


Rogerio Nabor Kondo; Ana Carolina Cechin Alves; Camila Medyk; Luis Felipe Stella Santos
Submitted on: 31/03/2023
Approved on: 27/04/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Kondo RN, Alves ACC, Medyk C, Santos LFS. Shark island pedicle flap: a series of two cases. Surg Cosmet Dermatol. 2023;15:e20230241.
Basal cell carcinoma (BCC) is the most common skin cancer. Depending on its size and location, the reconstruction of the defect resulting can become very challenging for the dermatological surgeon. Shark Island Pedicle Flap (SIPF) technique is used for defects mainly in the alar or perialar nasal region, but we also use it in a modified way to close a large lesion defect in the cutaneous portion of the lip. We report two cases, one being the application of classic SIPF and the other a modified one, in which both results were satisfactory, both in terms of cosmetics and functionality.
Keywords: Carcinoma; Basal cell; Surgical flaps; Nose; Case reports
Basal cell carcinoma (BCC) is the most common type of skin cancer.1 Depending on the size and location of the tumor, the defect resulting from excision requires reconstruction with flaps, grafts, or both at the same time, making it a very challenging surgical procedure.2,3
The Shark Island Pedicle Flap (SIPF) is a rotating island flap where part of the pedicle makes a movement to "snap" the defect, and the final design of the flap resembles a shark's fin. Usually, it is used to correct circular defects in the nasal alar or perialar region, in which the adjacent skin above and laterally to the defect is used to provide greater mobility to the flap.3,4,5
We report two cases where we used reconstruction with SIPF after excision of nasal BCC, one with a lesion in the nasal alar region (where the flap is recommended) and the other with a lesion in the cutaneous portion of the lip (area not yet reported in the literature), with satisfactory aesthetic results in both cases. This case report aims to demonstrate SIPF as an option to correct defects in the cutaneous portion of the lip, with easy execution and a good level of patient satisfaction.
We treated one patient with BCC in the right nasal alar region and another with two BCCs in the cutaneous portion of the lip.
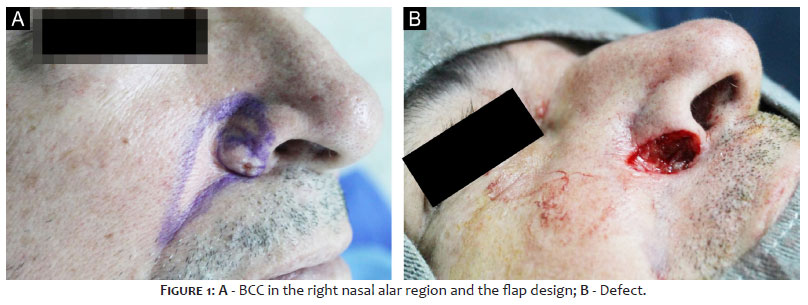
PATIENT 1: A 69-year-old man, skin phototype III, from Londrina (PR), presented a pearly plaque, 11x7 mm, in the nasal alar region on the right. The biopsy confirmed BCC and the lesion was excised with safety margins of 3 mm. The resulting defect was 14x10 mm and SIPF was chosen (Figures 1, 2, 3 and 4).
