


Vítor Cercal de Oliveira1; Mariana M. Morita1; Hélio Amante Miot2
Financial support: This study received funding from FAPESP (2020/01455-5 and 2020/01953-5).
Conflict of interest: None.
Clinical trial: RBR-8tkx2dp / Ethics committee number: 3.826.868
Submitted on: 30/01/2023
Approved on: 21/02/2023
How to cite this article: Oliveira VC, Morita MM, Miot HA. Cryosurgery with liquid nitrogen combined with trichloroacetic acid 90% is not superior to individualized interventions in the treatment of anogenital warts. Surg Cosmet Dermatol. 2023;15:e20230217.
INTRODUCTION: Many options for anogenital warts (AGWs) treatment are available. Recently, trichloroacetic acid (TAA) and liquid nitrogen (LN) began to be associated to treat AGWs.
METHODS: Randomized, parallel, controlled clinical trial involving patients with penile AGWs. Patients were treated with LN, TAA, or their combination and reevaluated after 28 days.
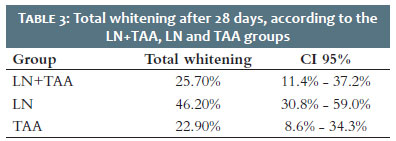
RESULTS: Among therapy with TAA, LN, and their combination, the clearance rate was 22.9% (95% CI: 8.6%-34.3%), 46.2% (95% CI: 30.8%-59.0%), and 25.7% (95% CI: 11.4%-37.2%), respectively.
DISCUSSION: All therapeutic options were effective. Though, there was no statistically significant difference between the groups.
Keywords: Nitrogen; Papillomavirus infections; Sexually transmitted diseases; Cryotherapy
Dear Editor,
Anogenital warts (AGW) are sexually transmitted infections (STIs) caused by the human papillomavirus (HPV), whose contagion is preferably sexual, and subtypes 6 and 11 are the most frequent.1,2 The primary therapies available for AGW are destructive ones, such as trichloroacetic acid (TAA) 80%-90%, cryosurgery with liquid nitrogen (LN) and electrocoagulation; and those for home clinical management, such as imiquimod and podophyllotoxin. A systematic review of clinical trials concluded that there was no robust evidence to establish a hierarchy between treatments, however, with superiority for destructive therapies over home treatments.3
Primary care frequently uses TAA and LN due to their accessible cost, practicality, and lower operational complexity. A randomized clinical trial compared the effectiveness of the two methods and showed no difference between them in terms of complete whitening of the lesions.4
Combining TAA and LN in the same treatment session is a strategy explored by gynecologists and dermatologists to approach AGWs. However, we lack clinical studies proving the effectiveness of this practice compared to the isolated use of these methods.
Between July/2020 and January/2022, an open, parallel, randomized clinical trial was conducted, involving men treated at the STIs outpatient clinic of the Clinics Hospital of the Medical School of de Botucatu-UNESP (HC-FMB/UNESP). This study aimed to compare the efficacy of LN versus TAA, or their combination, to treat AGWs. The Research Ethics Committee of the institution approved the project was approved by (nº 3.826.868), and the Brazilian Registry of Clinical Trials authorized its protocol ( https://ensaiosclinicos.gov.br/rg/RBR-8tkx2dp ).
Patients with AGWs on the penis, diagnosed by physical or acetoscopic examination by a certified dermatologist, were included. The study randomized the treatments used in each session as LN for 10 seconds, TAA 90%, or the association of both: TAA 90% followed by application of LN for 10 seconds.
The lesions were cataloged, and the patients were reassessed in 28 days to follow up on remaining lesions or complete bleaching. If they presented lesions in the reassessment, the patients were re-included in the study under new randomization.
