


Cintia Navarro Lamas1; Fatima Maria de Oliveira Rabay1,2; Elisangela Manfredini Andraus de Lima1,2; Flávia Regina Ferreira1,2; Veridiana de Paula Santos Miranda1; Fernanda da Rocha Gonçalves3,4
Submitted on: 24/02/2023
Approved on: 10/05/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Lamas CN, Rabay FMO, Lima EMA, Ferreira FR, Miranda VPS, Gonçalves FR. Dermabrasion in exogenous ochronosis: a therapeutic option. Surg Cosmet Dermatol. 2023;15:e20230232.
Exogenous ochronosis is a stigmatizing dermatosis characterized by asymptomatic, bluish-black, or grayish macules in photoexposed areas. Associated with the prolonged use of hydroquinone for the treatment of dyschromias, it has a broad therapeutic arsenal, but the results are unsatisfactory and/or costly. We report the case of a female patient with histologically proven exogenous ochronosis who underwent dermabrasion associated with the use of tretinoin and topical corticosteroids with surprising results after three months of follow-up to demonstrate the possibility of therapeutic success with a low-cost technique and an outpatient clinic procedure.
Keywords: Ochronosis; Therapeutics; Dermabrasion
Exogenous ochronosis is a rare, acquired dermatosis restricted to the skin, of unknown incidence. Its most frequent cause is the indiscriminate use of hydroquinone to treat melasma.1-4 It is characterized by asymptomatic, bluish-black, or grayish macules in photoexposed areas.2,3,5 In its pathogenetic basis, proposed by Penneys, hydroquinone inhibits the homogentisic acid oxidase enzyme, leading to its deposition in the form of ochronotic pigment between dermal collagen fibers.2-5
Wirchow first named it in 1866, and later Pick (1906), Berddard and Plumtre (1912), and Findlay (1975) described it. Exogenous ochronosis predominates in the black population and preferentially affects the face, neck, upper back, and the limbs' extensor surface.1-3,5 It must be differentiated from endogenous ochronosis (alkaptonuria), an autosomal recessive metabolic disorder that presents articular and cardiovascular manifestations in addition to skin hyperpigmentation.1,4,5
In 1979, Dogliotti and Leibowitz classified it into three clinical stages: grade I – erythema and mild hyperpigmentation; grade II – pigmented colloid milium (caviar-like lesions) and some atrophy; and grade III – papulonodular lesions with or without inflammation.2,3,5
Its main risk factors are high phototypes, lack of photoprotection, and use of hydroquinone in concentrations >3% for more than six months.2,4 However, some cases report concentrations lower than 2% and time lower than six months.2-4 Furthermore, the condition can be caused by exposure to other substances such as antimalarials, phenol, resorcinol, and mercury, among others.1,5
The therapeutic arsenal is broad; however, the results are unsatisfactory and/or costly.3 Thus, the therapeutic success obtained with a low-cost technique and outpatient implementation motivated this report.
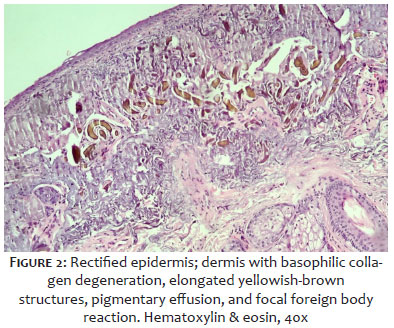
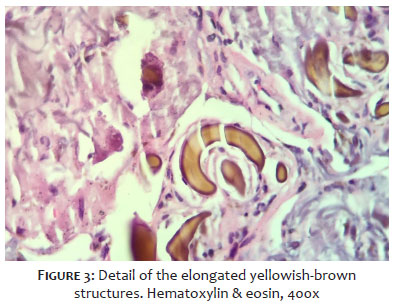
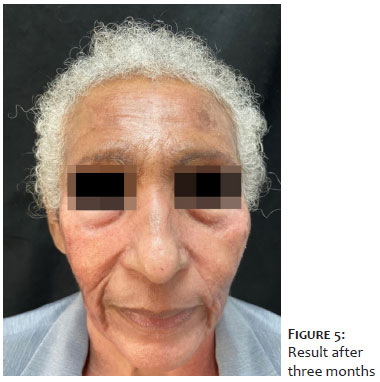
A 70-year-old woman, skin phototype IV, complained of “spots on her face for ten years”. Dermatological examination showed well-defined, hyperchromic macules with irregular edges, formed by the confluence of blackish-grayish pigmentation with follicular distribution, asymptomatic, on the face (frontotemporal, malar, and bilateral mandibular), and neck (Figure 1). She denied comorbidities and reported previous use of a formulation containing tretinoin and hydroquinone to treat melasma. Given the clinical picture, we made the diagnostic hypotheses of lichen planus pigmentosus, exogenous ochronosis, pigmented contact dermatitis, and toxic melanoderma. We performed an incisional biopsy at two points and prescribed topical dexamethasone associated with photoprotection. Histopathology showed rectified epidermis and dermis with basophilic collagen degeneration, elongated yellowish-brown structures, pigmentary spillage, and focal foreign body reaction in both samples (Figures 2 and 3). These findings associated with the skin condition and the absence of systemic manifestations concluded the diagnosis of exogenous ochronosis. The patient underwent dermabrasion with water sandpaper in the affected facial area (Figure 4), associated with the use of a nighttime topical formulation containing 0.05% desonide, 0.01% tretinoin, and 2% alpha-bisabolol, in addition to photoprotection. After three months, there was significant lightening (Figure 5). The patient is undergoing out-patient follow-up and maintains the results.
