promoting wound healing. In the last 5 years, there have also been significant advances in combining exosomes with innovative engineering strategies. Exosome-based therapies have emerged as promising tools for wound healing, with advantages such as abundant sources; ease of preparation, storage and transportation; and minimal immunogenicity.28
Healing is a process that at least partially comes down to an exosome-mediated interaction between various skin cells, including keratinocytes, fibroblasts, endothelial cells, adipocytes, macrophages, and other immune cells. Li et al. suggested that macrophage-derived exosomes are capable of promoting the healing of diabetic wounds, with marked pro-angiogenesis and proliferative effects and attenuating the secretion of cytokines and pro-inflammatory enzymes.29 Kim et al. found that subcutaneous administration of M2 macrophage-derived exosomes (M2-exos) in a mouse wound model markedly decreases and increased the local populations of M1 and M2 macrophages, respectively, thus contributing to a successful conversion of M1 to M2 macrophages.30 Finally, exosome-guided reprogrammed M2 macrophages improved fibroblast migration, collagen deposition, and endothelial cell tube formation in wound healing. Interestingly, exosomes derived from mesoglycan-treated, exosome-containing keratinocytes were able to induce increased expression of vascular endothelial growth factor (VEGF) and fibroblast growth factor (FGF) in human fibroblasts and endothelial cells, thereby increasing angiogenesis and stress fiber formation, in vitro.31 This finding revealed an autocrine loop with a positive impact on re-epithelialization which is implicated in wound healing. Furthermore, Zhao et al. discovered that exosomes derived from human umbilical vein endothelial cells (HUVECs) could accelerate wound healing, both in vitro and in vivo, and promote the proliferation and migration of keratinocytes and fibroblasts, two important types of effector cells for skin regeneration.32
Exosomes play a critical role in the pathogenesis of inflammatory and autoimmune cutaneous diseases. AD-MSCs can exert an important paracrine effect by secreting active soluble factors and exosomes that modulate inflammation and may thus be an option for treating atopic dermatitis. Cho et al. found that injection of ADSC-exos was able to improve atopic dermatitis in mice treated with house dust mite antigens by reducing serum levels of IgE, eosinophils, and pro-inflammatory cytokines such as IL-4, IL-23, IL-31 and TNF-α, thus improve pathological symptoms in AD skin lesions.33 Shin et al. found that, in an oxazolone-induced dermatitis model, subcutaneous injection of ADSC-exos markedly reduced transepidermal water loss, while also improving stratum corneum moisture and markedly decreasing levels of inflammatory cytokines such as IL-4, IL- 5, IL-13, TNF-α, IFN-γ, IL-17 and thymic stromal lymphopoietin (TSLP), indicating that ASC-exos effectively restored the epidermal barrier functions in AD by promoting ceramide synthesis.34
Psoriasis is at least partly attributable to immune system dysfunction; therefore, exosomes can act by modulating the production of pro-psoriatic cytokines. Phospholipase A2 is highly overexpressed in psoriasis. It was recently discovered that mast cells produce exosomes containing phospholipase A2, generating neolipid antigens and leading to recognition by active CD1 cells, which results in the production of interleukins IL-22 and IL-17, involved in the pathogenesis of psoriasis. Cutaneous T cells from patients with psoriasis were found to exhibit increased sensitivity to phospholipase A2 versus control T cells, suggesting that mast cell exosomes are important mediators in the pathogenesis of psoriasis and that inhibition of phospholipase A and CD1 exosomes may be therapeutic strategies in psoriasis.35
As targeted anti-IL-17 and anti-IL-23 therapies have proven effective in psoriasis, it can be assumed that manipulating the function of the exosomes of dendritic cells (which release IL-23, which in turn controls the release of IL-17 and IL-23) 17) may be a promising avenue to treat this common chronic disease. Along these lines, Jiang et al. demonstrated that exosomes isolated from psoriasis-like keratinocytes and treated with a "psoriatic cytokine cocktail" (IL-17A, IL-22 and TNF-α) are critical actors in the induction of psoriatic inflammation, through activation and infiltration of T cells and neutrophils. Increased expression of inflammatory cytokines (IL-6, IL-8 and TNF-α) has been reported after stimulation with keratinocyte-derived exosomes, suggesting that control of these Evs may have therapeutic potential to treat psoriasis.36
