


Sergio Schalka
Submitted on: 15/12/2022
Approved on: 27/02/2023
Financial support: None.
Conflict of interest: Sérgio Schalka acted as a consultant for the FQM Melora laboratory.
How to cite this article: Schalka S. Polypodium leucotomos extract in topical and oral photoprotection: ten years of Brazilian experience. Surg Cosmet Dermatol. 2023;15:e20230207.
Polypodium leucotomos extract was first described in the literature 55 years ago, demonstrating anti-inflammatory action in dermatoses such as vitiligo and psoriasis. It is currently available as an oral and topical photoprotection agent in more than 26 countries to prevent and treat dermatoses resulting from solar radiation, such as polymorphous light eruption, melasma, actinic keratoses, skin cancer, and photoaging, among others. In Brazil, ANVISA registered the patented Polypodium leucotomos extract in 2012. After 10 years of its launch, its recommendation by Brazilian dermatologists is well established and is presented in this review paper.
Keywords: Solar radiation; Sunscreening agents; Polypodium
Solar radiation is the primary environmental element that interacts with skin health, having a relevant acute and chronic biological effect. It can vary significantly due to time, exposure intensity, professional and recreational activities, and, mainly, the phenotypic characteristics of individuals, namely their phototypes.1
Ultraviolet radiation (UVR), which represents about 10% of the total incident solar radiation, is the most active spectrum band from a photobiological point of view. Fraction B of ultraviolet radiation (UVB) is the most energetic radiation band that reaches us and, despite representing only about 0.5% of solar radiation, it is the main triggering agent of sunburn and skin cancer, in addition to having its main positive biological effect on the production of vitamin D.1
Fraction A of UVR (UVA) is about 20 times more available than UVB, representing approximately 9.5% of total UVR. Its main biological actions are directly or indirectly linked to the ability to generate reactive oxygen species (ROS), culminating in the clinical manifestations of pigmentation and aging, in addition to the photoimmunosuppressive potential as a contributing factor to the development of skin cancer and photodermatoses.1
Recently, the biological activity of non-ultraviolet radiation bands is better understood. Studies show that visible light (representing about 45% of solar radiation) stimulates the human retina making us see and also promotes skin pigmentation and ROS generation. Within visible light, the band comprised of violet and blue lights, also called high-energy visible (HEV) light, or simply blue light, is the most active, biologically speaking, and the main responsible for the pigmentary effect.2
Infrared radiation, in turn, represents about 45% of solar radiation and is the primary generator of heat. Recently, studies demonstrated that it is also a powerful ROS generator, interfering particularly in the photoaging process.1
Photoprotection can be defined as a set of measures to minimize the harmful effects resulting from sun exposure. In its broadest concept, it includes photoprotection education measures, the use of clothing and other mechanical protection, and regular use of topical and oral photoprotection.1
Among the photoprotective actives, besides the inorganic (physical) and organic (chemical) filters in topical sunscreens, there are biological filters. They may not interact directly with the incident radiation; however, they protect, orally or topically, cellular structures from damage caused by radiation.3
Polypodium leucotomos extract (PLE) is the best-studied and referenced photoprotective active in the international scientific literature. Its introduction in Brazil took place in 2012 after Anvisa approved an oral medication composed of Polypodium leucotomos extract (Helioral®, FQM Melora, RJ, Brasil) indicated to prevent photodermatoses, particularly polymorphous light eruption, and sunburn.
This study aims to review the main scientific publications and discuss the experience of using this drug ten years after its launch in Brazil.
Polypodium leucotomos is a tropical fern that belongs to the family Polypodiaceae.4
This plant, originally aquatic, evolved into a terrestrial form. To this end, it has naturally developed, in the evolutionary process, an enormous antioxidant capacity to protect its structures from solar radiation and other environmental effects.4
It and other ferns belonging to the same family have value in traditional medicine in South and Central America. The natives of these regions already recognized its anti-inflammatory properties, using them in infusions for oral consumption.5
The pharmacological use of Polypodium leucotomos began in the 1990s, when Gonzalez, Pathak, Fitzpatrick, and other researchers from the Harvard Medical School developed studies based on PLE using a patented hydrophilic extraction technology from the plant leaves (Fernblock®). They demonstrated the ability of the oral and topical use of this phytoextract to reduce sunburn and acute phototoxicity and immunosuppression reactions (Langerhans cells depletion) after sun exposure.6
Since then, the topical and oral use of the standardized extract of Polypodium leucotomos has become more frequent in different countries, initially in Europe and later in Asia and the Americas, as a photoprotective active due to its biological actions described below.
