


Frederico França Rezende; Isadora Vilaça Carvalho; Luisa Murakami de Assis; Raquel Keller
Submitted on: 28/07/2023
Approved on: 07/01/2024
Financial support: None.
Conflict of interest: None.
How to cite this article: Rezende FF, Carvalho IV, Assis LM, Keller R. Hypersensitivity reaction to hyaluronic acid dermal filler concomitant with coronavirus infection - case report. Surg Cosmet Dermatol. 2024;16:e20240286.
The incidence of hypersensitivity reactions to dermal fillers with hyaluronic acid is between 0.3 and 4.5% being mediated by T lymphocyte. Influenza-like illnesses can trigger immunological reactions at the site of the filler. The authors report a case of a patient who presented a hypersensitivity reaction to the filler concomitant with a SARS-COV-2 infection. With the large-scale growth of procedures with fillers, there has been an increase in allergic reactions, making their identification essential for adequate treatment, minimizing the deleterious consequences to the patient.
Keywords: Hypersensitivity; Hyaluronic Acid; Coronavirus.
In 2019 there was a 15.7% growth in the number of procedures performed with dermal filler, hyaluronic acid (HA), compared to the previous year. The increase in the number of cases of patients with COVID-19, who presented adverse events resulting from the application of hyaluronic acid, drew the attention of the international scientific community to an alarming trend of the amplification of hypersensitivity reactions 1,2. Adverse effects of treatments with fillers are often classified into two types, depending on the onset of symptoms. Type 1 hypersensitivity reactions are IgE-mediated, occur minutes to hours after the procedure, and may result in clinical pictures of angioedema and anaphylaxis. Delayed-type hypersensitivity reactions are rare, occurring between 24 hours to weeks or months after the process. These reactions are T-lymphocyte mediated and present clinically with a picture of edema, erythema, and local pain 4.
The exact mechanism of late-onset reactions is not fully understood. However, factors such as infection, filler properties, trauma, injection technique, and influenza-like illnesses contribute to the increased incidence, triggering activation of the immune system against the injected product 5.
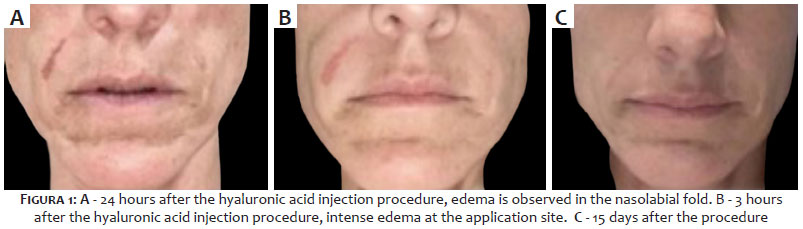
A 47-year-old woman underwent a procedure with hyaluronic acid (Juvederm Ultra Plus XC with lidocaine - Allergan) to fill the nasolabial fold. We perform the approach using a 27G 1/2 needle without any intercurrence. After 24 hours, the patient started presenting intense edema at the application site, mild pruritus, and local pain. Treatment with prednisone 40 mg and loratadine 10 mg was initiated, with regression of the edema a few hours later. On the third day after the procedure, the patient presented flu-like symptoms. The corticosteroid was then suspended due to the hypothesis of coronavirus infection, and the antihistamine was maintained.
The patient performed a self-test, which was positive for COVID-19. The respiratory symptoms were mild, presenting with coryza and cough, which improved after ten days. Loratadine was maintained for seven days. On the 15th day after the filling, the patient was examined, did not presenting anyedema at the site, and was satisfied with the result of the filling in the nasolabial fold. As per the patient's personal history, she had never had a procedure with hyaluronic acid and presented an urticarial picture after the ingestion of contrast in an exam performed three years ago (Figure 1).