Indeed, epidermal keratinocyte-derived exosomes have been found to exacerbate skin lesions in a psoriasis-like mouse model. Keratinocytes interact with infiltrating immune cells (such as neutrophils and mast cells) via exosomes, positively affecting the epidermal microenvironment in psoriasis. Shao et al. found that exosomes secreted by neutrophils harvested from patients with generalized pustular psoriasis could be internalized by keratinocytes and increase the expression of inflammatory molecules in these keratinocytes via activation of signaling pathways, such as IL-1β, IL-36 G, IL-18, and TNF-α.37
It has been demonstrated that IFN-γ can mediate exosome secretion in cells that play a critical role in the pathogenesis of psoriasis, activating innate and adoptive immune cells, such as dendritic cells, lymphocytes, neutrophils, NK cells and macrophages.38 Evidence further suggests that RNAs transported by exosomes play a critical role in regulating inflammatory responses against endotoxin and in several diseases, including psoriatic arthritis. A recent study showed that plasma exosomal microRNAs play a critical role in the pathogenesis of autoimmune diseases, including psoriasis, and can be used as biomarkers of disease or prognosis.39
Exosomes play an important role in anti-skin cancer therapy. Zhao et al. reported that exosomes are critical to 5-aminolevulinic acid photodynamic therapy (ALA-PDT) of cutaneous squamous cell carcinoma (SCC), as they mediate its antitumor action via induction of dendritic cell maturation and TGF-β1 fibroblast secretion, providing a new strategy for antitumor immune response.40 Chang et al. identified clustered exosomes from fibroblasts and keratinocytes in patients with basal cell carcinoma (BCC), demonstrating an increase in proliferation, metabolic activity, migration, and invasion capacity of exosomes in patients with BCC compared to a control group without BCC.41
Merkel cell carcinoma (MCC) is an aggressive cancer, with a poor prognosis, for which biomarkers to allow early detection and assessment of treatment response are lacking. Konstantinell et al. investigated exosomes from four different MCC cell lines and identified 164 common proteins, many of which were involved in tumor progression and metastasis, demonstrating the importance of obtaining information on the protein cargo of exosomes and laying the foundation for identification of exosome proteins that might measured in biopsy specimens as prognostic and diagnostic biomarkers to assess the progression of MCC.42
Recently, the importance of melanoma-derived exosomes in the progression of this cancer has become more evident due to their role in various stages of metastasis, including induction of migration, invasion, primary niche manipulation, immune modulation, and pre-metastatic niche formation. In a review on the role of exosomes in melanoma progression, Isola et al. concluded that tumor-derived exosomes participate as cellular messengers and are involved in several steps that are essential for successful metastasis. Some melanoma exosome-specific proteins found in patients' circulating exosomes are now known to correlate with prognosis; this evidence shows the great potential of using exosomes to detect cancer and estimate prognosis. The field of research into the role of exosomes in cancer progression is expanding and being increasingly explored, as exosomes emerge both as a druggable target and as a tool to deliver anticancer drugs directly to tumors.43
Human keratinocytes release exosomes that modulate pigmentation. Exosomes transport specific RNAs to melanocytes and modulate pigmentation status by altering gene expression and tyrosinase activity. Thus, they can act both to inhibit and to stimulate melanogenesis. Kim et al. showed that keratinocyte exosomes can inhibit melanogenesis by decreasing levels of microphthalmia-associated transcription factor – the main transcriptional regulator of melanogenesis – in melanocytes.44 Lo Cicero et al. found that exosomes from UVB-stimulated keratinocytes increased tyrosinase activity in melanocytes. Furthermore, transfection of melanocytes with keratinocyte-specific pre-mRNAs increases melanin production and microphthalmia-associated transcription factor gene expression. Thus, keratinocyte exosomes have roles in delivering RNA cargo to alter melanocyte pigment production in microphthalmia-associated transcription factor-dependent and microphthalmia-associated transcription factor-independent pathways.5
Takano et al. found that exosomes from UVB-irradiated keratinocytes significantly activated melanocytes, suggesting quantitative changes in exosomes secreted by keratinocytes homeostatically regulate human skin color development.45 Liu et al. also suggested that crosstalk between keratinocytes and melanocytes in the epidermal melanin unit occurs via exosomal mRNAs, reporting that keratinocyte exosomes induced a significant decrease in melanin production and tyrosinase expression in melanocytes.46 Despite this evidence, additional studies of this nature are needed to gain insight into how exosomes can be used to manipulate pigmentation in hypo- and hyperpigmentation disorders.
