


Bhertha Miyuki Tamura
Submitted on: 24/03/2021
Approved on: 27/09/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Tamura BM. New indication for calcium hydroxyapatite: safe rejuvenation of the dorsum of the foot based on anatomy. Surg Cosmet Dermatol. 2023;15:e20230003
INTRODUCTION: For religious reasons, a portion of the population does not expose their body, showing only the feet.
OBJECTIVE: This study aimed to meet the demand for treatments to rejuvenate the dorsum of the foot, observe the safety of using calcium hydroxyapatite and its results, and discuss the region anatomy.
METHODS: Sixty women with an average age of 63 years and skin phototypes from I to VI had the dorsum of their foot's age classified by types from I to VII, and were injected with 0.75 ml to 3 ml of calcium hydroxyapatite per patient in this region, in a single session. A dermatologist who did not participate in the treatment and the patients conducted the evaluation through photos.
RESULTS: The results were considered good to very good depending on the aging stage of the dorsum of the feet. Complications were limited to local edema and erythema. Follow-up lasted from six months to one year.
CONCLUSION: The injection of calcium hydroxyapatite into the dorsum of the feet, based on knowledge of the anatomy of this region and correct volume, could be considered a body area treatment.
Keywords: Calcium Hydroxyapatite; Foot; Anterior Compartment Syndrome; Collagen
Although Brazil's majority religion is Christianity, there is a growing community of Muslims, some of whom are radical. The demand for procedures on the dorsum of the feet began with requests from this population to rejuvenate the part of the body exposed below the typical clothing or burkas. This demand, both in countries with a Muslim majority and in others, has shown the need for body treatment based on an anatomical study of the dorsum of the feet. Knowledge of this technique caused interest among Brazilian patients with high expectations regarding body beauty.
Anatomical studies of the dorsal region of the feet1,2 focusing on biostimulator injections and fillers are not conducted frequently. A better understanding of the local anatomy to avoid anterior compartment syndrome and the triggering of vascular injuries leads us to know the ideal injection plan. Furthermore, following the global trend, priority is given to choosing injection techniques using cannulas.
This study aimed to meet the growing and unusual demand for treatment indications in an uncommon area and to observe its safety and results based on an evaluation of the local anatomy.
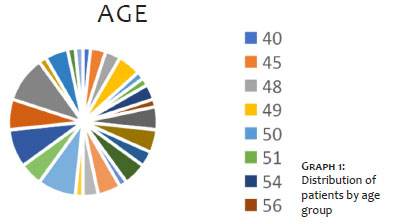
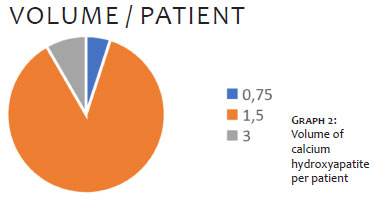
We selected 60 women with an average age of 63 years (between 40-74 years – Graph 1) with skin phototypes I to VI: five patients with skin phototype I; 13 with II; 11 with III; 2 with IV; 21 with V; and 8 with skin phototype VI. Regarding the classification of the dorsum of the feet aging, we only treated patients with types between III and VI. We chose calcium hydroxyapatite to treat the biostimulation of the skin on the dorsum of the feet, and the injected volume varied between 0.75 ml and 3 ml per patient in a single session (Graph 2).
As selection criteria, we included patients without arterial insufficiency, who were not using anticoagulants, without chronic illness or pain when walking, and without any other systemic disease that could contraindicate any aesthetic treatment to rejuvenate the dorsum of the feet. The patient should be able to understand the procedure and its possible complications, report any adverse event, and follow instructions to massage the treated area every four hours during the first day after the procedure, in addition to wearing comfortable shoes until complete recovery of the possible edema.
The dorsum of the feet aging were classified into types I to VII (Figure 1), where type I represents the dorsum of a young foot, without changes in the skin and subcutaneous tissue and visualization of veins; type II shows a slight decrease in subcutaneous tissue and slight visualization of the vascular network; type III presents a vascular network, with or without visualization of the tendons; type IV has the addition of visible loss of subcutaneous tissue to the previous characteristics; type V represents skin with melanosis and possible changes in the subcutaneous tissue; type VI has signs of venous stasis and/or vascular insufficiency; and type VII shows complete vascular changes, skin aging and atrophy, which appears parchment-like or with sequelae of stasis, such as ochre dermatitis.