The exact pathophysiological mechanism of late-type hypersensitivity reactions, which occur after the filling, is not fully understood. However, it is believed that the triggering of these reactions may be related to the pattern of the patient's immune response to an infectious condition, similar to what occurs with the influenza virus, but in this case, SARS-COV-2. This response is initiated by the activation of T lymphocytes via CD44 and mediated by CD4+ cells associated with macrophage memory consolidation.2,6
Hyaluronic acid (HA) is a naturally occurring, non-sulfated glycosaminoglycan with a high molecular weight of 4,000 to 20,000,000 daltons. Its structure consists of polyanionic disaccharide units of glucuronic acid and N-acetylglucosamine connected by alternating b1-3 and b1-4 bonds. It is a linear polysaccharide of the extracellular matrix of connective tissue, synovial fluid, embryonic mesenchyme, vitreous humor, skin, and many other organs and tissues. HA has essential immunological functions, acting as the major ligand for CD44, a glycoprotein expressed in mammalian cells involved in lymphocyte recruitment and targeting.2 HA occupies several roles in cell signaling, depending on its molecular weight. High molecular weight (HMW) HA is known to have anti-inflammatory effects, while low molecular weight (LMW) HA, less than 500 kDa, is pro-inflammatory. LMW HA activates dendritic cells and macrophages, providing stimulatory co-signals to T cells via CD44 cell surface receptors that alter HA production or degradation via synthetases or hyaluronidase, respectively.3
Dermal fillers with hyaluronic acid can introduce two types of LMW HA: during product degradation and as cross-linking agents. Beleznay et al. (2015) suggested that systemic inflammatory responses, similar to those occurring in flu-like conditions, may trigger accelerated degradation of the HA dermal filler due to free radical production, resulting in LMW HA fragments leading to prolonged irregular CD44-HA signaling, thus resembling the pathophysiology described in the reported case.
Another consequence of LMW HA production is the recruitment of lymphocytes to the filling site where there is the highest concentration of HA. Therefore, HA dermal filler is a risk factor in the development of hypersensitivity reactions in the presence of systemic infection, and this is the likely cause of edema in HA dermal filler after SARS-COV2 infection. Without modification, the half-life of HA in tissues is 24-48 hours, making it unsuitable as a dermal filler. Cross-linking agents are used to produce a viscoelastic, stable gel for cosmetic use to overcome this, the exact technology of which often remains undisclosed by dermal filler manufacturers. It is believed that these cross-linking agents can also activate the immune system.7 Bitterman-Deutsch et al. (2015)9 report that glycosaminoglycans such as HA can act as a superantigen and directly trigger an immune response, unlike the other theories that suggest the degradation of HA into low molecular weight fragments resulting in molecules with pro-inflammatory activity.
Turkmani et al. (2019)6 highlight that influenza infection or the use of medications such as antibiotics, non-steroidal anti-inflammatory drugs, and antipyretics, counteracting infectious agents, could instigate delayed hypersensitivity reactions by activation of lymphocytes through CD4+ cells.
Injection of HA fillers causes erythema, edema, bruising, pain, and itching due to disruptions in the vasculature and dermal structures, as well as excessive water retention due to the hydrophilic nature of HA.
A mild inflammatory reaction is normal, characterized by infiltration of resident macrophages and activation of fibroblasts leading to collagen production that anchors the gel to the tissue. These events usually resolve within a few days. However, with the exponential increase in the use of fillers, it has been shown that HA compounds can trigger acute local hypersensitivity reactions early and late, with the overall incidence rate being 0.8%. More recently, the incidence of late-onset nodules using fillers with VYcross technology has been reported, ranging from 0.5% to 4.25%. Rohrich et al. (2007)3 proposed the most relevant classifications of these hypersensitivity reactions, suggesting that complications should be named as early, late, and delayed (less than 14 days, 14 days to one year, and more than one year, respectively). However, this classification encompasses all types of adverse effects and fillers, and with time, the need for new algorithms emerged. Mikkilineni et al. (2020)4 proposed a new classification scheme that correlates the timing of the inflammatory process for hyaluronic acid only. During the inflammatory process, neutrophils and monocytes are predominant during the first week. Then, between the first and fourth week, the inflammatory response is mild, and the monocytes differentiate into macrophages that activate and interact with T lymphocytes, most of them CD4+ and, to a lesser extent, CD8+ and B lymphocytes, followed by macrophages that engulf particles of the injected material. Subsequently, macrophage-dependent fibroblast infiltration leads to chronic perpetuation and collagen deposition. Thus, adverse hypersensitivity events can be early (up to one week), intermediate (one week to one month), and late (one month to years).9,10 Determining the exact cause of the pathophysiology of the SARS-COV-2 virus with the hypersensitivity process requires further investigation. Several hypotheses collectively determine a broad combination of immunoregulatory properties of HA associated with susceptible host genetic background. Other factors, such as depolymerization of high molecular weight fragments to low molecular weight fragments by enzymatic degradation, cause biological effects that induce immune activation in a local microenvironment depending on host genetics in the case.10
With the increasing use of filler treatments, the incidence of hypersensitivity reactions will consequently increase as well. Recognizing, classifying, and treating hypersensitivity reactions is fundamental, requiring the physician to have an accurate pathophysiological and biochemical understanding of this procedure. Thus, he can identify the patient's predisposition to hypersensitivity reactions by recording the clinical history, preventing and promoting the best prognosis. Improving the infiltration technique and early recognition of complications, as well as mastering the management, are essential for all who perform the procedure, thus reducing the deleterious consequences for the patient.
