


Rogerio Nabor Kondo; Carlos Borges Junior; Laís Gonzalez Leugi; Marina Gubert; Fabiana De Mari Scalone
Submitted on: 20/10/2023
Approved on: 08/01/2024
Financial support: None.
Conflict of interest: None.
How to cite this article: Kondo RN, Borges Junior C, Leugi LG, Gubert M, Scalone FM. Electrosurgery in rhinophyma: report of two cases. Surg Cosmet Dermatol. 2024;16:e20240312.
Rhinophyma is characterized by chronic inflammation of the tissues of the nose, resulting in irregular exophytic growth and telangiectasias. The disease progresses with hyperplasia and hypertrophy of the nasal sebaceous glands, associated with fibrosis and dilation of local blood vessels and connective tissue. These changes can lead to complete nose deformity and compromise the patients' quality of life. There are different treatment methods, such as laser, microdermabrasion, chemical exfoliation, cryosurgery, surgery with skin graft, and electrosurgery, with varying results and costs. We report two cases of rhinophyma treated with electrosurgery with very satisfactory results.
Keywords: Rhinophyma; Electrosurgery; Case Reports; Acquired Nasal Deformities.
Rhinophyma, also called alcoholic nose and nasal elephantiasis, among others, is characterized by chronic inflammation of the nose tissues with changes in texture, color, and vascularization, resulting in irregular exophytic growth and telangiectasias.1,2 This clinical condition has a strong association with alcoholism and rosacea, and some authors consider it the final stage of the latter.2 It can be classified as simple hypertrophic when it evolves with hyperplasia and hypertrophy of the nasal sebaceous glands or fibroangiomatotic when associated with fibrosis and dilation of blood vessels and local connective tissue.1 These changes are responsible for giving the region a tuberous appearance and darker color and can lead to complete deformity of the nose.1
The prevalence of rhinophyma is 5% to 10% in the general population, and it is observed frequently in middle-aged and elderly men.3,4 Some studies have demonstrated ratios of 12 men to one woman.2 Other associated factors include a positive family history of rhinophyma, excess sun exposure, and high consumption of spicy foods and caffeine – all of these cause facial flushing and rosacea, predisposing factors to the appearance of the lesion.1,2
In addition to being an aesthetic problem as it is located in the central region of the face, exophytic growth can hide a basal cell carcinoma (BCC).5,6 The literature cites several treatments with varying results and costs.4,5 We report two cases of rhinophyma without association with skin neoplasms, treated with electrosurgery, a low-cost method with very satisfactory results.
Two patients with fibroangiomatotic rhinophyma underwent surgical procedures:
PATIENT 1: A 46-year-old man was referred to the Dermatology Service to treat a tumor on his nose, which had been growing progressively for four years. The patient was diagnosed with hepatitis B, untreated at the time, had systemic arterial hypertension, and a history of smoking and daily sun exposure without photoprotection. He was taking ramipril 10 mg a day. Examination demonstrated increased nasal volume, erythema, telangiectasias, nodules, and skin thickening, compatible with rhinophyma. The patient denied prior treatment for the condition. The surgical approach was indicated (Figure 1).
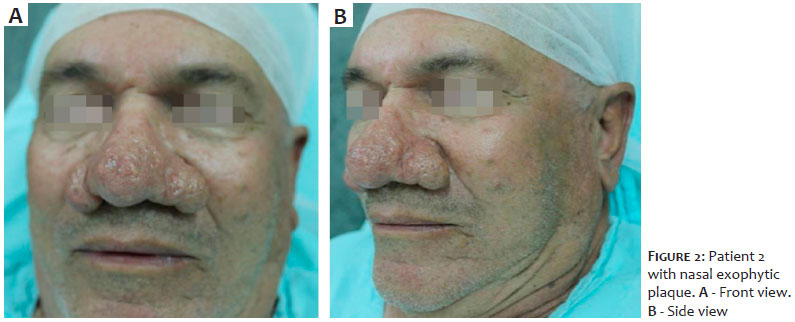
PATIENT 2: A 71-year-old man attended the Dermatology Service due to complaints of increased nasal volume for 20 years, with significant worsening for three years. He had systemic arterial hypertension as a comorbidity and denied alcohol consumption or smoking. He was taking atenolol 25 mg a day. A dermatological examination showed a nose with skin thickening, nodules, and erythema. Surgical treatment was indicated (Figure 2).