In Brazil, the medicine Helioral® was the first one registered in Anvisa, containing PLE and intended to prevent photodermatoses, particularly polymorphous light eruption to light and sunburn reactions, and photoimmunosuppression.
In addition to the oral route, PLE presents results when applied topically combined with physical and chemical filters.
After ten years of the Polypodium leucotomos extract introduction in Brazil, Brazilian dermatologists have gained experience in different clinical indications in office practice for dermatoses related to acute or chronic exposure to solar radiation.
*The correct nomenclature, defined by the “List of Common Brazilian Denominations” of the National Health Surveillance Agency (Anvisa), is Polypodium leucatomos. However, in the international scientific literature, the plant is called Polypodium leucotomos.
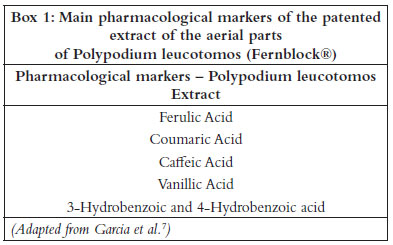
Unlike synthetic drugs, when we address actives that determine a well-defined pharmacological activity, in the botanical extracts evaluation we do talk about pharmacological markers (elements quantified by analytical methods related to the pharmacological properties of the plant and that must be controlled in the quality assurance process so that variations present in extraction batches do not interfere with the effectiveness and safety of the extract) rather than actives.7
For a phytoextract, it is more difficult to link a specific marker to a specific effect or mechanism of action. Thus, the set of these elements determines the extract action.7
Garcia et al. quantified, through analytical techniques, which are the main pharmacological markers present in the patented hydrophilic extract of Polypodium leucotomos leaves (Fernblock®). The study demonstrated that Fernblock® is rich in phenolic compounds. Box 1 describes it in detail.
These markers are quantified in the phytoextract production quality control, ensuring that the production of different batches, with variations in seasonality, microclimate, and other conditions, offers products with the same efficacy and safety.
It is essential to highlight that the safety and efficacy studies presented in this article were conducted with the standardized hydrophilic extract of Polypodium leucotomos leaves, patented and called Fernblock®. Other Polypodium leucotomos extracts, derived from other parts of the plant (e.g., root) and with different extraction and standardization processes, are available in Brazil through manipulation by magistral pharmacies. Consequently, as a basic principle of phytopharmacology, it is not possible to compare the efficacy and safety of phytoextracts derived from diverse parts of the plant or different extraction and standardization processes.
In terms of pharmacokinetics, we know that PLE phenolic derivatives, when ingested, are rapidly absorbed and have their complete metabolism after 24 hours of oral administration. Intestinal absorption is highly efficient (between 70% and 100%). Regarding metabolism, coumaric, phenolic, and vanillic acids are metabolized in cytochrome P150, in the liver, with partial conjugation to derivatives with a plasma half-life between four and six hours.8
Toxicological safety assessment studies have been performed with PLE and are summarized below.
Carcinogenicity and mutagenicity studies, through the AIMES and the reverse mutation test, were performed and showed the absence of a mutagenic product effect.8
Studies conducted with animal species have shown absent oral toxicity in acute, subacute, and chronic doses.8
Studies to assess dermatotoxicity showed no effect of the extract when in contact with the skin and mucous membranes. Dermatotoxicity data are particularly relevant for the topical use of PLE.
In addition to preclinical studies, numerous clinical trials have been performed in over 50 years of scientific publications, all demonstrating a high safety profile for both topical and oral use.
Lastly, the pharmacovigilance data of the product, over more than 30 years of prescription and sale in the European market, demonstrate low rates of adverse events, usually related to transient and mild gastrointestinal symptoms, such as dyspepsia, stomach fullness sensation, nausea, and possible changes in intestinal flow.
Regarding Polypodium leucotomos topical use, its safety has also been well demonstrated, having been used in sunscreen formulations in Brazil and abroad for decades. In order for a cosmetic active to be used, it must be registered in the encyclopedia of cosmetic actives and receive an INCI (International Nomenclature of Cosmetic Ingredient) nomenclature. Polypodium leucotomos extract is registered under the INCI name “Polypodium Leucotomos Leaf Extract”.