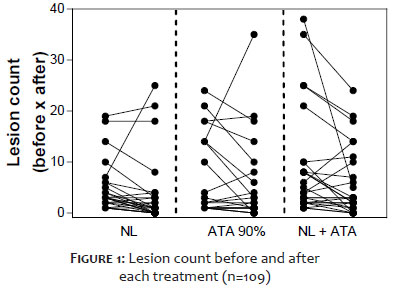
The study's primary outcome was the complete clearance of lesions on D28, compared between treatment groups using Fisher's exact test.5 Secondary outcomes were: a reduction in lesion count (Figure 1 and Table 1) and subgroup analysis of age, smoking status, immunosuppression status, and topography. Data were analyzed according to the protocol (per protocol), excluding cases that did not attend the D28 visit. A p-value <0.05 was considered significant.
The sample size was calculated to detect a complete clearance rate of the TAA+LN association 30% higher than that estimated for therapy with LN (25%) in one session, considering alpha 0.05 and power of 80%, resulting in the need for 38 treatments for each group.
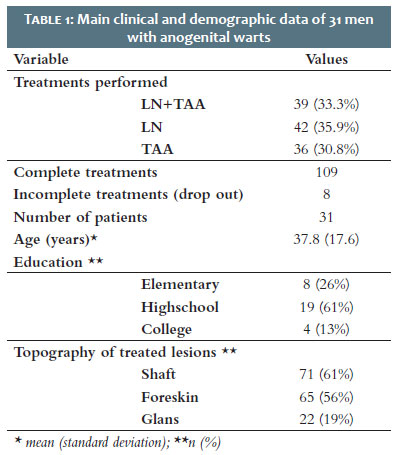
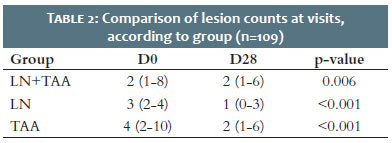
Table 1 shows the main clinical-demographic characteristics of the studied patients and the number of treatments performed. Tables 2 and 3 present the results of total whitening between groups. There was no difference between treatments in the rate of total whitening between groups (p=0.074) or for shaft or glans lesions (p>0.069). Furthermore, age group, immunosuppression, or smoking did not influence the total clearance at D28 (p=0.523).
The study has limitations because it is monocentric, depends on the clinical diagnosis of the lesions, does not quantitatively assess immunity, lost eight individuals to follow-up, and because the design does not allow intrapatient comparison of all treatments. However, these elements did not prevent the comparison of performance between groups.
In conclusion, there was no evidence of the superiority of the association between LN and TAA to treat AGWs. The choice of LN or TAA, or even the alternation of therapies, should follow clinical criteria.
Vítor Cercal de Oliveira
ORCID: 0000-0001-6823-491X
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Mariana M. Morita
ORCID: 0000-0002-6396-7388
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Hélio Amante Miot
ORCID: 0000-0002-2596-9294
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Leto Md, Santos Júnior GF, Porro AM, Tomimori J. Human papillomavirus infection: etiopathogenesis, molecular biology and clinical manifestations. An Bras Dermatol.;86(2):306-17.
2. Sociedade Brasileira de Dermatologia; Miot HA, Penna GO, Ramos AMC, Penna MLF, Schmidt SM, et al. Profile of dermatological consultations in Brazil (2018). An Bras Dermatol. 2018;93(6):916-28.
3. Bertolotti A, Milpied B, Fouéré S, Dupin N, Cabié A, Derancourt C. Local management of anogenital warts in non-immunocompromised adults: a systematic review and meta-analyses of randomized controlled trials. Dermatol Ther (Heidelb). 2019;9(4):761-74.
4. Morita MM, Marcondes TSP, Haddad V, Miot HA. Cryosurgery with liquid nitrogen versus trichloroacetic acid in the treatment of human papillomavirus (HPV) penile wart: a randomized controlled trial. Surg Cosmet Dermatol. 2021;13:e20210041.
5. Miola AC, Miot HA. Comparing categorical variables in clinical and experimental studies. J Vasc Bras. 2022;21:e20210225.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}