The method used was manual dermabrasion with water sandpaper. We used anesthesia with 2% lidocaine solution and vasoconstrictor, diluted in saline solution (5 ml and 15 ml, respectively), plus 8.4% sodium bicarbonate (0.5 ml) to minimize application pain and promote considerable hemostasis, allowing better visualization of the degree of injury to the treated tissue. The sandpaper used was 120 and 280, starting with 120 (thicker and rougher). The sandpapers were immersed in saline solution in a dome before use. We also used a 3 ml syringe, a suitable diameter for adapting and holding the sandpaper concerning the operator. Dermabrasion involves back-and-forth movements in all directions until intense dermal bleeding dew and lightening of the ochronotic pigment are observed. Around the treated area, more superficial dermabrasion must be performed to avoid a marked difference regarding normal skin.
Although infrequent, exogenous ochronosis is a dermatosis that negatively impacts the quality of life of the affected individual since its characteristics and locations can interfere with self-esteem. The differential diagnosis includes melasma, endogenous ochronosis, argyria, pigmented lichen planus, bilateral nevus of Ota, Riehl melanosis, and post-inflammatory or drug-induced hyperpigmentation, such as amiodarone and minocycline.1,4,5
Histopathological confirmation is mandatory, showing pigmentary effusion, solar elastosis, banana-shaped yellow-brown fibers in the papillary dermis, and the eventual presence of collagen degeneration, colloid milium, and granulomas.1-4 Dermoscopy can corroborate the diagnosis, showing irregular structures, globular, annular, or arciform, grayish-brown, distributed throughout the lesion and obliterating the follicular openings.4,5,6
The therapeutic arsenal is broad, comprising photoprotection associated with acids, depigmenting agents, topical corticosteroids, dermabrasion, and lasers, but with results considered unsatisfactory and/or costly.3
Tretinoin, effective in some cases, produced transient hyperpigmentation in some patients.7 The association of photoprotection with topical corticosteroids, as well as the use of cryotherapy, showed variable results.7,8 The oral use of tetracycline in lesions with a sarcoid appearance led to complete resolution after three months.7 Lasers such as CO2, QS ruby 694 nm, QS alexandrite 755 nm, and Nd: YAG 1064 nm show promising technologies, with good results in the literature.7-9
Trichloroacetic acid (TAA) is mentioned as ineffective in treating ochronosis. However, França et al. used 20% TAA peelings as adjuvant therapy, achieving regression of the lesions. Nevertheless, in this case, several methods/ technologies (QS Nd: YAG laser, CO2 laser, microdermabrasion, intense pulsed light [IPL], and TAA 20% peel) were used and certainly had an impact on the final result.7 In the report by Ceglio et al., different therapeutic modalities such as QS Nd: YAG laser and 10,600 nm fractional CO2 laser, including IPL, were also associated with success. Care must be taken with patients with high skin phototypes (above IV) due to the risk of dyschromia.8
Dermabrasion is a technique that removes superficial layers of the skin and aims to initiate re-epithelialization and healing. Its clinical use in various conditions, such as scars, blemishes, and facial rejuvenation, has decreased substantially in recent years with the development of the new technologies mentioned above. However, dermabrasion successfully treated a variety of medical conditions in the past.10,11 Its first indications were described by Hanke et al., summarized as follows: acne scars, actinic keratoses, sebaceous adenoma, keloids, lichen, nevi, seborrheic keratosis, tattoos, traumatic scars, and rhytids.10,11 Other studies have also shown the success of its use in idiopathic guttate hypomelanosis, vitiligo, and after Mohs micrographic surgery for better aesthetic and functional results.12-15
Few reports in the literature demonstrate dermabrasion as an option to treat exogenous ochronosis. Diven et al. used a combination of dermabrasion and ablative CO2 laser with satisfactory results in the periorbital and nasal regions of a woman with a high skin type.6 In the present report, dermabrasion alone with sandpaper, a low-cost technique performed on an outpatient basis, showed significant improvement in this condition and, consequently, the patient's quality of life.