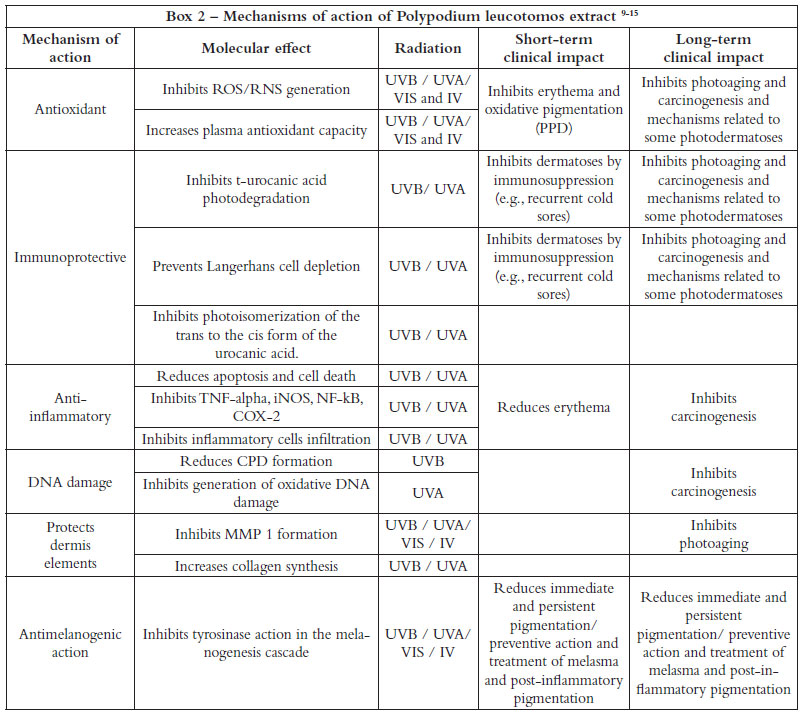
Despite the large number of publications identifying Polypodium leucotomos mechanisms of action, the effective participation of each mechanism against the effects of solar radiation is still not established.
In a didactic way, we can highlight six main mechanisms: antioxidant activity, photoimmunoprotective action, anti-inflammatory activity, dermis elements protection, and antipigmentary or melanogenesis inhibitor activity.
Box 2 presents, in a didactic way, the main mechanisms of action described in the literature.
The mechanisms highlighted in Box 2 benefit the treatment and prevention of different dermatological conditions, discussed below.
Sunburn prevention is possibly the most evident benefit of topical and oral photoprotection.
Regarding topical photoprotection, we know that the capacity of a sunscreen to protect against sunburn was the reason to develop these products, and it is, until today, the best and most used way to quantify the effectiveness of sunscreen through the determination of the sun protection factor (SPF).16
PLE oral use as an oral photoprotector also improves skin resistance to erythema production after exposure to ultraviolet radiation, demonstrated by increased minimum erythematous dose.
Middlekamp et al. demonstrated that volunteers treated with 7.5 mg/kg of PLE in a single dose, ingested between 30 minutes and three hours before exposure, showed a statistically significant growth in the minimum erythematous dose (MED), demonstrating an acute effect on protection against erythema.17
Schalka et al. evaluated volunteers who used PLE at a dose of 1000 mg daily (500 mg in the morning and 500 mg in the afternoon) for 28 days. The results showed a statistically significant reduction in MED after repeated use of the drug.18
Nestor et al. assessed healthy volunteers using PLE at a dose of 480 mg daily for 60 days and demonstrated reduced episodes of sunburn and increased MED.19 It is interesting to highlight that the photoprotective action of Polypodium leucotomos extract is well established in the literature against the effects of ultraviolet radiation and also against the effects of visible and infrared light.20,21
THe use of oral PLE during the summer period is well established in European countries as a way to add protection to topical sunscreen and minimize the risks of sun exposure, in particular, due to inadequate application and reapplication of sunscreen, resulting from the low amount of sunscreen application, lack of reapplication, and non-application in determined areas of the body (the recognized “forgotten areas” such as folds and ears).
In Brazil, dermatologists have also recommended the use of oral PLE during the period of more intense sun exposure.
Preventing skin aging is one of the main motivations for using sunscreens, particularly among younger people.
