


Laura Areli Pérez-Campos1; Salvador Alonso Gutiérrez-Ávila2; Valerie Dafne Alcántara-Ramírez3; Daniel Oswaldo Dávila-Rodríguez4
Submitted on: 04/01/2023
Approved on: 12/02/2023
Financial support: None
Conflict of interest: None
How to cite this article: Pérez-Campos LA, Gutiérrez-Ávila SA, Alcántara-Ramírez VD, Dávila-Rodríguez DO. Extensive perianal pyoderma gangrenosum, diagnostic-therapeutic approach to a complicated patient. Case report and literature review. Surg Cosmet Dermatol. 2023;15:e20230211.
BACKGROUND: Pyoderma gangrenosum is a rare neutrophilic dermatosis with very low incidence and varied clinical presentation associated with different comorbidities. It is also a diagnostic-therapeutic challenge.
CLINICAL CASE: A 79-year-old woman presented 18 months of dermatosis evolution that began as a perianal pustule and progressed to a 20 cm in diameter ulcer. Due to her comorbidities, she received topic treatment with satisfactory evolution.
CONCLUSIONS: Pyoderma gangrenosum is frequently associated with a systemic disease. Consequently, it must be approached from a systemic perspective with the support of a multidisciplinary team to provide the most appropriate treatment.
Keywords: Pyoderma gangrenosum, Skin diseases, Peptic ulcer hemorrhage, Hypothyroidism
Pyoderma gangrenosum is a chronic inflammatory neutrophilic dermatosis characterized by single or multiple painful ulcers. It has varied clinic presentations depending on the infiltrated regions,1 and its approach continues to be an exclusion diagnosis.2 Its incidence is 3-10 patients per one million worldwide.3
Its etiology is complex, multifactorial, and still poorly understood. It involves genetic interaction, environmental factors, immune dysregulation, altered neutrophil chemotaxis, and keratinocyte apoptosis with molecular patterns release associated with damage.4
Underlying systemic diseases are present in up to 77% of cases.5 Inflammatory bowel disease, rheumatoid arthritis, and hematological malignancies, among others, are the more frequently associated diseases.2
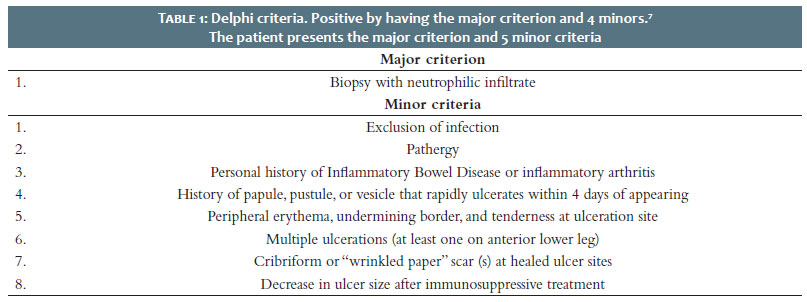
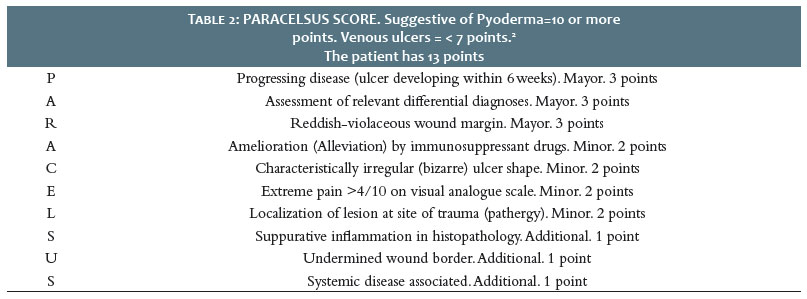
Five clinical variants make its diagnosis a challenge: classic (ulcerative), bullous, vegetative, pustular, and peristomal6. Therefore, Delphi criteria with 86% sensitivity and 90% specificity (Table 1)7and PARACELSUS score were recently defined to improve the diagnostic approach (Table 2).2
The pretibial area, peristomal skin, chest, hands, head, and neck are the primary skin location, and it is infrequent in the perianal area.8 Gulliver’s sign can clinically evaluate their therapeutic response due to epithelial growth in the ulcer edge towards the center, leaving cribriform scars.9
Histopathology of early lesions classically shows deep suppurative, follicular-centric inflammation, dense neutrophilic infiltrates, and leukocytoclastic vasculitis. Then, the mixed inflammatory infiltrate predominates with neutrophils and epidermal ulceration. However, it is an inconsistent finding, not pathognomonic.10
Regarding treatment, currently, no drug has been approved by the Food and Drug Administration (FDA). Traditional therapies include corticosteroids and other immunosuppressants, either local or systemic. Recently, biological therapies have become a trend.2 Nevertheless, there is lacking of scientific evidence from large clinical trials that assess safety, efficacy, adverse events, and outcomes.