Frederico França Rezende
ORCID: 0009-0001-7882-825X
Statistical analysis; Study design and planning; Preparation and writing of the manuscript; Collecting, analyzing, and interpreting data; Effective participation in research orientation; Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; Critical literature review; Critical review of the manuscript.
Isadora Vilaça Carvalho
ORCID: 0009-0007-3056-1211
Approval of the final version of the manuscript; Study design and planning; Preparation and writing of the manuscript; Collecting, analyzing, and interpreting data; Effective participation in research orientation; Critical literature review; Critical review of the manuscript.
Luisa Murakami de Assis
ORCID: 0009-0004-1397-5867
Author's contribution: Approval of the final version of the manuscript; Study design and planning; Preparation and writing of the manuscript; Collecting, analyzing, and interpreting data; Effective participation in research orientation; Critical literature review; Critical review of the manuscript.
Raquel Keller
ORCID: 0009-0003-0808-1896
Statistical analysis; Approval of the final version of the manuscript; Study design and planning; Preparation and writing of the manuscript; Collecting, analyzing, and interpreting data; Effective participation in research orientation; Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; Critical literature review; Critical review of the manuscript.
1. Kokoska RE, Lima AM, Kingsley MM. Review of late reactions to 15 hyaluronic acid fillers. Dermatol Surg. 2022;48(7):752-757.
2. RowlandWarmann MJ. Hypersensitivity reaction to hyaluronic acid dermal fillers after infection with the novel coronavirus-a case report. J Cosmet Dermatol. 2021;20(5):1557-1562.
3. Rohrich RJ, Ghavami A, Crosby MA. The role of hyaluronic acid fillers (Restylane) in facial cosmetic surgery: review and technical considerations. Plast Reconstr Surg. 2007;120(6 Suppl):41S-54S.
4. Mikkilineni R, Wipf A, Farah R, Sadick N. New classification scheme for hypersensitivity adverse effects after hyaluronic acid injections: pathophysiology, treatment algorithm, and prevention. Dermatol Surg. 2020;46(11):1404-1409.
5. Decates T, Kadouch J, Velthuis P, Rustemeyer T. Hypersensitivity of the immediate or late type has changed a role in late physiological reactions after hyaluronic acid filler injections. Clin Cosmet Investig Dermatol. 2021;14:581-589.
6. Turkmani MG, De Boulle K, Philipp-Dormston WG. Delayed hypersensitivity reaction to hyaluronic acid dermal fillers after influenza-like illness. Clin Cosmet Investig Dermatol. 2019;12:277-283.
7. Beleznay K, Carruthers JDA, Carruthers A, Mummert ME, Humphrey S. Delayed-onset nodules secondary to a smooth cohesive 20 mg/mL hyaluronic acid filler: cause and management. Dermatol Surg. 2015;41(8):929-939.
8. Bhojani-Lynch T. Late onset inflammatory response to hyaluronic acid dermal fillers. Plast Reconstr Surg Glob Open. 2017;5(12):e1532.
9. Bitterman-Deutsch O, Kogan L, Nasser F. Delayed immune-mediated adverse effects to hyaluronic acid fillers: report of five cases and review of the literature. Dermatol Rep. 2015;7(1):5851.
10. Ofir A, Loizides C, Landau M. Resistant and recurrent late reaction to hyaluronic acid-based gel. Dermatol Surg. 2016;42(1):31-37.
11. Rohrich RJ, Ghavami A, Crosby MA. The role of hyaluronic acid fillers (Restylane) in facial cosmetic surgery: review and technical considerations. Plast Reconstr Surg. 2007;120(6 Suppl):41S-54S.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}