Circulating exosomes have been shown to be immunologically active and their levels to correlate with disease activity in SLE patients. SLE exosomes mediate increased production of TNF-α, IL-1β, and IL-6, all of which may play a role in the inflammatory process of SLE.47 In a review on the role of exosomes in SLE, Fei et al. reported that exosomes play important roles in the occurrence and development of lupus via several molecular mechanisms that significantly mediate its progression. They further concluded that exosomes have attracted increasing attention from pharmacologists and drug developers as potential drug carriers, as it has been demonstrated that exosomes provide substantial benefits in the targeted delivery of drugs and biomolecules, making them excellent candidates for the treatment of SLE and other autoimmune diseases.48
Exosomes from patients with systemic sclerosis contain mRNAs with a profibrotic profile and induce a profibrotic phenotype in normal fibroblasts in vitro. Wermuth et al. discovered that serum exosomes from systemic sclerosis had profibrotic mRNAs. Exosomes isolated from patients with systemic sclerosis stimulated profibrotic gene expression (type 1 collagen and fibronectin) in human dermal fibroblasts. Thus, exosomes are involved in the pathogenesis of systemic sclerosis and may be a promising therapeutic target.49
Dermal papilla cells (DPCs) play an important role in hair follicle stem cell (HFSC) differentiation. In the resting phase, HFSCs are located in the bulge region of the follicles. During apoptosis of matrix cells, the dermal papilla (DP) migrates upward and, upon reaching the bulge, releases signals that stimulate the differentiation of HFSCs and trigger follicle regeneration.50 Exosomes play an important role in cell-to-cell communication. Research in mice has shown that DPC exosomes (DPC-exos) induce the anagen phase while delaying the catagen phase of hair follicle growth, producing longer hair strands and larger bulges, as well as improve outer root sheath cell proliferation and migration in vitro. These effects were found to be mediated by β-catenin and hedgehog signaling. These findings highlight a novel role for exosomes in regulating hair follicle growth and development and provide a potential avenue for treating hair loss.52
Yan et al. showed that HFSC differentiation could be induced by culturing DPCs with DPC-exos coupled to the surface of the HFSCs. Using high-throughput micro RNA (miRNA) sequencing, 111 miRNAs were identified that were significantly differentially expressed between DPC-exos and DPCs, and the predicted target genes of the top 34 differentially expressed miRNAs suggested that DPC-exos regulate the proliferation and differentiation of HFSCs via genes involved in cellular signal transduction, regulation of fatty acid expression, and cell-to-cell communication.53
A recent study by Wang et al. evaluated the use of DPC-exos in the treatment of male pattern baldness in an animal model. The results showed significant hair regeneration in the group treated with DPC-exos, which probably activated VEGF and AKT1 expression, protecting DPCs and restoring hair growth.54
Skin aging is a complex mechanism that involves intrinsic and extrinsic processes, which manifest clinically as loss of epidermal and dermal thickness, deepening of rhytids, enlargement of pores, depigmentation, and decreased soft-tissue elasticity. This is a multifactorial process, but one key component – the senescence of vitally important cells such as keratinocytes, fibroblasts, and melanocytes – is believed to be mediated by miRNA dysregulation. Consequently, structural and functional changes occur in the extracellular matrix, such as a decrease in the organization and production of collagen, elastin, and proteoglycans, all of which are necessary for the tensile strength, elasticity, and moisture of young skin. Many factors are known to exacerbate aging, including oxidative stress, DNA damage, telomere shortening, miRNA regulation, accumulation of advanced glycation end products, genetic mutations, and inflammation. Exosomes are believed to act mainly on oxidative stress and inflammatory pathways, impacting both the extracellular matrix and collagen.55