Regarding oral photoprotection, the prevention of skin aging could also be considered a motivation for its use.
Polypodium leucotomos extract demonstrates, through in vitro studies, efficacy in protecting the dermal structures of the extracellular matrix, such as collagen, elastin, glycosaminoglycans, and in inhibiting matrix metalanoproteinases and increased collagen synthesis.22
Its indication to prevent photoaging is already well established among Brazilian dermatologists.
Melasma is a very prevalent pigmentary dermatosis in Brazil, affecting mainly the face of young women, with enormous psychological and social discomfort.
In melasma pathophysiology, the participation of solar radiation is a triggering factor through the action of ultraviolet radiation and visible light.2
Any therapeutic plan for melasma demands photoprotection and recommends the use of topical sunscreens (preferably with protection against visible light) and oral photoprotection.1
Different studies show the benefit of PLE in reducing pigmentation and controlling melasma.
In the previously mentioned study, Schalka et al.18 demonstrated an increase in the minimum pigmentary dose (MPD) in volunteers treated with PLE at 1000 mg daily (500 mg in the morning and 500 mg in the afternoon) for 28 days. Increased MPD indicates higher resistance to pigmentation and, therefore, a protective effect.
Goh et al.23 demonstrated that Polypodium leucotomos extract at a dose of 480 mg daily combined with hydroquinone and topical sun protection for 90 days was superior (p<0.05) in the treatment of melasma compared to a placebo combined with the same association of hydroquinone and sunscreen, proven through the reduction of the Melasma Area and Severity Index (MASI).
In Brazil, oral Polypodium leucotomos in melasma is well established and one of its main indications by dermatologists.
We know that skin cancer is the most prevalent cancer of the human body. Among all environmental factors, solar radiation is the one that has the greatest relevance in triggering skin cancer, particularly keratinocyte skin cancer.
Thus, photoprotection is considered a central measure in skin cancer prevention, with the recommendation of daily use of sunscreens, especially in patients with a personal or family history of skin cancer.1
the daily oral use of Polypodium leucotomos extract has been proposed as a measure associated with topical photoprotection to prevent skin cancer.
Studies demonstrate that PLE inhibits the proliferation of epidermal cells, increasing the expression of the p53 tumor suppressor gene. A study in mice exposed to UVB radiation showed that animals treated with PLE reduced the appearance of skin cancer lesions.24,25
Another study randomized patients with actinic keratosis undergoing photodynamic therapy into two groups: PLE or placebo. At the end of the study, the authors observed that the group treated with PLE presented less recurrence of actinic keratoses than the control group after six months of photodynamic therapy sessions.26
Aguillera et al.27 investigated the possible role of a PLE extract to improve systemic photoprotection in patients at risk of developing melanoma. The authors analyzed the ability of PLE to reduce UV-induced erythema by determining the minimum erythematous dose (MED).
The study exposed 61 patients (20 with sporadic melanoma, 25 with multiple melanomas, and 16 with no history of melanoma) to UVB radiation. PLE improved photoprotection as evidenced by the MED increase of 30% in all patients. The use of PLE had a more significant effect on increasing MED in patients with familial melanoma than in patients with sporadic melanoma. These results are promising, suggesting the need for further studies with long-term administration of PLE in patients at high risk of developing melanoma.
Brazil has one of the highest levels of solar radiation throughout the year. Brazilians, even for cultural reasons, are used to exposing themselves to the sun in their daily or leisure activities since early childhood. Thus, the high incidence of skin cancer in the Brazilian population would not be surprising. Dermatologists recommend the introduction of the continued use of PLE to complement the use of sunscreens and contribute to the best complete photoprotection strategy.1
Ideally, oral photoprotection should be recommended throughout the year, as well as the use of sunscreens, considering the high levels of ultraviolet radiation even in the winter in Brazil.
Polypodium leucotomos has also been studied as a treatment for vitiligo. The antioxidant effects of PLE, as well as a shift from a Th1 cell cytokine profile to a Th2 cell cytokine profile with consequently decreased lL2, IFN-g, and TNF-alpha production and increased anti-inflammatory cytokine, IL 10, production, play a role in vitiligo treatment.24
Scientific publications show that the association between oral PLE 480 mg daily and narrowband UVB phototherapy (NB-UVB) is more effective in repigmentation than phototherapy alone, both in terms of extent and speed of treatment response.