Only patients with the dorsum of the foot aging types III to VI underwent therapy. We conducted simple digital photographic documentation in pre-treatment, immediate post-treatment, and 30 days after the procedure. A dermatologist not involved in the treatment and the patient assessed the improvement according to the table of types of foot aging.
Technique used:
a) Antisepsis with alcoholic chlorhexidine solution;
b) 1.5 ml of calcium hydroxyapatite diluted in 5 ml of 1% lidocaine;
c) A light tourniquet on the ankle to visualize the largest veins on the back of the feet;
d) 1% lidocaine with 1:200,000 adrenaline to anesthetize the cannula entry point with a 23G or 18G needle, depending on the type of cannula used for treatment: 27G x 4cm or 22G x 5cm, respectively;
e) The volume of calcium hydroxyapatite per patient was 0.75 ml to 3 ml;
f) The cannula entry port was located at a single point in the distal region of the third metatarsal, directing the cannula proximally towards the ankle, in a fan shape, distributing the suspension as uniformly as possible;
g) After the injection, a vigorous massage was performed to spread the suspension on the back of the feet.
In the immediate post-procedure period, the patient should rest with her limbs elevated as long as possible for at least two days and massage the treated area every two hours during the first day (except at night); three times a day the second day; and at least once a day for seven days (total of 10 days of massage). We asked patients not to use ice or cold compresses but cool ones, if necessary, without extreme exercise for three days. We also advised them to bypass swimming, sauna, or any other type of activity that could cause contamination to avoid local infection, and avoid compression or tight shoes on the dorsal area of the feet during the first month. Revaluation returns were stipulated at two months, six months, and one year.
The patients received calcium hydroxyapatite in an average volume of 1.6 ml per patient, ranging from 0.75 ml to 3 ml. Although in some cases the volume was small, the results reported by patients varied from good (n = 54 patients), when the improvement occurred with a visible change between the types of aging, to very good (n = 6 patients), when improvement occurred in two types of aging, according to the classification mentioned above. The result reported by the dermatologist was no improvement in one patient, very good in two patients, and good for the others.
In the post-treatment period, one patient had no complaints, 30 presented mild edema, erythema, and mild pain, and 26 had mild to moderate pain. Three patients reported grade 4 (severe) pain, requiring an oral analgesic prescription. Mild local post-procedure pain was considered a regular event due to infiltration of the suspension. The patients did not experience complications other than local edema and erythema, which occurred in 100% of cases, lasting one to three days after treatment.
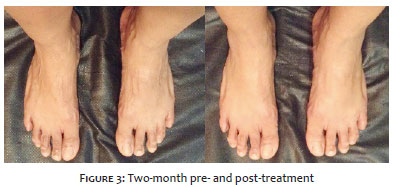
We conducted a two-month follow-up when a dermatologist asked the patients about the results and assessed them. The returns after six and 12 months showed no evidence of adverse events. All patients confirmed that they would repeat the procedure and maintained the results after a one-year follow-up. Figures 2 and 3 show patients before and after treatment with very good responses (Figures 2, 3).
Based on anatomy and the fact that the superficial layer, fascia, and fat on the dorsum of the foot are very thin, we insert the needle bevel facing the dermis, allowing the cannula to enter directed to the safe plane between the superficial and the deep fascia (very similar to the back of the hands). There are no reports on the use of biostimulators on the dorsum of the foot except for the article published by Cotofana.1
The plane between the superficial lamina and the superficial fascia, located with the help of ultrasound, helps the cannula slide easily, without obstacles, and painlessly. The anatomy of the dorsum of the foot is interesting. It's noteworthy that, to rejuvenate the dorsum of the foot, we selected ideal patients without deformities or comorbidities so that there would be no question or biomechanical alteration of the foot or predisposition to thrombotic phenomena.
It is helpful to perform dissections of the dorsum of the foot not only to assess the blood vessels, nerves, and tendons but also to define the planes between the structures and observe whether there would be a safer space between the fasciae for the introduction of cannulas and infiltration of biostimulators. This assessment aims to minimize complications and possible anterior compartment syndrome.