The potential therapeutic utility of exosomes has increased interest in the proliferation of fibroblasts and stimulation of their migration. In vitro and in vivo studies with UVB photoaging models showed that exosome treatment protects cells from UVB damage by decreasing proinflammatory mediators such as tumor necrosis factor alpha (TNF-α), while upregulating TGF-β and tissue inhibitor MMP (TIMP).56 These mechanisms lead to the reversal of senescence in fibroblasts, upregulating the production of type I collagen, elastin, and fibronectin, and downregulating expression of type III collagen.57
Guo et al. successfully isolated ADSC-exos and found they were able to attenuate the senescence of human dermal fibroblasts (HDFs) and stimulate HDF migration. In addition, the ADSC-exos increased expression of type I collagen and reduced reactive oxygen species (ROS) and senescence-associated β-galactosidase (SA-β-Gal) activity in HDFs. They further demonstrated that ADSC-exos inhibited expression of senescence-related proteins (p53, p21, and p16). These broad anti-senescence effects of ADSC-exos in HDFs may herald a new cell-free antiaging strategy.58
Oh et al. showed that exosomes derived from human pluripotent stem cells inhibit UVB damage to dermal fibroblasts and overexpression of matrix-degrading enzymes, in addition to restoring the expression of type I collagen in senescent dermal fibroblasts, suggesting therapeutic potential in rejuvenation.56
Recent studies evaluating topical exosomes in conjunction with nonsurgical facial treatments have demonstrated synergistic effects.59,60 Chernoff found that combining topical exosomes with facial microneedling produced greater skin quality, tone, texture, vascularity, clarity, and overall patient satisfaction compared to microneedling alone.59 Duncan added topical exosomes after facial rejuvenation procedures such as laser resurfacing and found faster recovery and fewer side effects compared to resurfacing alone.60
Exosomes play a key role in skin physiology, skin diseases, and rejuvenation. Although research and scientific evidence are still recent, their importance in Dermatology has been consolidated. In this sense, exosomes represent a new perspective that encompasses cellular and molecular mechanisms involved in skin processes and provides the possibility of revolutionary therapies in the near future.
Carlos Roberto Antonio
ORCID: 0000-0001-9243-8293
Approval of the final version of the manuscript; study design and planning; effective participation in research guidance; critical review of the literature; critical review of the manuscript.
Lívia Arroyo Tridico
ORCID: 0000-0002-7743-4195
Preparation and writing of the manuscript; collecting, analyzing, and interpreting data; critical review of literature; critical review of the manuscript.
1. Liu Y, Wang H, Wang J. Exosomes as a novel pathway for regulating development and diseases of the skin. Biomed Rep. 2018;8(3):207-14
2. Raposo G, Stoorvogel W. Extracellular vesicles: exosomes, microvesicles, and friends. J. Cell Biol.2013;200:373–83.
3. Bach DH, Hong JY, Park HJ, Lee SK. The role of exosomes and miRNAs in drug-resistance of cancer cells. Int J Cancer. 2017;141:220–30.
4. Wang WM, Wu C, Jin HZ. Exosomes in chronic inflammatory skin diseases and skin tumors. Exp Dermatol.2019;28(3):213-8.
5. Lo Cicero A, Delevoye C, Gilles-Marsens F, Loew D, Dingil F, Guéré C, et al. Exosomes released by keratinocytes modulate melanocyte pigmentation. Nat Commun.2015;6:7506.
6. Bonucci E. Fine structure of early cartilage calcification. J Ultrastruct Res. 1967;20(1):33–50.
7. Pan BT, Teng K, Wu C, Adam M, Johnstone RM. Electron microscopic evidence for externalization of the transferrin receptor in vesicular form in sheep reticulocytes. J Cell Biol. 1985;101(3):942–8.
8. Valadi H, Ekström K, Bossios A, Sjöstrand M, Lee JJ, Lötvall JO. Exosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat Cell Biol. 2007;9(6):654–9.