We conclude by highlighting the need for new studies that reproduce this result and corroborate this indication/technique. We also alert the dermatologist about the importance of reconsidering the diagnosis of refractory melasma.
Cintia Navarro Lamas
ORCID: 0000-0003-4092-4921
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; critical literature review.
Fatima Maria de Oliveira Rabay
ORCID: 0000-0003-3709-5819
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Elisangela Manfredini Andraus de Lima
ORCID: 0000-0002-2390-0410
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Flávia Regina Ferreira
ORCID: 0000-0001-5679-4282
Approval of the final version of the manuscript; preparation and writing of the manuscript; effective participation in research orientation; critical review of the manuscript.
Veridiana de Paula Santos Miranda
ORCID: 0000-0002-5360-9640
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; effective participation in research orientation; critical literature review; critical review of the manuscript.
Fernanda da Rocha Gonçalves
ORCID: 0000-0003-2933-2845
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Qorbani A, Mubasher A, Sarantopoulos GP, Nelson S, Fung MA. Exogenous Ochronosis (EO): skin lightening cream causing rare caviar-like lesion with banana like pigments; review of literature and histological comparison with endogenous counterpart. Autops Case Rep [Internet]. 2020;10(4):e2020197.
2. Martins VMR, Sousa ARD, Portela NC, Tigre CAF, Goncalves LMS, Castro Filho RJL. Ocronose exógena: relato de caso e revisão da literatura. An Bras Dermatol. 2012;87(4):633-6.
3. Ribas J, Schettini APM, Cavalcante MSM. Ocronose exógena induzida por hidroquinona: relato de quatro casos. An Bras Dermatol. 2010;85(5):699-703.
4. Ko WL, Wang KH. Exogenous ochronosis. Dermatol Sin. 2015;33(1):29-30.
5. Sánchez-Martínez EM, García-Briz MI, Moneva-Lêniz LM, Gegúndez-Hernández H, Pose-Lapausa P, Mateu-Puchades A. Exogenous ochronosis: the failure of depigmenting creams. Dermatol Online J. 2019;25(4):13030/qt5vd7h6xc.
6. Carvalho CGS, Vilela VN, Rocha AEA, Carvalho GSM, França ER, Rodrigues AGA. Ocronose exógena tratada com laser de CO2. Surg Cosmet Dermatol. 2016:8(4):370-2.
7. França ER, Paiva V, Toscano LPN, Rodrigues TFA. Ocronose exógena: relato de caso. Surg Cosmet Dermatol. 2010;2(4)319-21.
8. Ceglio WW, Careta MF, Patriota R, Torezan LA. Exogenous ochronosis successfully treated with the combination of intense pulsed light and fractional CO2 laser. An Bras Dermatol. 2023;98(1):138-40.
9. Torraca PFS, Sandini EM, Freitas TCM. Uso de tecnologias a laser e luz intensa pulsada no tratamento da ocronose exógena: uma revisão da literatura. Surg Cosmet Dermatol. 2021;13:e20210002.
10. Hanke CW, O'Brian JJ, Solow EB. Laboratory evaluation of skin refrigerants used in dermabrasion. J Dermatol Surg Oncol. 1985;11(1):45-9.
11. El-Musa KA, Shehadi RS, Shehadi S. Extensive facial adenoma sebaceum: successful treatment with mechanical dermabrasion: case report. Br J Plast Surg. 2005;58(8):1143-7.
12. Dhotre AP, Singh SP, Madke B, Singh A, Jawade S. A comparison of the efficacy of 50% trichloroacetic acid (TCA) application and dermabrasion in patients with idiopathic guttate hypomelanosis (IGH): a pilot study. Iranian J Dermatol. 2020;23(4):142–49.
13. Campbell RM, Harmon CB. Dermabrasion in our practice. J Drugs Dermatol. 2008;7(2):124-8.
14. Tolkachjov SN, Harmon CB. How we do it: dermabrasion as a primary reconstruction option for nasal defects. Dermatol Surg. 2019;45(4):627-30.
15. Dev A, Vinay K, Kumaran MS, Bishnoi A, Srivastava N, Dogra S, et al. Electrofulguration-assisted dermabrasion is comparable to manual dermabrasion in patients undergoing autologous non-cultured epidermal cell suspension for treatment of stable vitiligo: a randomized controlled trial. J Cosmet Dermatol. 2022;21(4):1574-81.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}