PATIENT 2: A 66-year-old man, skin phototype III, from Londrina (PR), presented two lesions: one was a hyperchromic papule, measuring 10x7 mm, and the other was a papule measuring 5x5 mm, in the region of the right nasolabial fold and in the cutaneous portion of the lip on the right. Biopsies confirmed BCCs, and the two lesions were excised en bloc with safety margins of 4 mm. The resulting defect was 35x15
Description of the technique used in patient 1 (Figures 1 e 2):
a) Patient in horizontal supine position;
b) Marking of the lesion with methylene blue or a surgical pen with a 3 mm margin and flap incision sites: an arc that starts from the defect, in its inferior-medial portion, contouring and rising up to 10 mm from the defect (size of the transverse diameter of the defect), descending at 45 degrees until it meets the nasolabial fold and returning to the lower edge of the defect (Figure 1A);
c) Antisepsis with topical 10% polyvinyl iodine;
d) Placement of surgical drapes;
e) Infiltrative anesthesia with 2% lidocaine with vasoconstrictor;
f) Incision with a 15 blade of the lesion and en bloc excision of the piece;
g) Hemostasis;
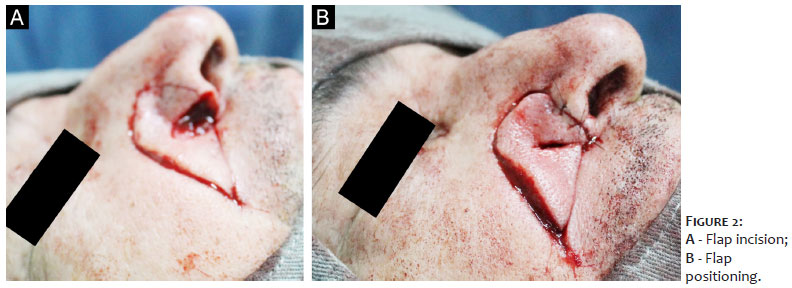
h) Incision of the flap, starting from the defect, making an arc that starts from the defect, in its inferior-medial portion, rising up to 10 mm from the defect, descending at 45 degrees until it meets the nasolabial fold and returning to the lower edge of the defect (according to prior marking);
i) Flap detachment, keeping the pedicle in the central region;
j) Positioning of the flap and other sutures with 5.0 mononylon, simple stitches. Approximation of the medial and lateral portion around the defect. Appearance of the flap "capturing" the defect (shark bite) and image of an inverted cone (shark fin) (Figures 2A e 2B);
k) Local cleaning with saline solution;
l) Occlusive dressing.
Description of the technique used in patient 2 (Figuras 5, 6 e 7):
a) Patient in horizontal supine position;
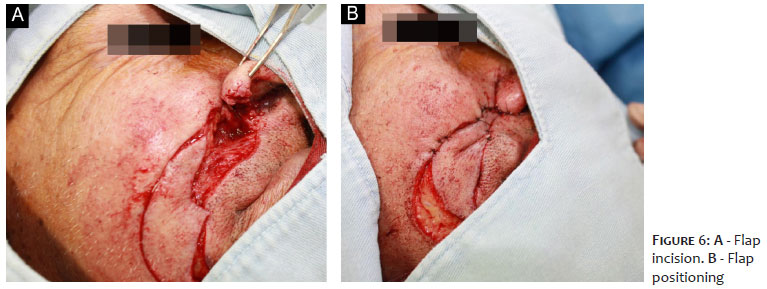
b) Marking of the lesion with methylene blue or a surgical pen with a margin of 4 mm from the largest lesion and 3 mm from the smaller lesion, with planning for excision of the two lesions en bloc. Flap design: an arc that starts from the upper region of the defect, keeping 1 0 mm away from the nasolabial fold until 10mm below the labial commissure and returning 5 mm away from the nasolabial fold (same longitudinal width as the defect) to the lower portion of the defect (Figures 5 e 6);
c) Antisepsis with topical 10% polyvinyl iodine;
d) Placement of surgical drapes;
e) Infiltrative anesthesia with 2% lidocaine with vasoconstrictor;
f) Disinsertion of the right nasal ala (this was chosen, in this specific case, to facilitate excision with margin of the lesion);
g) Incision with a 15 blade of the lesion and en bloc excision of the piece;
h) Hemostasis;
i) Incision of the flap, starting from the upper region of the defect, moving up to 10 mm below the lip commissure and returning to the lower portion of the defect in the lower region of the defect (according to prior marking);
j) Flap detachment, maintaining the vascular pedicle in the central region;
k) Positioning of the flap and reinsertion of the right nasal ala with 5.0 mononylon, simple stitches. The union of the upper and lower medial portion of the flap appears to "engulf" the defect (shark bite) and the final appearance of a shark fin (Figures 6A, 6B e 7A);
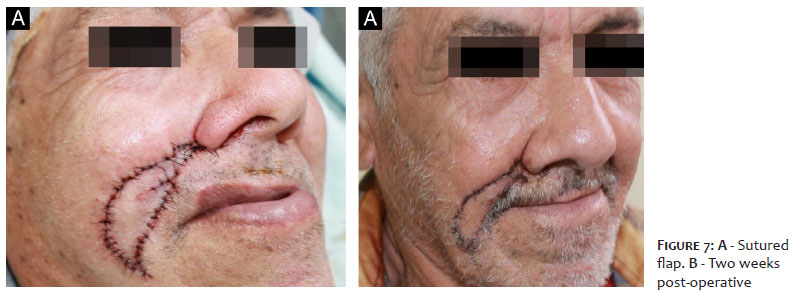
l) Complete suture with 5.0 mononylon, single stitches (Figure 7A);
m) Local cleaning with saline solution;
n) Occlusive dressing.
