


Maria Fernanda R. Gavazzoni Dias1; Nadia El-Kadi2; Ludmila Auzier Bentes Novais1; Enoi Vilar2; Paulo R. B. Fontinha3; Luisa V. Aarão Reis3; Justyna Sicinska4; Chloe Ekelem5
Conflict of interest: None.
Submitted on: 23/02/2023
Financial support: None.
Approved on: 07/08/2023
How to cite this article: Dias MFRG, El-Kadi N, Novais LAB, Vilar E, Fontinha PRB, Reis LVA et al. Alopecia areata after DRESS syndrome with a rapid resolution. Surg Cosmet Dermatol. 2023;15:e20230231.
Anagen effluvium (AE) is a hair growth disorder that occurs due to a disturbance in the hair follicle cycling. The most common cause of AE is alopecia areata (AA). Autoimmune diseases like AA may develop after drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome and are usually long-standing conditions. We report the case of a 17-year-old woman who developed a severe and abrupt AE after DRESS syndrome with a full and rapid recovery after two months of topical minoxidil.
Keywords: Alopecia; Alopecia Areata; Drug Hypersensitivity Syndrome; Case Reports
Anagen effluvium (AE) is a diffuse, non-scarring alopecia characterized by the loss of anagen hairs as an acute insult result. The most common cause of AE is alopecia areata (AA). Drug reaction with eosinophilia and systemic symptoms (DRESS) presents with severe skin rash, fever, lymphadenopathy, and multiple organ involvement. Autoimmune diseases, such as AA, can manifest after DRESS syndrome and, in general, present long-lasting signs and symptoms.1 The mechanisms of this condition are not fully understood, and the development of autoimmune disorders after DRESS syndrome involves the activation of T lymphocytes, with possible viral reactivation.2
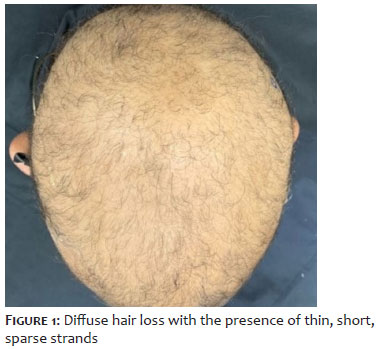
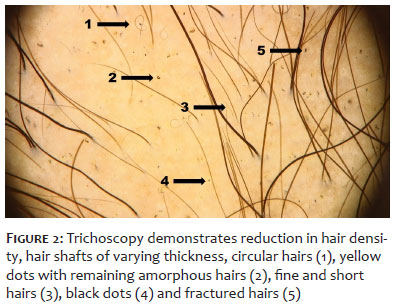
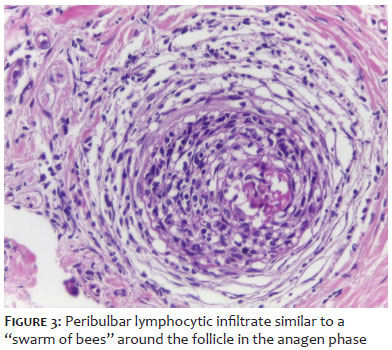
A 17-year-old woman was admitted to the hospital due to DRESS syndrome caused by the use of amoxicillin with potassium clavulanate. She received systemic corticosteroids, plasmapheresis, and cyclophosphamide. The patient was discharged after the resolution of the condition, using only prednisone 5 mg daily, suspended after a week. Ten days after hospital discharge, the patient presented extensive AE (Figure 1). Trichoscopy revealed diffuse capillary rarefaction, black dots, yellow dots, and dystrophic anagens (Figure 2). The scalp biopsy demonstrated a peribulbar lymphocytic infiltrate, supporting the diagnosis of AA (Figure 3). After two months of using topical minoxidil without systemic treatment, the patient showed complete hair recovery and no longer had signs of disease activity (Figure 4).
