


Amanda Cochlar Medeiros Perrella; José Roberto Pereira Pegas; Mariana Reis e Rocha Dultra; Paula Barros Curvo Costa; Tayna Rangel Barreto
Submitted on: 24/04/2023
Approved on: 21/07/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Perrella ACM, Pegas JRP, Dultra MRR, Costa PBC, Barreto TR. Peristomal Pseudoverrucous Epitheliomatous Hyperplasia. Surg Cosmet Dermatol. 2023;15:e20230255.
The incidence of stoma complications ranges from 20-70%. Pseudoverrucous Epitheliomatous Hyperplasia (PEH) is a rare complication of the peristomal skin of unknown incidence, without protocol treatment, and with a significant impact on the patient's quality of life. There are numerous ways to treat peristomal lesions, mostly outpatient care. We report a case of peristomal PEH in which surgical intervention was performed using the shaving technique with very satisfactory aesthetic and functional results.
Keywords: Ileostomy; Colostomy; Hyperplasia
The incidence of stoma complications ranges from 20-70%.1 Pseudoverrucous epitheliomatous hyperplasia (PEH) is a rare complication of peristomal skin of unknown incidence, non-protocol treatment, and that impacts the patient's quality of life significantly.2,3
A 69-year-old man with definitive terminal colostomy due to colorectal neoplasia for 18 years presented a history of peristomal skin lesion of insidious onset and slow growth for approximately two years. The lesion appeared as a violet-brown papillomatous plaque, friable upon manipulation and extremely painful (Figure 1). It substantially impacted the patient's quality of life and, mainly, the patient's sleep. We raised the hypothesis of allergic contact dermatitis (ACD) due to the products used in the colostomy bag system. The patch test presented readings at 48h and 96h, and it was positive in a cross for rosin, a substance present in adhesives, insulation, glues, paper, cardboard, cosmetics, insecticides, and topical medicines. The test battery included products that the patient used in the peristomal region, such as powder, ointment, and barrier spray, all with negative readings.
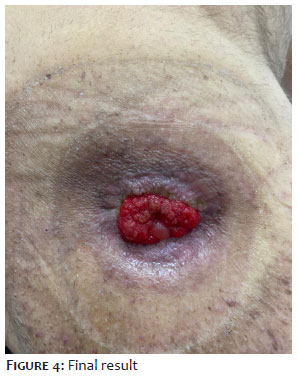
The patient underwent chemocauterization with a 10% silver nitrate caustic stick and 70% trichloroacetic acid, with little improvement (Figure 2). Three weeks later, we performed the surgical excision using the shaving technique with a surgical blade, and the level of excision reached the reticular dermis. We sent all the material for the histopathological study. The patient used mupirocin for seven days on the surgical wound in the immediate postoperative period, followed by potassium permanganate compresses and a tape dressing with calcium alginate. One week after the procedure, the surgical wound presented granulation tissue, little fibrin, and a moist surface (Figure 3). It progressed over six weeks, with complete skin recovery and pain improvement (Figure 4).
Temporary or permanent ileostomies and colostomies may be necessary to treat several pathological conditions such as congenital anomalies, intestinal obstruction, inflammatory bowel diseases, trauma, or neoplasia.4
Proper stoma care, nutrition, and patient water balance allow most ostomy patients to have a healthy social, professional, and sexual life.1,5,6
A colostomy bag system consists of a colostomy bag, a skin barrier, and a water-resistant adhesive.