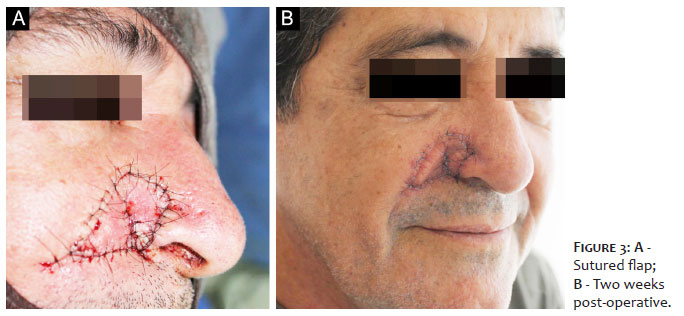
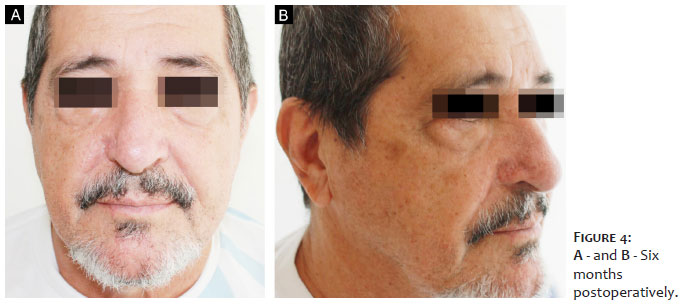
PATIENT 1: The patient evolved uneventfully in the first few days after surgery. There was good healing and accommodation, with a satisfactory aesthetic result in the late postoperative period. (Figures 3B, 4A e 4B).
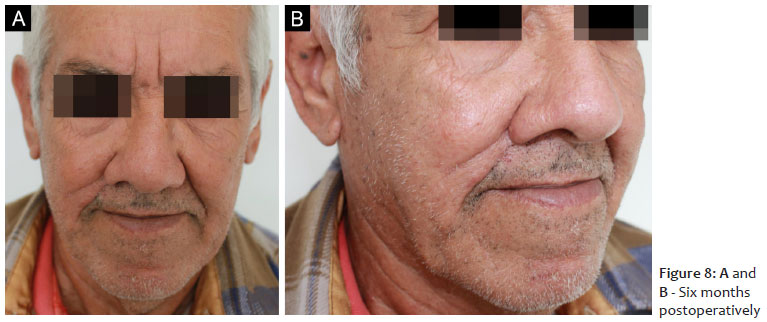
PATIENT 2: The patient evolved uneventfully in the immediate postoperative period. There was good healing and accommodation, with a satisfactory aesthetic result in the late postoperative period. (Figures 7B, 8A e 8B).
SIPF is an island flap technique that maintains the vascularization in its central region. It was described by Cvancara (2006) to correct defects in the nasal alar or perialar wall, and is considered a good alternative, as it can be performed in a single surgical procedure. The configuration of the flap to "capture" the defect and the final appearance of a fin led to the name "shark island".3
There is no exclusivity for applying SIPF in the nasal alar or perialar region. However, there is a recommendation for these locations, as it leads to the natural creation of the nasal groove.3-5 Nevertheless, when applying an island flap, resembling the shark's bite and fin, we will have a SIPF.
