


Laura Boldrin Cardoso de Souza1; Aline da Luz Sousa1; Luís Henrique Barbizan de Moura1; Milvia Maria Simões e Silva Enokihara2; Samira Yarak1
Submitted on: 10/22/2023
Approved on: 01/16/2024.
Financial support: None.
Conflict of interest: None.
How to cite this article: Souza LBC, Sousa AL, Moura LHB, Enokihara MMSS, Yarak S. Schwannoma of the upper lip in an adolescent: report of a rare case. Surg Cosmet Dermatol. 2024;16:e20240313.
Schwannomas are benign nerve sheath tumors derived from Schwann cells. The sites most often involved are the head and neck (25-48%), with only 1% occurring in the oral cavity. Most schwannomas occur in adult individuals between the third and fifth decades of life. Lip involvement is extremely rare during childhood and adolescence, with few reports in the literature. The prognosis is favorable and surgical excision is the treatment of choice. We report an interesting case of upper lip schwannoma in an adolescent with successful surgical treatment and no evidence of recurrence after 4 years.
Keywords: Neurilemmoma; Lip; Neoplasms; Schwann Cells.
Schwannoma or neurilemmoma is a benign neoplasm that arises from Schwann cells in the sheath of peripheral or cranial nerves. The vestibulocochlear nerve is most commonly involved, but any myelinated nerve fiber can be affected, with the exception of the olfactory and optic nerves.1
The etiology of these tumors is not fully understood. Evidence suggests that tumor transformation of Schwann cells is caused by loss-of-function mutations of the NF2 tumor suppressor gene and suggests that these tumors have a predilection for locations prone to neural injury due to compression or physical trauma.2 Approximately 25-48% of schwannomas occur in the head and neck region. Schwannomas account for just over 1% of benign tumors reported in the oral cavity, with the tongue being the most common site.3 These tumors only rarely appear on the lips, with few cases reported in the literature.3
As a rule, schwannoma is a solitary tumor, only occasionally presenting as multiple lesions. Clinically, it appears as an encapsulated, slow-growing nodule.4 When small, most schwannomas are asymptomatic, but pain, whether localized to the tumor or radiating along the nerve of origin, may be present.5 Differential diagnoses of schwannoma in the oral region include neurofibroma, granular cell tumor, fibroma, leiomyoma, hemangioma, lymphangioma, lipoma, pyogenic granuloma, and benign salivary gland tumors.1 Excisional biopsy and histopathological examination are indicated to establish the diagnosis.4 Histologically, in addition to the classic schwannoma, there are cellular, epithelioid, glandular, and plexiform variants.5
Conservative surgical excision is the approach of choice, with a favorable prognosis and low recurrence rates as long as complete removal of the tumor is achieved.6 Malignant transformation is rare, and wide margins are not recommended.4 In this report, we present a case of classic schwannoma in an unusual location and age range.
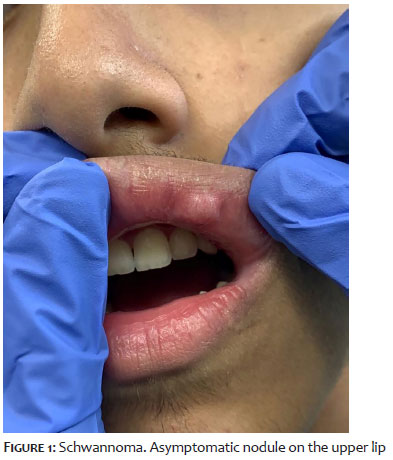
A 16-year-old male presented with a painless nodule on his upper lip that had been growing slowly for 2 years. Dermatological examination revealed a fibroelastic nodule of the same color as the adjacent mucosa, 1.5 × 1.0 cm in size (Figure 1). There was no cervical lymphadenopathy. The patient’s past medical history was notable for sporadic local trauma.
Despite the likely benign nature of the lesion and absence of local pain, the patient and his legal guardians were anxious to obtain a definitive diagnosis. It was therefore decided to excise the lesion. An infraorbital nerve block was performed and a longitudinal incision was made over the lesion, which was then enucleated. The surrounding nervous structure, motor function and local sensitivity were preserved intact (Figure 2).
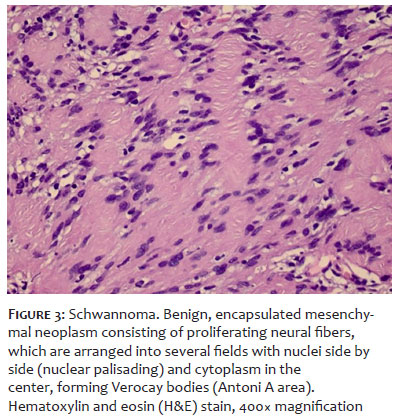
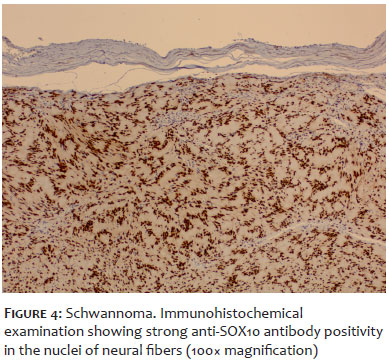
Histopathological examination revealed an encapsulated schwannoma, exhibiting the classic Antoni A (with Verocay bodies) and Antoni B areas (Figure 3). There was no evidence of mitosis or necrosis. Immunohistochemical examination showed a positive reaction to anti-SOX10 antibody in the nuclei of neural fibers (Figure 4).