The skin barrier consists of a flexible hydrocolloid plate that can be pre-cut or cut by the patient to fit the stoma-skin junction. Cutting the hydrocolloid plate in a personalized way more effectively prevents stoma effluent from coming into contact with the skin. It also allows it to be adapted to monitor postoperative anatomical changes, which occur with reduced edema. The adhesiveness of the hydrocolloid is broken by moisture, so the bag's usage time is generally four days to prevent chemical irritation due to leakage.2,4
The literature does not recommend washing the bag since water and detergents soften the bag's adhesive, reducing its usage time.2
If an excessively full and, consequently, heavy bag can detach from the skin, it is recommended to empty it six or more times a day.2
Another recommendation is accessory products to help improve the fixation of the bag, such as adhesive agents and skin preparation agents, as well as to prevent irritation of the peristomal skin with ointments, powders, and barrier sprays.5
Between 20% and 70% of ostomized patients will experience an ostomy-related complication.1 Skin complications occur in 25-43% of ileostomies patients and 7-20% of colostomies patients.2
The anatomical location and type of stoma have different impacts on its management. Loop colostomies tend to be larger and, in some ways, more difficult to care for than terminal colostomies. The location of the stoma concerning the ileocecal valve determines the type and volume of the effluent and the flow rate. As effluents from the small intestine are richer in proteolytic enzymes, patients with ileostomies must take care of their peristomal skin thoroughly. Colostomy patients produce feces that do not contain digestive enzymes, putting them at a lower risk of peristomal skin lesions.1,5,6
Skin lesions should be treated aggressively to prevent their progression. The treatment strategy includes, for most peristomal skin complications, colostomy bag system adjustment and topical treatment to promote healing.2,5 Chemical dermatitis is a common problem that affects more than 34% of ileostomized patients. The slightly acidic nature of the skin (pH: 4.0-5.9) contributes to the normal function of the skin barrier.9 Ileostomies continually produce an aqueous, alkaline effluent rich in proteolytic enzymes that irritate the exposed peristomal skin. Chronic leakage causes maceration and integrity loss of the skin barrier that can quickly progress to painful ulceration. The distribution of chemical dermatitis topographically corresponds to the leak. Inadequate location and protrusion of the stoma and inadequate size of the bag system can generate dermatitis associated with leakage. Furthermore, keeping the bag worn out, generally when it has been in use for more than five days, can cause the protection of the hydrocolloid plate to disintegrate, leading to a silent leak that can generate chemical irritation in a matter of hours of exposure. Creating an adequately protruding stoma (1-2 cm for colostomy and 2-3cm for ileostomies) located in a flat abdomen area, with an appropriately coupled bag system, can prevent dermatitis associated with leakage. The skin lesion improves quickly after identifying and correcting the leak, often with filler pastes and/or a convex-based bag system. The hydrocolloid powder will help prevent loss of skin integrity. Operative repositioning of the ostomy is rarely indicated for recalcitrant leakage dermatitis.2,7,8,9,10
Allergies can arise from any product used in the ostomy, such as plates, powders, ointments, belts, cleaning products, and adhesives. Allergic reactions are rare but can produce erythema, vesicles, itching, and pain at the site. Allergic contact dermatitis (ACD) should be suspected when changing products used in the ostomy. An easy way to empirically diagnose ACD is to apply a small amount of the suspected product to a small area of the patient's skin for 24-48 hours. A formal patch test should be performed in case of no allergic reactions. ACD treatment begins by replacing the product that contains the allergenic substance. Subsequently, it can be treated with topical corticosteroids, and the need for systemic corticosteroids is rare.2,7,8,9,10
Pseudoverrucous epitheliomatous hyperplasia (PEH) is an uncommon sequelae of chronic primary irritant contact dermatitis, hypothetically arising from chronic exposure to moisture. Chronic peristomal humidity generates benign pseudoverrucous changes around the stoma that appear, as they grow, to be an infiltrated and irregular skin lesion with multiple color variations. Patients may report itching, pain, or bleeding. The pathological study may reveal acanthosis, elongation of epidermal ridges, hyperkeratosis, and dermis inflammation. The differential diagnosis involves condyloma, neoplasia, bacterial infection, and candidiasis. Treatment comprises reevaluating the skin barrier and readjusting the opening of the hydrocolloid plate. However, the area of the lesion, due to its irregularity, may prevent adequate coupling. Topical silver nitrate may resolve the raised skin lesion. Infiltration with corticosteroids may be necessary, and more extensive and severe lesions may require surgical excision.2,3
In this case report, we ruled out chemical dermatitis as causing the lesion, as the effluent had a colonic origin, that is, non-proteolytic or very alkaline. We also ruled out ACD since there was no adhesive material close to the lesion but in a more distal region, where the hydrocolloid plate and the bag's flange system were fixed to the skin. Furthermore, the result of the anatomopathological study was more compatible with PEH as it exhibits a non-specific chronic inflammatory process with the absence of spongiosis.