AE is a consequence of an autoimmune inflammatory process against the hair follicle bulb in the anagen phase, which interrupts the follicle's mitotic activity. This phenomenon is primarily observed in cases of AA.1
Autoimmune diseases, such as graft versus host disease, hemolytic anemia, vitiligo, alopecia areata, systemic lupus erythematosus, thyroid diseases, type 1 diabetes mellitus, rheumatoid arthritis, and hypersensitivity to new drugs, may develop after the resolution of DRESS syndrome.3 Cases of AA that occur after DRESS syndrome are, in general, long-lasting (Table 1).4,5,2,6,7,7,8
The reaction to drugs alone could represent a breakdown in the immune system's tolerance and be a risk factor for autoimmunity development. DRESS syndrome can be considered as part of an autoimmune spectrum.3
AA and DRESS syndrome are conditions mediated by T lymphocytes, possibly of autoimmune origin, whose mechanisms are not fully understood. The development of autoimmune diseases after the cure of DRESS syndrome may be related to the change in the expression of regulatory T lymphocytes (Tregs) and a gradual loss of function of these lymphocytes.9
Well-known factors in the development of AA, such as immune privilege collapse, genetic inheritance, the role of the ULBP genes and the ULBP3 and NKG2D receptors, and innate and acquired immunity involvement, also appear to participate in the pathophysiogenesis of DRESS syndrome.9,10
The episode of hair loss described in our patient occurred just one month after the development of DRESS syndrome and was quickly resolved with topical minoxidil as monotherapy. To our knowledge, this is the first case report describing rapid recovery from AA triggered after DRESS syndrome resolution.
The reported case illustrates the development of AA, an autoimmune disease, after DRESS syndrome resolution. We describe for the first time a patient who had complete and rapid AA resolution using only topical treatment. The immunological mechanism involved remains to be elucidated.
Maria Fernanda Reis Gavazzoni Dias
ORCID: 0000-0001-7397-7478
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Nadia El-Kadi
ORCID: 0000-0003-1172-4963
Preparation and writing of the manuscript; collecting, analyzing and interpreting data; critical literature review.
Ludmila Auzier Bentes Novais
ORCID: 0000-0002-4759-5051
Preparation and writing of the manuscript; collecting, analyzing and interpreting data; critical literature review.
Enoi Vilar
ORCID: 0000-0001-8069-2104
Critical review of the manuscript.
Paulo R. B. Fontinha
ORCID: 0000-0002-5192-839X
Collecting, analyzing, and interpreting data.
Luisa V. Aarão Reis
ORCID: 0000-0002-6138-2677
Collecting, analyzing, and interpreting data.
Justyna Sicinska
ORCID: 0000-0002-7907-2837
Author's contribution: Critical review of the manuscript.
Chloe Ekelem
ORCID: 0000-0002-7919-6901
Critical review of the manuscript.
1. Kanwar AJ, Narang T. Anagen effluvium. Indian J Dermatol Venereol Leprol. 2013;79(5):604–12.
2. Hollingsworth P, Paci K, Evans M, Miedema J, Morrell DS. Alopecia universalis after drug reaction with eosinophilia and systemic symptoms (Dress). Pediatr Dermatol. 2020;37(5):947–9.
3. Sasidharanpillai S, Joseph AT, Ajithkumar K, Devi K. Autoimmune diseases, end organ dysfunction and adverse drug reaction following drug reaction with eosinophilia and systemic symptoms (DRESS): a retrospective cohort study. Indian Dermatol Online J. 2021;12(5):722-5.
4. Chen YC, Chang CY, Cho YT, Chiu HC, Chu CY. Long-term sequelae of drug reaction with eosinophilia and systemic symptoms: a retrospective cohort study from Taiwan. J Am Acad Dermatol. 2013;68(3):459–65.
5. Ushigome Y, Kano Y, Ishida T, Hirahara K, Shiohara T. Short- and long-term outcomes of 34 patients with drug-induced hypersensitivity syndrome in a single institution. J Am Acad Dermatol. 2013;68(5):721–8.
6. Morita C, Yanase T, Shiohara T, Aoyama Y. Aggressive treatment in paediatric or young patients with drug-induced hypersensitivity syndrome (DiHS)/drug reaction with eosinophilia and systemic symptoms (DRESS) is associated with future development of type III polyglandular autoimmune syndrome. BMJ Case Rep. 2018;2018:bcr2018225528.
7. Lan J, Lahoti A, Lew DB. A severe case of minocycline-induced DRESS resulting in liver transplantation and autoimmune sequelae. Ann Allergy Asthma Immunol. 2016;116(4):367–8.
8. Kano Y, Sakuma K, Shiohara T. Sclerodermoid graft-versus-host disease-like lesions occurring after drug-induced hypersensitivity syndrome. Br J Dermatol. 2007;156(5):1061–3.
9. Shiohara T, Mizukawa Y. Drug-induced hypersensitivity syndrome (DiHS)/drug reaction with eosinophilia and systemic symptoms (DRESS): an update in 2019. Allergol Int. 2019;68(3):301–8.
10. Speiser JJ, Mondo D, Mehta V, Marcial SA, Kini A, Hutchens KA. Regulatory T-cells in alopecia areata. J Cutan Pathol. 2019;46(9):653–8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}