Pyoderma gangrenosum is a rare disease,3-4 which makes it challenging to conduct large clinical trials and observational studies with adequate statistical significance. Hence, observational studies such as case reports, case series, and trials in reference centers, among other strategies, become relevant11 to evaluate the diagnostic-therapeutic approach, reporting their outcomes toward establishing records to provide the basis for future extended review development.
Therefore, we report a case of extensive perianal pyoderma gangrenosum in the presence of gastrointestinal bleeding secondary to duodenal ulcer and hypothyroidism, highlighting the importance of an individualized diagnostic-therapeutic approach based on comorbidities and clinical history.
A 79-year-old woman referred from the first level of care through a diagnosis of ulcer disease with a history of primary hypothyroidism, systemic arterial hypertension, acid peptic disease, hemorrhoidal disease, and bilateral knee osteoarthritis associated with the chronic use of nonsteroidal anti-inflammatory drugs for one year.
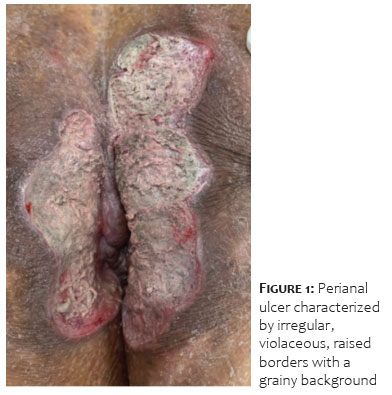
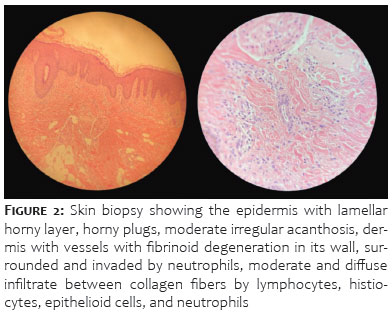
On physical examination, she presented a localized dermatosis in the perianal region consisting of a 20 cm approximately ulcer with undermined and erythematous- violaceous edges with fibrinous tissue associated. The condition started 18 months before the patient’s admission with a pustule that progressed to a painful ulcer (Figure 1). She went to a dermatologist, who performed a skin biopsy, which reported leukocytoclastic vasculitis. (Figure 2) Upon admission to the hospital, the patient presented pale skin and low cardiac output data. She was admitted to the internal medicine service, protocolized, and treated by the endoscopy service for suspected inflammatory bowel disease. However, they observed digestive bleeding secondary to a duodenal ulcer.
Pyoderma gangrenosum treatment started based on a high-potency topical steroid (clobetasol) due to the contraindication of systemic therapy, and the patient demonstrated improvement of the condition.
After a 2-month follow-up, the patient did not present any recurrence, with a complete lesion healing after 30 days.
The researchers present a diagnostic-therapeutic approach to rare pyoderma gangrenosum location associated with comorbidities. Based on the Delphi and PARACELSUS scores, we established the diagnosis, which is currently internationally accepted, generating homogeneity when reporting the results and reducing the diagnostic-therapeutic approach. However, future studies of greater statistical relevance are required.
The association with hypothyroidism and pyoderma gangrenosum is new in the medical literature, and it was recently added to its list of systemic associations. Thus, it should receive special attention in future reviews since it is relevant to the disease pathophysiology and its relationship with the decrease in collagen and hydroxyproline in wounds during the inflammatory and the proliferative phase, we emphasize the maintenance of endocrinological control to improve healing conditions.11 Therefore, we emphasize maintaining endocrinological control to improve healing conditions. However, more scientific evidence should be available regarding relationships and clinical results.
Regarding treatment, in localized forms, topical therapy has shown an excellent response.12 A prospective study assessed topical tacrolimus 0.03% and clobetasol 0.05% and observed that 44.8% of individuals presented a response at six months, 33% required systemic treatment, and 15% had recurrent disease.13 We opted for clobetasol only, considering that steroids increase the risk of bleeding or perforation in hospitalized patients,14 and we observed improvement of the lesion in a 3-month follow-up.
Recently, in an updated literature review, the researchers proposed a treatment algorithm based on evidence-based medicine.15 The study points out that an ulcer ≥3 cm, ≥3 lesions, or ≥5% body surface involvement is classified as a mild disease and proposes that these patients receive treatment for pain and topical therapy, leaving the systemic therapy for those with moderate or severe disease or with a contraindication for this treatment, as is the case of the presented patient.
Finally, no international guidelines assess the results in patients with comorbidities contraindicating the use of systemic and biological therapies. Thus, it justifies the topical treatment, and the clinical result was favorable. The preceding may form the basis for future reviews and research projects focused on topical therapy in a complicated patient with a contraindication to systemic treatment.