No recurrence has been observed over 4 years of follow-up. Furthermore, a good cosmetic outcome was obtained without compromising local function or sensitivity.
Schwannomas are benign, slow-growing, encapsulated, generally solitary tumors. Although the etiology of neurilemmomas remains unknown, these lesions are believed to originate as a result of proliferating Schwann cells, which can compress and displace the surrounding nerve.7
The majority of reported cases occur in the head and neck. Although the oral region is highly innervated, only 1% of these tumors arise from peripheral nerves in the oral cavity.4 The upper lip is one of the least likely sites, with very few documented cases.1 Neurilemmomas may occur at any age but are most common between the third and fourth decades of life; in contrast, our patient was much younger. The diagnosis of schwannoma is based on its histological features.8 In this case, the histological presentation was characteristic and easily distinguishable from that of other lesions composed of spindle cells, such as neurofibroma or leiomyoma. The features of the tumor reported herein meet all histological criteria for a classic schwannoma. Typically, Antoni A type tissue is observed, which consists of spindle cells aligned in a characteristic “nuclear palisade” arrangement. Between two neighboring palisades are small eosinophilic masses known as Verocay bodies, formed by a combination of Schwann-cell cytoplasm and associated reticular fibers. Antoni B areas comprise a smaller number of spindle cells arranged randomly within a loose myxomatous stroma.5 The nuclear palisade distribution typical of a schwannoma8 was easily identifiable in this case.
Complementary immunohistochemical analysis showed diffuse anti-SOX10 antibody positive in the nuclei of nerve fibers. The most commonly used immunohistochemical markers for the diagnosis of schwannoma are currently S100 and SOX10.9
The prognosis in schwannoma is favorable. Conservative surgical excision is facilitated by the capsule, which provides a safe natural plane of dissection. As a rule, there is no recurrence after complete excision.6 If the lesion does recur, one must consider whether complete enucleation was indeed achieved or whether malignant transformation has occurred. Malignant transformation is exceedingly rare overall, but is significantly more common in lip schwannomas than in those occurring elsewhere (9.47% versus 0.001%).4
Despite their rarity, schwannomas should be considered in the differential diagnosis of labial nodules due to the abundant innervation of the lip.1 Early diagnosis of these lesions while they are still small increases the odds of a successful surgical outcome, as resection can be particularly complex due to the extensive network of nerves that supply the lips.4 This patient had an excellent postoperative course, with no evidence of recurrence and no sensory impairment at 4 years of follow-up.
Although schwannomas of the upper lip are extremely rare, this diagnosis should be contemplated by dermatologists when evaluating lesions on the lips. Awareness of the histological and immunohistochemical hallmarks of schwannoma is essential to prevent diagnostic error and ensure a satisfactory surgical outcome. Enucleation is an appropriate technique for resection of these encapsulated tumors in the lip region, as it produces a cosmetically acceptable scar while preserving peripheral nerve integrity.
Laura Boldrin Cardoso de Souza
ORCID: 0000-0003-4709-3227
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; critical review of the literature; critical review of the manuscript.
Aline da Luz Sousa
ORCID: 0000-0003-1720-2525
Approval of the final version of the manuscript; study design and planning; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript.
Luís Henrique Barbizan de Moura
ORCID: 0000-0002-5714-8386
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript.
Milvia Maria Simões e Silva Enokihara
ORCID: 0000-0002-3340-4074
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript.
Samira Yarak
ORCID: 0000-0002-5657-6645
Approval of the final version of the manuscript; study design and planning; effective participation in research guidance; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript.
1. Phulware RH, Sardana R, Chauhan DS, Ahuja A, Bhardwaj M. Extracranial Schwannomas of the head and neck: a literature review and audit of diagnosed cases over a period of eight years. Head Neck Pathol. 2022;16(3):707-715.
2. Helbing DL, Schulz A, Morrison H. Pathomechanisms in Schwannoma development and progression. Oncogene. 2020;39(32):5421-5429.
3. Bhola N, Jadhav A, Borle R, Khemka G, Bhutekar U, Kumar S. Schwannoma of the tongue in a pediatric patient: a case report and 20-year review. Case Rep Dent. 2014;780762.
4. Sitenga J, Aird G, Vaudreuil A, Huerter CJ. Clinical features and management of Schwannoma affecting the upper and lower lips. Int J Dermatol.201857(9):1047-1052.
5. Lever WF, Elder DE. Lever’s histopathology of the skin. 10th ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins, Cop; 2009.
6. Yaghoobi R, Pazyar N. Lower lip plexiform schwannoma: report of a rare case and a literature review. Indian J Dermatol.2019;64:407-410.
7. Shim S, Myong H: Neurilemmoma in the floor of the mouth: a case report. J Korean Assoc Oral Maxillofac Surg. 2016;42:60-64.
8. Yang SW, Lin CY. Schwannoma of the upper lip: case report and literature review. Am J Otolaryngol. 2003;24:351-354.
9. Sergheraert J, Zachar D, Furon V, Khonsari RH, Ortonne N, Mauprivez C. Oral plexiform schwannoma: a case report and relevant immunohistochemical investigation. SAGE Open Med Case Rep. 2019; 19;7:2050313X19838184.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}