Description of the technique:
Patient in horizontal supine position;
Antisepsis with topical 10% polyvinyl iodine;
Placement of surgical drapes;
Infiltrative anesthesia using 2% lidocaine with vasoconstrictor. Wait two minutes for the procedure;
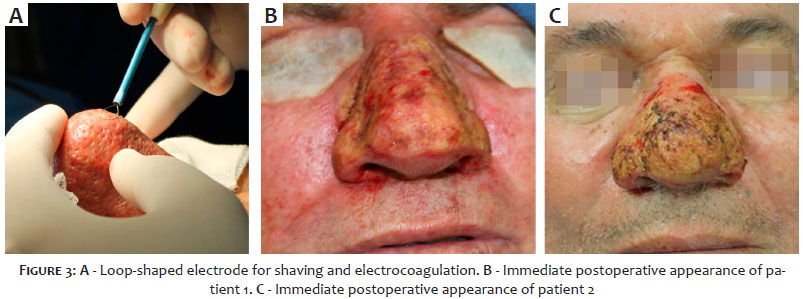
Electrocoagulator in cutting mode and power 20 (Wavetronic® 5000 Digital) and introduction of the loop electrode (Figure 3A), cutting the skin at a depth of 2 mm to 3 mm and sculpting the spare parts;
Electrocoagulator in coagulation mode to achieve local hemostasis. Depending on the need to remodel the nose, it is possible to return to the cutting mode to excise excess skin, and hemostasis is completed again in the coagulation mode;
Once the electrocoagulated nasal tissue is standardized and hemostasis is complete, local cleaning is performed with saline solution (Figure 3B and 3C);
The procedure is completed with an occlusive dressing with gauze and neomycin ointment. The dressing is fixed with hypoallergenic tape.
The return is made after 24 hours to remove the first dressing, with instructions for occlusive dressings (once daily) with collagenase ointment 0.6 U/g with chloramphenicol 0.01 g/g and reassessment in seven days. After this return, only collagenase ointment (without chloramphenicol) is recommended, keeping the surgical wound without occlusion and weekly visits until completing one month.
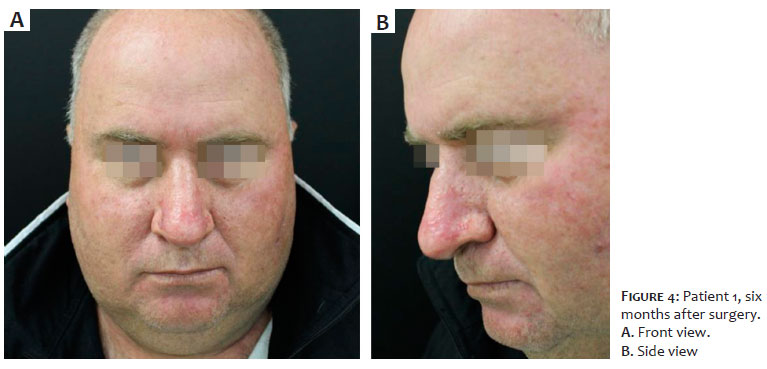
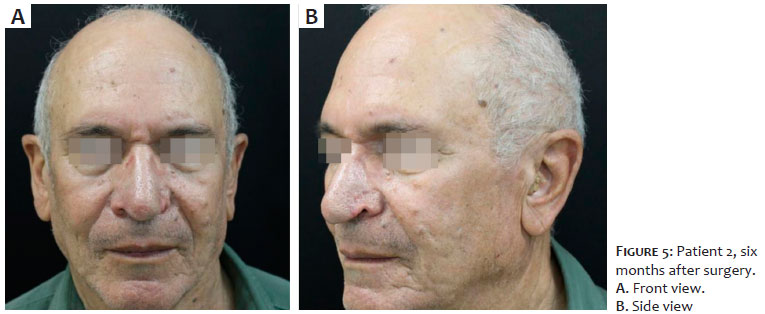
Both patients evolved without hemorrhage in the immediate postoperative period, presenting total epithelialization of the surface of the nose, without unsightly scars, preserving the nasal shape (Figures 4 and 5). Patients reported great satisfaction with the result.