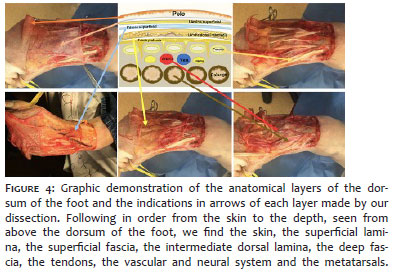
In a summarized description of the area anatomy, we can describe the layers of the dorsum of the foot: the superficial lamina, and then the superficial fascia is just below the skin, lifting it. Below the superficial fascia is the dorsal lamina with a relatively thin subcutaneous tissue layer. After its dissection proximally, the retinaculum is found. Below this subcutaneous tissue of the dorsal lamina layer, the flexor tendons of the fingers rise as a block because they are encompassed by the lamina. Under this plane are the dorsal artery and vein of the foot together with the nerve branches, especially the deep peroneal, involving the metatarsals and phalanges,3 according to the scheme with the anatomical planes shown in Figure 4. Exact knowledge of the planes is essential to evade vascular canalization and, mainly, anterior compartment syndrome,4 our biggest concern. The ideal technique to avoid these complications5 is to infiltrate the biostimulators just below the skin, where the needle that makes the opening for the cannula entry must be introduced, as superficially as possible to try to keep the injection in a higher position concerning the superior plane of the intermediate dorsal lamina, preferably between the skin and the superficial fascia. In these planes, the cannula slides easily without encountering obstacles. If the patient has superficial veins, the gentle passage of the cannula in these areas prevents the formation of bruises or bruises. By keeping the cannula in a superficial position, in the ideal plane, accidents with the superficial venous network do not occur (Figure 4).
Edema of the dorsum of the foot is expected after the procedure, but careful choice of the anatomical plane and a small total volume of a maximum of 1.5 ml per foot/side bypass anterior compartment syndrome. We performed the distribution with the cannula in a fan pattern and not in a bolus to avoid product accumulation. This movement is recommended to distribute the product evenly throughout the area during the massage. It is also essential for the patient to participate during the first few days of the post-procedure, performing the massages.
The injection of collagen biostimulators into the dorsum of the feet, based on an adequate classification of aging in this region, in-depth anatomical knowledge, and satisfactory volume, can open promising perspectives to treat this new body area.
Bhertha Miyuki Tamura
ORCID: 0000-0001-7259-2998
Statistical analysis, Approval of the final version of the manuscript, Study design and planning, Preparation and writing of the manuscript, Collecting, analyzing and interpreting data, Effective participation in research orientation, Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases, Critical review of the literature, Critical review of the manuscript.
1. Custozzo A, Konstantin F, Schenck TL, Gotkin RH, Smith MP, Green JB, Sykes J, et al. Anatomy of the dorsum of the foot and its relevance for nonsurgical cosmetic procedures. Plast Reconstr Surg. 2020;146(1):64-72.
2. Vazquez-Zorrilla D, Millan-Alanis JM, Alvarez-Villalobos NA, Elizondo-Omaña RE, Guzman-Lopez S, Vilchez-Cavazos JF, Fernandez-Rodarte BA, et al. Anatomy of foot compartments: a systematic review. Ann Anat. 2020;229:151465.
3. Al-Himdani S, Din A, Wright TC, Wheble G, Chapman TWL, Khan U. The medial sural artery perforator (MSAP) flap: a versatile flap for lower extremity reconstruction. Injury. 2020;51(4):1077-1085.
4. Yunoki M. Analysis of surgical cases of tarsal tunner syndrome in our department: case series and literature review. Asian J Neurosurg. 2020;15(1):59-64.
5. Forsythe RO, Apelqvist J, Boyko EJ, Fitridge R, Hong JP, Katsanos K, Mills JL, et al. Effectiveness of revascularization of the ulcerated foot in patients with diabetes and peripheral artery disease: a systematic review. Diabetes Metab Res Ver. 2020;36(Suppl 1):e3279.
Acknowledgment: I thank Sebastian Cotofana, Division of Anatomy, Department of Medical Education, Albany Medical College, Albany, NY, USA.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}