


Juliana Tortajada; Talita Itoh Ferdinandi; Marina Riedi Guilherme; Ligia Márcia Mário Martin; Cássio Rafael Moreira
Financial support: None.
Conflict of interest: None.
Submitted on: 17/01/2023
Approved on: 07/03/2023
How to cite this article: Tortajada J, Ferdinandi TI, Guilherme MR, Martin LMM, Moreira CR. Aneurysmal dermatofibroma with exuberant presentation. 2023;15:e20230216.
Aneurysmal dermatofibroma (ADF) is a rare benign tumor originating in the dermis. It is most common in the lower limbs of women over 30 years. Its etiology is unknown, and histopathological examination confirms the diagnosis. This paper presents a case of ADF with an exuberant presentation in a young female patient with a pedunculated tumor in the right pretibial region, measuring 12 cm in greatest diameter. This report aims to demonstrate an infrequent variant of dermatofibroma with significant growth and emphasize the importance of lesion excision and follow-up because of the high recurrence rate.
Keywords: Histiocytoma, Benign fibrous; Dermatology; Dermoscopy
Dermatofibromas (DF) are common benign tumors originating in the dermis and may extend to the subcutaneous tissue. They are more frequent in the trunk and extremities of young adults, with a predominance in women from the third decade of life.1
Considering clinical and histopathological characteristics, DF is classified into multiple variants that include aneurysmal, hemosiderotic, cellular, epithelioid, atypical, lipidized, clear cell, palisading, atrophic, keloidal, granular cell, myxoid, lichenoid, among others. Thus, the diagnosis can be challenging.2,3
Aneurysmal dermatofibroma, also known as aneurysmal benign fibrous histiocytoma, is an uncommon form representing 1% to 7% of cases.2 Santa Cruz et al. first described it as an "aneurysmal fibrous histiocytoma".4 It is a rare variant of cutaneous fibrous histiocytoma that results from the proliferation of blood vessels and hemorrhage in a fibrous histiocytoma.5 It has an unknown etiology. Several authors have noted a correlation with the extravasation of red blood cells in the vascular wall due to repeated microtraumas that dissect the tumor area forming fissures and resulting in hemosiderin phagocytosis by tumor cells.1
A 24-year-old woman, skin phototype III, was referred from primary health care because of a tumor in the right leg due to a history of a papule in the right distal pretibial region for ten years. The lesion was asymptomatic, with progressive growth, mainly after a twin pregnancy in 2019.
Physical examination revealed a pedunculated tumor in the right pretibial region, measuring 10x12 cm (Figure 1), with a positive transillumination test (Figure 2).
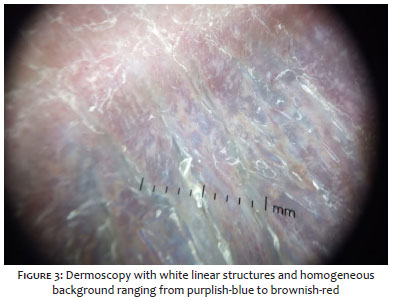
Dermoscopy showed white linear structures and a homogeneous background ranging from blue-purplish to red-brown (Figure 3).
An excisional biopsy was performed with primary closure of the surgical wound.
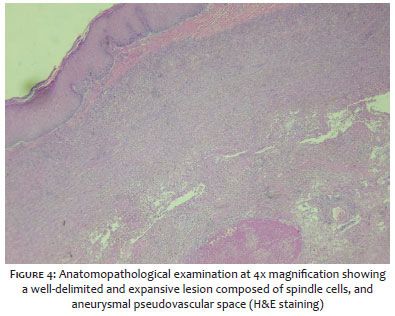
The anatomopathological study revealed a well-defined benign neoplasm with expansive borders, characterized by fibrohistiocytic proliferation without atypia, exhibiting collagen entrapment in the periphery and dilated and congested capillaries, with extravasation of red blood cells and numerous hemosiderophages, accompanied by the formation of aneurysmal pseudovascular spaces with fibrinohematic material (Figures 4 and 5). Fluid drain cytology was negative for neoplastic cells.
DF usually presents clinically as a papule, nodule, or erythematous brownish or violaceous tumor. The aneurysmal type is a rare variant occurring in less than 2% of DF. It is larger than the classic DF, and it can be painful due to intralesional hemorrhages, causing discomfort to the patient and reduced quality of life.1,6,7 Studies show a predilection for lower limbs (55%), followed by upper limbs (17%), trunk (12%), and head and neck (4%).8
Dermoscopy can find known DF patterns. However, the characteristics that suggest aneurysmal DF are white linear structures, brown or purplish background, vascular structures, and a delicate pigmented network in the periphery.9
Aneurysmal dermatofibroma is challenging to diagnose due to its rarity, morphological heterogeneity, inconsistent immunological profile, and overlap with a wide spectrum of neoplastic and non-neoplastic, benign, and malignant entities.10 Its incidence may be underestimated due to overlapping histopathological findings.11
Histopathological examination confirms the diagnosis showing a dermal-based cellular nodule composed of intertwined fascicles of thin cells with peripheral collagen entrapment, spaces similar to central hemorrhagic cysts without endothelial lining, extracellular hemorrhage, and hemosiderin-laden macrophages.12
Regarding immunohistochemistry, spindle cells of dermatofibroma usually express factor XIII and are negative for immunostaining with S100 HMD45 and CD34.1,9
Imaging findings are nonspecific regarding its histogenesis. When originating from soft tissue, X-rays and CT scans show a heterogeneous mass, possibly suggesting cystic and enhancement components. However, they are ultimately inferior to MRI soft tissue detail.13
The differential diagnosis is made with hemosiderodic hemangioma, angiomatoid malignant fibrous histiocytoma, and melanoma, whose histological aspects are completely different. Other clinical differential diagnoses include papular, nodular, or plaque-like lesions of Kaposi sarcoma, angiosarcoma, and epithelioid fibrous histiocytoma.9,14
The treatment must be conducted with exeresis to differentiate it from malignant lesions. Surgical margins between three and 5 mm are recommended.1
The disease prognosis is favorable. Local recurrence after excision ranges from 2% to 10%, and the chance of metastasis is less than 1%.15,16
Therefore, the exeresis of the lesions is indicated for diagnostic clarification, and the patient follow-up must be conducted frequently due to the possibility of recurrence.