Hebrea, in 1845, replaced names such as "cauliflower" or "alcoholic" nose with the term rhinophyma. This nomenclature is accepted worldwide and derives from the Greek rhino (nose) and phyma (growth). It is a disease that is not only disfiguring but can also negatively impact respiratory function, causing nasal obstruction.1
El-Azhary et al. (1991) classified rhinophyma into three forms: minor, moderate, or major. The minor form is when the patient presents telangiectasias accompanied by mild skin thickening. The moderate type is when lobes accompany the skin thickening. Lastly, the major form is when there are prominent nodules and nasal hypertrophy.7
There are several approaches varying according to the rhinophyma classification. The most frequently cited methods are YAG/CO2 laser, surgical microdermabrasion, electrosurgery (electrocoagulation), cryosurgery, high-frequency equipment (radiofrequency), and total excision with a cold blade and grafting. There is no method of choice in the literature, as costs and results vary, and there is a surgeon-dependent factor.3
The YAG/CO2 laser has a good response but is expensive. Microdermabrasion may require several sessions. Cryosurgery can leave residual post-inflammatory hypochromia, especially in patients with higher skin phototypes. The aesthetic result with grafting is generally unsatisfactory, but it can be used for reconstruction when there is associated BCC.3,5
Electrosurgery (ELC), on the other hand, is a simple technique with a low cost of materials. The disadvantages are the difficulty in delimiting the tissue to be excised (surgeon-dependent) and the risk of leaving a scar when going too deep into the skin to be removed.5
A vasoconstrictor associated with the anesthetic and manual compression or using the blend mode (mixture of 50% cutting and 50% coagulation) at the time of surgery can reduce bleeding, another ELC complication.
Our described cases agree with the literature and corroborate the good results obtained with the technique.4,5
Rhinophyma treatment can be conducted using several methods, with their risks and surgeon-dependent factors. Among them, electrosurgery presents a low cost and shows satisfactory results, as in the cases presented.
Rogerio Nabor Kondo
ORCID: 0000-0003-1848-3314
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in research guidance; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Carlos Borges Junior 0009-0005-2561-3879
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical review of the manuscript.
Laís Gonzalez Leugi 0009-0009-2586-8141
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical review of the manuscript.
Marina Gubert
ORCID: 0000-0002-9293-5019
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical review of the manuscript.
Fabiana De Mari Scalone
ORCID: 0000-0002-5050-8246
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical review of the manuscript.
1. Daoud M, Ullas G, Kumar R, Raghavan U. Rhinophyma: combined surgical treatment and quality of life. Facial Plast Surg. 2021;37(1):122-131.
2. Chauhan R, Loewenstein SN, Hassanein AH. Rhinophyma: prevalence, severity, impact and management. Clin Cosmet Investig Dermatol. 2020;13:537-551.
3. Dugourd PM, Guillot P, Beylot-Barry M, Cogrel O. Surgical treatment of rhinophyma: retrospective monocentric study and literature review. Ann Dermatol Venereol. 2021;148(3):172-176.
4. Dornelas MT, Correa MPD, Dornelas MC, Dornelas GV, Correa LD, Dornelas LV, et al. Rinofima: análise da técnica cirúrgica por Shave Excision. Rev Bras Cir Plast. 2017;32(3):328-331.
5. Caiado BC, Neto BRC, Caiado LC, Hakme F. Rinofima: aspectos importantes da patologia e tratamento cirúrgico com eletrocautério. Arq Cat Med.2015;44(Supl 1):S180-82.
6. Vasconcelos BN, Vasconcellos JB, Fonseca JCM, Fonseca CR. Dermoquimioabrasão: um tratamento eficaz e seguro para o rinofima. Surg Cosmet Dermatol. 2016;8(1):28- 31.
7. Kassirer SS, Gotkin RH, Sarnoff DS. Treatment of Rhinophyma with fractional CO2 laser resurfacing in a woman of color: case report and review of the literature. J Drugs Dermatol. 2021;20(7):772-775.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}