9. Zhou H, Cheruvanky A, Hu X, Matsumoto T, Hiramatsu N, Cho ME, et al. Urinary exosomal transcription factors, a new class of biomarkers for renal disease. Kidney Int. 2008;74(5):613–21.
10. Barile L, Moccetti T, Marban E, Vassalli G. Roles of exosomes in cardio protection. Eur Heart J. 2017;38(18):1372–9.
11. Turturici G, Tinnirello R, Sconzo G, Geraci F. Extracellular membrane vesicles as a mechanism of cell-to-cell communication: advantages and disadvantages. Am J Physiol. Cell Physiol. 2014;306:C621–C633.
12. Rashed MH, Bayraktar E, Helal GK, Abd-Ellah MF, Amero P, Chavez-Reyes A, et al. Exosomes: from garbage bins to promising therapeutic targets. Int J Mol. Sci. 2017;18(3):538.
13. Fitzner D, Schnaars M, Van Rossum D, Krishnamoorthy G, Dibaj P, Bakhti M, et al. Selective transfer of exosomes from oligodendrocytes to microglia by macropinocytosis. J Cell Sci. 2011;124(Pt 3):447– 58.
14. Gaur M, Dobke M, Lunyak VV. Mesenchymal stem cells from adipose tissue in clinical applications for dermatological indications and skin aging. Int J Mol Sci. 2017;18(1):208.
15. Cole MA, Quan T, Voorhees JJ, Fisher GJ. Extracellular matrix regulation of fibroblast function: redefining our perspective on skin aging. J Cell Commun Signal.2018;12(1):35-43.
16. Xiong M, Zhang Q, Hu W, Zhao C, Lv W, Yi Y, et al. The novel mechanisms and applications of exosomes in dermatology and cutaneous medical aesthetics. Pharmacol Res. 2021;166:105490.
17. Mistry DS, Chen Y, Sen GL. Progenitor function in self-renewing human epidermis is maintained by the exosome. Cell Stem Cell. 2012;11:127–35.
18. Gross JC, Chaudhary V, Bartscherer K, Boutros M. Active Wnt proteins are secreted on exosomes. Nat Cell Biol. 2012;14:1036–45.
19. Hu S, Li Z, Cores J, Huang K, Su T, Dinh P-U, et al. Needle-free injection of exosomes derived from human dermal fibroblast spheroids ameliorates skin photoaging. ACS Nano. 2019;13(10):11273–82.
20. Cho BS, Kim JO, Ha DH, Yi YW. Exosomes derived from human adipose tissue- derived mesenchymal stem cells alleviate atopic dermatitis. Stem Cell Res Ther. 2018;9(1):187.
21. Hoang DM, Pham PT, Bach TQ, Ngo ATL, Nguyen QT, Phan TTK, et al. Stem cell- based therapy for human diseases. Signal Transduct Target Ther. 2022;7:272.
22. Mazini L, Rochette L, Admou B, Amal S, Malka G. Hopes and limits of adipose- derived stem cells (ADSCs) and mesenchymal stem cells (MSCs) in wound healing. Int J Mol Sci. 2020;21:1306.
23. Ha DH, Kim HK, Lee J, Kwon HH, Park GH, Yang SH, et al. Mesenchymal stem/stromal cell-derived exosomes for immunomodulatory therapeutics and skin regeneration. Cells. 2020;9:1157.
24. An Y, Lin S, Tan X, Zhu S, Nie F, Zhen Y, et al. Exosomes from adipose-derived stem cells and application to skin wound healing. Cell Prolif. 2021;54:e12993.
25. Tutuianu R, Rosca AM, Iacomi DM, Simionescu M, Titorencu I. Human mesenchymal stromal cell-derived exosomes promote in vitro wound healing by modulating the biological properties of skin keratinocytes and fibroblasts and stimulating angiogenesis. Int J Mol Sci. 2021;22:6239.
26. Zhou C, Zhang B, Yang Y, Jiang Q, Li T, Gong J, et al. Stem cell-derived exosomes: emerging therapeutic opportunities for wound healing. Stem Cell Res Ther. 2023;14(1):107.
27. Prasai A, Jay JW, Jupiter D, Wolf SE, El Ayadi A. Role of exosomes in dermal wound healing: a systematic review. J Investig Dermatol.2022;142:662– 678.e8.