In patient 1, we performed a classic SIPF. We made an incision of an arch starting from the defect, in its inferior-medial portion, contouring in the arc in the upper portion, descending until it meets the nasolabial fold and returning to the lower edge of the defect. (Figure 1A).
In patient 2, we applied modified SIPF to the defect in the cutaneous portion of the lip. We created an arc starting from the upper region of the defect, 10 mm away from the nasolabial fold to 10 mm below the labial commissure and returning 5 mm away from the nasolabial fold to the lower portion of the defect, thus maintaining the same longitudinal width of the defect (Figures 5 e 6).
The SIPF requires less displacement from the donor area to the defect than a simple island advancement flap, as it makes better use of the adjacent tissues with the rotational movement, leaving less local tension. In patient 2, for example, if the upper and lower ends adjacent to the defect were not united ("engulfing" the defect), we would have to increase the length of the flap.
Still in case 2, we chose to disinsert the nasal ala to ensure complete removal of the tumor, as we did not have a micrographic surgeon during the surgery. Despite the large defect after excision, an acceptable and functional final result was possible using SIPF.
The use of SIPF can be a good option for resolving defects in the nasal alar or perialar regions and also in the cutaneous portion of the lip.
Rogerio Nabor Kondo
ORCID: 0000-0003-1848-3314
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; effective participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Ana Carolina Cechin Alves
ORCID: 0009-0007-6862-6287
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical review of the manuscript.
Camila Medyk
ORCID: 0009-0000-3491-5813
Approval of the final version of the manuscript; effective participation in research orientation; critical literature review; critical review of the manuscript.
Luis Felipe Stella Santos
ORCID: 0000-0001-7982-3875
Approval of the final version of the manuscript; preparation and writing of the manuscript; effective participation in research orientation; critical review of the literature.
1. Kondo RN, Cestari AI, Soares BM, Scalone FDM, Yabar SIA. Pinwheel flap as an option to reconstruct a nasal defect: a series of two cases. Dermatol Arch. 2021;5(1):122-6.
2. Kondo RN, Maia GB, Bertoncini LA, Silva ST. Retalho em caracol como uma opção de reconstrução de defeito nasal: uma série de dois casos. Surg Cosmet Dermatol. 2022;14:e20220043.
3. Cvancara JL, Wentzell JM. Shark island pedicle flap for repair of combined nasal ala-perialar defects. Dermatol Surg. 2006;32(5):726-9.
4. André MC, Fraga A, Garcia CR, Pignatelli JG, Soares RO. Retalho em ilha de tubarão: uma técnica cirúrgica reconstrutiva de defeitos localizados na área nasal alar/perialar. Um procedimento simples. An Bras Dermatol. 2011;86(4Suppl1):160-3.
5. Saraiva LPPG, Guimarães RV, Loda G, Benez M. Retalho de pedículo subcutâneo em formato de tubarão na região perialar. Surg Cosmet Dermatol. 2020;12(S1):11-4.
6. Feit NE, Dusza SW, Marghoob AA. Melanomas detected with the aid of total cutaneous photography. Br J Dermatol. 2004;150(4):706-14.
7. Fernandes NC, Calmon R, Maceira JP, Cuzzi T, Silva CSC. Melanoma cutâneo: estudo prospectivo de 65 casos. An Bras Dermatol. 2005;80(1):25-Hornung A, Steeb T, Wessely A, Brinker TJ, Breakell T, Erdmann M, et al. The value of total body photography for the early detection of melanoma: a systematic review. Int J Environ Res Public Health. 2021;18(4):1726.
8. Grupo Brasileiro de Melanoma. Recomendações para o tratamento do melanoma cutâneo. São Paulo: GBM; 2019. Disponível em: https://gbm.org.br/wp-content/uploads/2019/09/Livro-GBM.pdf
9. Kelly JW, Yeatman JM, Regalia C, Mason G, Henham AP. A high incidence of melanoma found in patients with multiple dysplastic naevi by photographic surveillance. Med J Aust. 1997;167(4):191-4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}