The fact that the patient's colostomy bag can be decoupled for cleaning using a flange system, without the need to detach the adhesive and hydrocolloid plate from the skin, may have been a predisposing factor to less frequent changes of the colostomy bag system, and, consequently, possible wear of the adhesiveness of the hydrocolloid plate, generating silent leakage of the effluent that led to contact dermatitis due to primary irritant and, over time, PEH.
We opted for surgical intervention, using the shaving technique, to remove the lesion due to its extension and chronicity, in addition to the poor response to topical treatment with silver nitrate and trichloroacetic acid in an attempt at chemocauterization. An excellent aesthetic and functional result was obtained, significantly improving the patient's quality of life with pain remission
Rare conditions that do not have treatments established in the literature become a real challenge for the dermatological surgeon. They must use their expertise in operative techniques from other cases, often very different, to extrapolate to the case in question. Malpractice in attempting to surgically correct this skin lesion in such a delicate area can generate a complication worse than the primary cause and, therefore, require a much larger intervention than reconstructing the ostomy in another location.
Several peristomal skin conditions are preventable with care of the peristomal skin and the colostomy bag system. Therefore, frequent multidisciplinary follow-up with stoma therapy doctors and nurses is essential for ostomized patients to educate and correct any identified complications early.
Amanda Cochlar Medeiros Perrella
ORCID: 0000-0002-5265-6445
Study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
José Roberto Pereira Pegas
ORCID: 0000-0002-2541-6008
Study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript.
Mariana Reis e Rocha Dultra
ORCID: 0000-0003-0510-221X
Critical literature review.
Paula Barros Curvo Costa
ORCID: 0000-0002-4114-4137
Critical literature review.
Tayna Rangel Barreto
ORCID: 0000-0002-9623-6397
Critical literature review.
1. Shabbir J, Britton DC. Stoma complications: a literature overview. Colorectal Dis. 2010;12(10):958-64.
2. Steinhagen E, Colwell J, Cannon LM. Intestinal stomas - postoperative stoma care and peristomal skin complications. Clin Colon Rectal Surg. 2017;30(3):184-92.
3. Douri T, Shawaf AZ. Letter: pseudoverrucous papules and nodules: a case report. Dermatol Online J. 2012;18(4):14.
4. Doughty D. Principles of ostomy management in the oncology patient. J Support Oncol. 2005;3(1):59-69.
5. Salvadalena G. Incidence of complications of the stoma and peristomal skin among individuals with colostomy, ileostomy, and urostomy: a systematic review. J Wound Ostomy Continence Nurs. 2008;35(6):596–607, quiz 608–609.
6. Hendren S, Hammond K, Glasgow SC, Perry WB, Buie WD, Steele SR, et al. Clinical practice guidelines for ostomy surgery. Dis Colon Rectum. 2015;58(4):375–87.
7. Agarwal S, Ehrlich A. Stoma dermatitis: prevalent but often over-looked. Dermatitis 2010;21(3):138–47.
8. Meisner S, Lehur PA, Moran B, Martins L, Jemec GBE. Peristomal skin complications are common, expensive, and difficult to manage: a population based cost modeling study. PLoS One. 2012;7(5):e37813.
9. Nybaek H, Jemec GB. Skin problems in stoma patients. J Eur Acad Dermatol Venereol. 2010;24(3):249–57.
10. Lyon CC, Smith AJ, Griffiths CE, Beck MH. The spectrum of skin disorders in abdominal stoma patients. Br J Dermatol. 2000;143(6):1248-60.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}