28. Sousa P, Lopes B, Sousa AC, Moreira A, Coelho A, Alvites R, et al. Advancements and insights in exosome-based therapies for wound healing: a comprehensive systematic review (2018-June 2023). Biomedicines. 2023;11(8):2099.
29. Mengdie Li, Tao Wang, He Tian, Guohua Wei, Liang Zhao, Shi Y. Macrophage-derived exosomes accelerate wound healing through their anti- inflammation effects in a diabetic rat model. Artif Cells Nanomed Biotechnol. 2019;47(1): 3793-803.
30. Kim H, Wang SY, Kwak G, Yang Y, Kwon IC, Kim SH. Exosome-guided phenotypic switch of M1 to M2 macrophages for cutaneous wound healing. Adv Sci (Weinh). 2019;6(20):1900513.
31. 31. Belvedere R, Pessolano E, Porta A, Tosco A, Parente L, Petrella F, et al. Mesoglycan induces the secretion of microvesicles by keratinocytes able to activate human fibroblasts and endothelial cells: a novel mechanism in skin wound healing. Eur J Pharmacol. 2020;869:172894.
32. Zhao D, Yu Z, Li Y, Wang Y, Li Q, Han D. GelMA combined with sustained release of HUVECs derived exosomes for promoting cutaneous wound healing and facilitating skin regeneration. J Mol Histol. 2020;51(3):251-63.
33. Cho BS, Kim JO, Ha DH, Yi YW. Exosomes derived from human adipose tissue-derived mesenchymal stem cells alleviate atopic dermatitis. Stem Cell Res Ther. 2018;9(1):187.
34. Shin KO, Ha DH, Kim JO, Crumrine DA, Meyer JM, Wakefield JS, et al. Exosomes from human adipose tissue-derived mesenchymal stem cells promote epidermal barrier repair by inducing de novo synthesis of ceramides in atopic dermatitis. Cells. 2020;9(3):680.
35. Cheung KL, Jarrett R, Subramaniam S, Salimi M, Gutowska-Owsiak D, Chen YL, et al. Psoriatic T cells recognize neolipid antigens generated by mast cell phospholipase delivered by exosomes and presented by CD1a. J Exp Med. 2016;213(11):2399-412.
36. Jiang M, Fang H, Shao S, Dang E, Zhang J, Qiao P, et al. Keratinocyte exosomes activate neutrophils and enhance skin inflammation in psoriasis. FASEB J. 2019;33(12):13241-53.
37. Shao S, Fang H, Zhang J, Jiang M, Xue K, Ma J, et al. Neutrophil exosomes enhance the skin autoinflammation in generalized pustular psoriasis via activating keratinocytes. FASEB J. 2019;33(6):6813-28.
38. Zhou W, Hu M, Zang X, Liu Q, Du J, Hu J, et al. Luteolin attenuates imiquimod-induced psoriasis-like skin lesions in BALB/c mice via suppression of inflammation response. Biomed Pharmacother. 2020;131:110696.
39. Alexander M, Hu R, Runtsch MC, Kagele DA, Mosbruger TL, Tolmachova T, et al. Exosome-delivered microRNAs modulate the inflammatory response to endotoxin. Nat Commun. 2015;6:7321.
40. Zhao Z, Zhang H, Zeng Q, Wang P, Zhang G, Ji J, et al. Exosomes from 5-aminolevulinic acid photodynamic therapy-treated squamous carcinoma cells promote dendritic cell maturation. Photodiagnosis Photodyn Ther.2020;30:101746.
41. Chang J, Tran DC, Zhu GA, Li R, Whitson R, Kim YH, et al. Initial in vitro functional characterization of serum exosomal microRNAs from patients with metastatic basal cell carcinoma. Br J Dermatol.2017;177(5): e187-90.
42. Konstantinell A, Bruun JA, Olsen R, Aspar A, Škalko-Basnet N, Sveinbjørnsson B, et al. Secretomic analysis of extracellular vesicles originating from polyomavirus-negative and polyomavirus-positive Merkel cell carcinoma cell lines. Proteomics. 2016;16(19):2587-91.