Pacifico et al.28 published a study suggesting that oral PLE 480 mg daily in combination with NB-UVB was more effective in the repigmentation of patients with generalized vitiligo than treatment with twice-weekly NB-UVB alone (40% versus 22.4%, p<0,05). The authors concluded that oral PLE combined with NB-UVB improved response to treatment in terms of extent and speed of repigmentation.
Another study by Reyes et al.29 compared PUVA alone with PUVA associated with oral PLE to treat generalized vitiligo. This double blind clinical trial randomized 19 patients to receive PUVA alone or PUVA combined with oral PLE, and dermatologists assessed repigmentation rates. The authors found a higher rate of moderate to excellent repigmentation in the PUVA and oral PLE group compared to PUVA alone.
Middlekamp et al.30 investigated the effect of oral Polypodium leucotomos extract associated with narrowband UVB (NB-UVB) phototherapy on repigmentation in patients with vitiligo. The study randomized 50 patients to receive oral PLE at a dose of 250 mg twice daily or placebo, both associated with NB-UVB treatments twice weekly for 25-26 weeks and the primary outcome was the percentage of repigmentation in week 26.
Although they found no statistically significant difference, the authors observed higher repigmentation rates in the PLE group, specifically in the head and neck areas (44% versus 27%, p=0.06). The authors also showed that the lighter skin phototypes (I and II) showed a significant increase in repigmentation in the head and neck areas compared to the placebo group (47% versus 21%, p=0.01).
Polypodium leucotomos extract has been used to treat and prevent different photodermatoses or photoaggravated dermatoses, with particular emphasis on immune-mediated photodermatoses, including polymorphous light eruption, solar urticaria, chronic actinic dermatitis, and actinic prurigo.31,32,33
Regarding subacute cutaneous lupus erythematosus, a dermatosis aggravated by sun exposure, oral PLE has been reported as adjuvant therapy, with a clinical and histopathological improvement of lesions in the case reports described.34 Clearly, more studies are needed to confirm this finding.
Scientific publications,35,36,37,38 including case reports or small treated groups, have demonstrated the benefit of using Polypodium leucotomos extract in diseases such as psoriasis vulgaris, atopic dermatitis, and infectious dermatoses, among others. However, further clinical studies are necessary to demonstrate the product’s effectiveness for these indications.
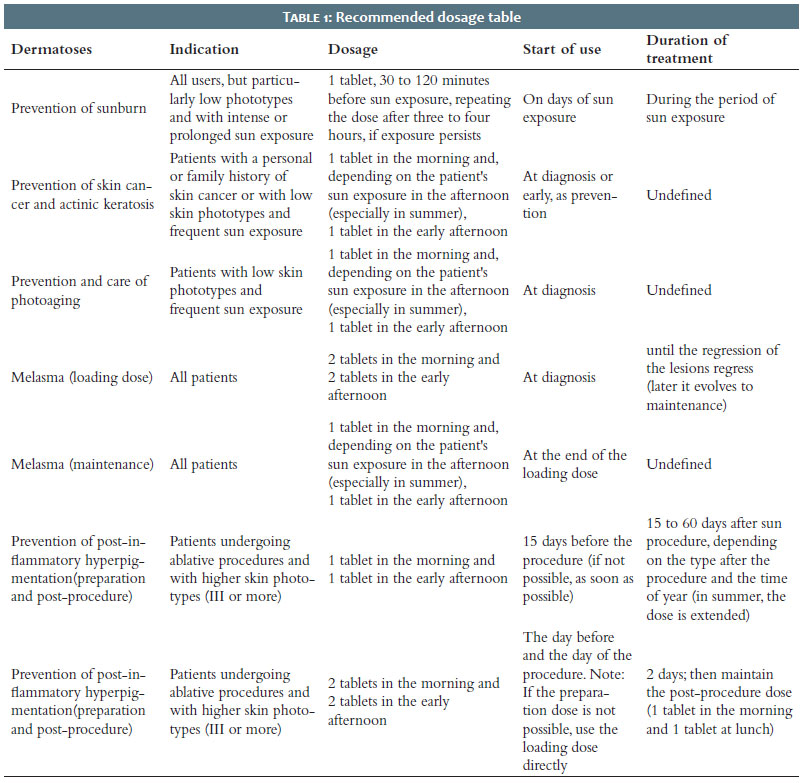
Clinical studies show that the action of oral Polypodium leucotomos can be effective in varying doses, between 250 mg (4 tablets) and 1 g a day, depending on the patient’s clinical condition and their sun exposure profile.8
Due to its rapid absorption and relatively short plasmatic half-life, oral administration of Polypodium leucotomos extract intrinsically relates to the user’s sun exposure.8
Thus, the usual recommendation is to take the medication about 30 to 60 minutes before the exposure begins and repeat it after approximately three to four hours in case sun exposure continues for longer periods.8,24
Therefore, from a practical point of view and the author’s experience, Table 1 shows the dosage recommendation for the most frequent indications.