This article has well-established limitations, as it is a case report, so the results presented here should be considered carefully. However, the researchers adequate the paper to international guidelines (CARE), thus increasing its internal validity. On the other hand, using this resource acquires epidemiological relevance in rare diseases such as this case.11
Pyoderma gangrenosum is a neutrophilic dermatosis with a diagnostic-therapeutic challenge, notwithstanding that there are few clinical studies due to the low prevalence of the disease, leading to the limited information or little statistical relevance on the clinical outcome and response to treatment. On the other hand, the literature still has not reported pyoderma gangrenosum in the perianal area in the presence of multiple comorbidities. The recent standardization of diagnostic criteria is a tool that can facilitate timely diagnosis and treatment to avoid the risk of developing squamous cell carcinoma.16
It is frequently associated with a systemic disease, so it must be approached from a systemic perspective with the support of a multidisciplinary team to provide the best treatment.
Patient perspective: “During my hospitalization, multiple specialties assessed each of my diseases to give appropriate and individualized treatment to my case. I went to several doctors for more than a year; however, it was not until this last hospitalization that I improved.
Laura Areli Pérez-Campos
ORCID:0000-0003-4806-1980
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Salvador Alonso Gutiérrez-Ávila
ORCID: 0000-0003-2586-2099
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Valerie Dafne Alcántara-Ramírez
ORCID: 0000-0003-1336-4949
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Daniel Oswaldo Dávila-Rodríguez
ORCID: 0000-0001-7691-4413
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Wallach D, Vignon-Pennamen MD. From acute febrile neutrophilic dermatosis to neutrophilic disease: forty years of clinical research. J Am Acad Dermatol. 2006;55(6):1066-71.
2. Goldust M, Hagstrom EL, Rathod D, Ortega-Loayza AG. Diagnosis and novel clinical treatment strategies for pyoderma gangrenosum. Expert Rev Clin Pharmacol. 2020;13(2):157-61.
3. Acosta-García J, Aguilar-García CR. Pioderma gangrenoso. Med Int Méx. 2014;30(5):92-8.
4. Ahn C, Negus D, Huang W. Pyoderma gangrenosum: a review of pathogenesis and treatment. Expert Rev Clin Immunol. 2018;14(3):225-33.
5. Martínez MZ, Enciso EM, Vázquez P. Gangrenous pyoderma associated to autoinmune hepatitis and thyroid disease. Med Int Méx 2022;38(1):185-92.
6. Ahronowitz I, Harp J, Shinkai K. Etiology and management of pyoderma gangrenosum: a comprehensive review. Am J Clin Dermatol. 2012;13(3):191-211.
7. Maverakis E, Ma C, Shinkai K, Fiorentino D, Callen JP, Wollina U, et al. Diagnostic criteria of ulcerative pyoderma gangrenosum: a delphi consensus of international experts. JAMA Dermatol. 2018;154(4):461-6.
8. Wollina U. Clinical management of pyoderma gangrenosum. Am J Clin Dermatol. 2002;3(3):149-58.
9. Landis ET, Taheri A, Jorizzo JL. Gulliver's sign: a recognizable transition from inflammatory to healing stages of pyoderma gangrenosum. J Dermatolog Treat. 2015;26(2):171-2.
10. Natori J, Shimizu K, Nagahama M, Tanaka S. The influence of hypothyroidism on wound healing. An experimental study. Nihon Ika Daigaku Zasshi. 1999;66(3):176-80.
11. Fregni F, Illigens B. Critical thinking in clinical research applied theory and practice using case studies. New York: Oxford University Press; 2018.
12. Bertoló MS, Ruiz M, Contreras C. Pioderma gangrenoso : excelente respuesta a tratamiento tópico . Rev Med Chil. 2015;143(1):130- 131.
13. Thomas KS, Ormerod AD, Craig FE, Greenlaw N, Norrie J, Mitchell E, et al. Clinical outcomes and response of patients applying topical therapy for pyoderma gangrenosum: a prospective cohort study. J Am Acad Dermatol. 2016;75(5):940-9.
14. Narum S, Westergren T, Klemp M. Corticosteroids and risk of gastrointestinal bleeding: a systematic review and meta-analysis. BMJ Open. 2014;4(5):e004587.
15. Maronese CA, Pimentel MA, Li MM, Genovese G, Ortega-Loayza AG, Marzano AV. Pyoderma gangrenosum: an updated literature review on established and emerging pharmacological treatments. Am J Clin Dermatol. 2022;23(5):615-34.
16. Ahn C, Negus D, Huang W. Pyoderma gangrenosum: a review of pathogenesis and treatment. Expert Rev Clin Immunol. 2018;14(3):225-33.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}