43. Isola AL, Eddy K, Chen S. Biology, therapy and implications of tumor exosomes in the progression of melanoma. Cancers (Basel). 2016;8(12):110.
44. Kim NH, Choi SH, Kim CH, Lee CH, Lee TR, Lee AY. Reduced MiR-675 in exosome in H19 RNA-related melanogenesis via MITF as a direct target. J Invest Dermatol. 2014;134(4):1075-82.
45. Takano K, Hachiya A, Murase D, Tanabe H, Kasamatsu S, Takahashi Y, et al. Quantitative changes in the secretion of exosomes from keratinocytes homeostatically regulate skin pigmentation in a paracrine manner. J Dermatol. 2020;47(3):265–76.
46. Liu Y, Xue L, Gao H, Chang L, Yu X, Zhu Z, et al. Exosomal miRNA derived from keratinocytes regulates pigmentation in melanocytes. J Dermatol Sci.2019;93(3):159–67.
47. Kusaoi M, Yamaji K, Ishibe Y, Murayama G, Nemoto T, Sekiya F, et al. Separation of circulating microRNAs using apheresis in patients with systemic lupus erythematosus. Ther Apher Dial. 2016;20(4):348-53.
48. Fei Y, Liu Q, Peng N, Yang G, Shen Z, Hong P, et al. Exosomes as crucial players in pathogenesis of systemic lupus erythematosus. J Immunol Res. 2022;2022:8286498.
49. Wermuth PJ, Piera-Velazquez S, Jimenez SA. Exosomes isolated from serum of systemic sclerosis patients display alterations in their content of profibrotic and antifibrotic microRNA and induce a profibrotic phenotype in cultured normal dermal fibroblasts. Clin Exp Rheumatol. 2017;35 Suppl 106(4):21-30.
50. Organ BA. The dermal papilla: an instructive niche for epithelial stem and progenitor cells in development and regeneration of the hair follicle. Cold Spring Harb Perspect Med. 2014;4(7):a015180–a015180.
51. Yan H, Gao Y, Ding Q, Liu J, Li Y, Jin M, et al. Exosomal micro RNAs derived from dermal papilla cells mediate hair follicle stem cell proliferation and differentiation. Int J Biol Sci. 2019;15(7):1368-82.
52. Zhou L, Wang H, Jing J, Yu L, Wu X, Lu Z. Regulation of hair follicle development by exosomes derived from dermal papilla cells. Biochem Biophys Res Commun. 2018;500(2):325-32.
53. Yan H, Gao Y, Ding Q, Liu J, Li Y, Jin M, et al. Exosomal Micro RNAs derived from dermal papilla cells mediate hair follicle stem cell proliferation and differentiation. Int J Biol Sci. 2019;15(7):1368-82.
54. Wang G, Wang Z, Zhang J, Shen Y, Hou X, Su L, et al. Treatment of androgenetic alopecia by exosomes secreted from hair papilla cells and the intervention effect of LTF. J Cosmet Dermatol. 2023;22(11):2996- 3007.
55. Zhang S, Duan E. Fighting against skin aging: the way from bench to bedside. Cell Transplant. 2018;27:729–38.
56. Oh M, Lee J, Kim YJ, Rhee WJ, Park JH. Exosomes derived from human induced pluripotent stem cells ameliorate the aging of skin fibroblasts. Int J Mol Sci. 2018;19(6):1715.
57. Liang JX, Liao X, Li SH, Jiang X, Li ZH, Wu YD, et al. Antiaging properties of exosomes from adipose-derived mesenchymal stem cells in photoaged rat skin. Biomed Res Int. 2020;2020:6406395.
58. Guo JA, Yu PJ, Yang DQ, Chen W. The antisenescence effect of exosomes from human adipose-derived stem cells on skin fibroblasts. Biomed Res Int. 2022;2022:1034316.
59. Chernoff G. The utilization of human placental mesenchymal stem cell derived exosomes in aging skin: an investigational pilot study. J Surg. 2021;6(5):1388.
60. Duncan DI. Combining PDO threads with exosomes for microlifting. Cosmetic Surgery. IntechOpen. 2020.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}