A research comprising 40 years of scientific publication8 described no serious adverse events or toxicity reported. It assessed 19 human studies with 1016 treated patients and registered 16 adverse events reports (1.6%), mainly gastrointestinal disturbances or mild to moderate pruritus.
There are no reports of relevant drug interactions with the use of oral Polypodium leucotomos extract.
The topical use of Polypodium leucotomos extract, although initially proposed by Fitzpatrick et al.39 in the 1990s, was only considered and included in photoprotector sunscreen formulations in the 21st century.
Studies show that the topical action of PLE has the same molecular effects as the oral action, as Box 2 presents.
From a clinical point of view, its action adds efficacy to the photoprotective action of UV filters present in photoprotective formulations.
Schalka et al.,40 demonstrated in a recent publication, through a clinical and immunohistochemical study, that sunscreens containing PLE have a higher photoprotective effect, proven through the reduction of DNA damage markers (sunburn cells and p53), immunosuppression (Langerhans cells), dermal structures damage (MMP-1), and melanogenesis (antityrosinase action).
The study exposed volunteers to full-spectrum solar radiation (ultraviolet, visible light and infrared) in areas protected by SPF 90 sunscreen photoprotector containing 0.5% Polypodium leucotomos extract or SPF 90 photoprotective sunscreen formulation without PLE.
After 24 hours of irradiation, skin samples were extracted and sent for histopathology and immunohistochemistry.
The results demonstrated that the area protected by the product containing PLE showed lower cell damage due to radiation, lower DNA damage expression (20.18% lower p53 expression and 13.08% lower sunburn cells formation), lower collagen damage (lower expression of matrix metalloproteinase 1 – MMP1 – in 53.88%), lower immunesuppression effect (higher Langerhans cells preservation in 51.18%) and lower melanogenic effect (lower tyrosinase expression).
In the end, the authors concluded that adding 0.5% Polypodium leucotomos extract to the SPF 90 sunscreen formula enhanced protection against the cellular/molecular effects of full-spectrum solar radiation.
Polypodium leucotomos extract (Fernblock®) as an oral and/or topical photoprotector is well established among Brazilian dermatologists, contributing to a broad photoprotective strategy to prevent and treat photodermatoses or dermatoses aggravated by solar radiation.
The experience arising from the use of this active over the last ten years in Brazil corroborates and reinforces the results described in the international literature, demonstrating safety and efficacy in its oral and topical forms.
Sergio Schalka
ORCID: 0000-0003-2425-7962
Preparation and writing of the manuscript.
1. Schalka S, Steiner D, Ravelli FN, Steiner T, Terena AC, Marçon CR, et al; Brazilian Society of Dermatology. Brazilian consensus on photoprotection. An Bras Dermatol. 2014;89(6 Suppl 1):1-74.
2. Schalka S. New data on hyperpigmentation disorders. J Eur Acad Dermatol Venereol. 2017;31(Suppl 5):18-21.
3. González S, Aguilera J, Berman B, Calzavara-Pinton P, Gilaberte Y, Goh CL, et al. Expert recommendations on the evaluation of sunscreen efficacy and the beneficial role of non-filtering ingredients. Front Med (Lausanne). 2022;9:790207.
4. Padilla HC, Laínez H, Pacheco JA. A new agent (hydrophilic fraction of polypodium leucotomos) for management of psoriasis. Int J Dermatol. 1974;13(5):276-82.
5. Gonzalez S, Alonso-Lebrero JL, Del Rio R, Jaen P. Polypodium leucotomos extract: a nutraceutical with photoprotective properties. Drugs Today (Barc). 2007;43(7):475–85.
6. González S, Pathak MA. Inhibition of ultraviolet-induced formation of reactive oxygen species, lipid peroxidation, erythema and skin photosensitization by polypodium leucotomos. Photodermatol Photoimmunol Photomed. 1996;12(2):45-56.