Juliana Tortajada
ORCID: 0000-0002-2255-2039
Study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Talita Itoh Ferdinandi
ORCID: 0000-0003-0085-755X
Preparation and writing of the manuscript; critical literature review.
Marina Riedi Guilherme
ORCID: 0000-0003-4765-2180
Preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Ligia Márcia Mário Martin
ORCID: 0000-0002-2143-679X
Critical literature review.
Cássio Rafael Moreira
ORCID: 0000-0002-8781-1505
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
1. Pegas JR, Santos BAC, Prado IDF, Tebcherani AJ, Cade KV. Dermatofibroma aneurismático. Surg Cosmet Dermatol 2010;2(2):225-7.
2. Zaballos P, Llambrich A, Ara M, Olazarán Z, Malvehy J, Puig S. Dermoscopic findings of haemosiderotic and aneurysmal dermatofibroma: report of six patients. Br J Dermatol. 2006;154(2):244-50.
3. Curcó N, Pagerols X, García M, Tarroch X, Vives P. Atrophic dermatofibroma accompanied by aneurysmatic characteristics. J Eur Acad Dermatol Venereol. 2006;20(3):331-3.
4. Santa Cruz DJ, Kyriakos M. Aneurysmal ("angiomatoid") fibrous histiocytoma of the skin. Cancer. 1981;47(8):2053-61.
5. Calonje E, Fletcher CD. Aneurysmal benign fibrous histiocytoma: clinicopathological analysis of 40 cases of a tumour frequently misdiagnosed as a vascular neoplasm. Histopathology. 1995;26(4):323-31.
6. Kawakami Y, Oyama N, Nishibu A, Nakamura K, Kaneko F. A case of 'giant' aneurysmal benign fibrous histiocytoma. Clin Exp Dermatol. 2006;31(3):456-7.
7. Venkataraman G, Hammadeh R. Report of an angiosarcoma mimic: cutaneous aneurysmal fibrous histiocytoma. APMIS. 2006;114(10):744-8.
8. Luzar B, Calonje E. Cutaneous fibrohistiocytic tumours - an update. Histopathology. 2010;56(1):148-65.
9. Carvalho RM, Botarelli T, Rodrigues NCS, Costa JM. Dermatoscopia do dermatofibroma aneurismático: relato de dois casos. Surg Cosmet Dermatol. 2020;12(S2):159-62.
10. Thway K, Gonzalez D, Wren D, Dainton M, Swansbury J, Fisher C. Angiomatoid fibrous histiocytoma: comparison of fluorescence in situ hybridization and reverse transcription polymerase chain reaction as adjunct diagnostic modalities. Ann Diagn Pathol. 2015;19(3):137-42.
11. Antonescu CR, Dal Cin P, Nafa K, Teot LA, Surti U, Fletcher CD, et al. EWSR1-CREB1 is the predominant gene fusion in angiomatoid fibrous histiocytoma. Genes Chromosomes Cancer. 2007;46(12):1051-60.
12. Santa Cruz DJ, Kyriakos M. Aneurysmal ("angiomatoid") fibrous histiocytoma of the skin. Cancer. 1981;47(8):2053-61.
13. Bauer A, Jackson B, Marner E, Gilbertson-Dahdal D. Angiomatoid fibrous histiocytoma: a case report and review of the literature. J Radiol Case Rep. 2012;6(11):8-15.
14. Wood KA, Easson AM, Ghazarian D, Saeed Kamil Z. Metastatic aneurysmal fibrous histiocytoma in a 20-year-old woman: A rare case report with review of the literature and discussion of its genomic features. J Cutan Pathol. 2020;47(9):870-5.
15. Rani D, Gupta A, Gupta A, Rastogi K. Cytological diagnosis of angiomatoid fibrous histiocytoma: Report of a case and review of literature. Diagn Cytopathol. 2021;49(1):E36-E39.
16. Antonescu CR, Rossi S. Angiomatoid fibrous histiocytoma. In: Fletcher CD, Bridge JA, Hogedoorn PC, Mertens F, eds. World Health Organizaation (WHO) Classification of Tumours of Soft Tissue and Bone. Lyon: IARC Press; 2013. p. 204-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}