7. Garcia F, Pivel JP, Guerrero A, Brieva A, Martinez-Alcazar MP, Caamano-Somoza M, et al. Phenolic components and antioxidant activity of Fernblock, an aqueous extract of the aerial parts of the fern Polypodium leucotomos. Methods Find Exp Clin Pharmacol. 2006;28(3):157-60.
8. Winkelmann RR, Del Rosso J, Rigel DS. Polypodium leucotomos extract: a status report on clinical efficacy and safety. J Drugs Dermatol. 2015;14(3):254-61.
9. Gombau L, García F, Lahoz A, Fabre M, Roda-Navarro P, Majano P, et al. Polypodium leucotomos extract: antioxidant activity and disposition. Toxicol In Vitro. 2006;20(4):464-71.
10. Alonso-Lebrero JL, Domínguez-Jiménez C, Tejedor R, Brieva A, Pivel JP. Photoprotective properties of a hydrophilic extract of the fern Polypodium leucotomos on human skin cells. J Photochem Photobiol B. 2003;70(1):31-7.
11. Philips N, Smith J, Keller T, Gonzalez S. Predominant effects of Polypodium leucotomos on membrane integrity, lipid peroxidation, and expression of elastin and matrixmetalloproteinase-1 in ultraviolet radiation exposed fibroblasts, and keratinocytes. J Dermatol Sci. 2003;32(1):1-9.
12. Capote R, Alonso-Lebrero JL, García F, Brieva A, Pivel JP, González S. Polypodium leucotomos extract inhibits trans-urocanic acid photoisomerization and photodecomposition. J Photochem Photobiol B. 2006;82(3):173-9.
13. Zattra E, Coleman C, Arad S, Helms E, Levine D, Bord E, et al. Polypodium leucotomos extract decreases UV-induced Cox-2 expression and inflammation, enhances DNA repair, and decreases mutagenesis in hairless mice. Am J Pathol. 2009;175(5):1952-61.
14. Parrado C, Mascaraque M, Gilaberte Y, Juarranz A, Gonzalez S. Fernblock (Polypodium leucotomos Extract): Molecular Mechanisms and Pleiotropic Effects in Light-Related Skin Conditions, Photoaging and Skin Cancers, a Review. Int J Mol Sci. 2016;17(7):1026.
15. Gonzalez S, Alcaraz MV, Cuevas J, Perez M, Jaen P, Alvarez-Mon M, et al. An extract of the fern Polypodium leucotomos (Difur) modulates Th1/Th2 cytokines balance in vitro and appears to exhibit anti-angiogenic activities in vivo: pathogenic relationships and therapeutic implications. Anticancer Res. 2000;20(3A):1567-75.
16. Schalka S, Reis VMS. Sun protection factor: meaning and controversies. An Bras Dermatol. 2011;86(3):507-15.
17. Middelkamp-Hup MA, Pathak MA, Parrado C, Goukassian D, Rius-Díaz F, Mihm MC, et al. Oral Polypodium leucotomos extract decreases ultraviolet-induced damage of human skin. J Am Acad Dermatol. 2004;51(6):910-8
18. Schalka S, Vitale-Villarejo MA; Agelune CM; Bombarda PCP. The benefits of using a compound containing Polypodium leucotomos extract for reducing erythema and pigmentation resulting from ultraviolet radiation. Surg Cosmet Dermatol. 214;6(4):344-8.
19. Nestor MS, Berman B, Swenson N. Safety and efficacy of oral Polypodium leucotomos extract in healthy adult subjects. J Clin Aesthet Dermatol. 2015;8(2):19-23.
20. Pourang A, Dourra M, Ezekwe N, Kohli I, Hamzavi I, Lim HW. The potential effect of Polypodium leucotomos extract on ultraviolet- and visible light- induced photoaging. Photochem Photobiol Sci. 2021;20(9):1229-38.
21. Zamarrón A, Lorrio S, González S, Juarranz À. Fernblock prevents dermal cell damage induced by visible and infrared a radiation. Int J Mol Sci. 2018;19(8):2250.
22. Parrado C, Mascaraque M, Gilaberte Y, Juarranz A, Gonzalez S. Fernblock (Polypodium leucotomos Extract): molecular mechanisms and pleiotropic effects in light-related skin conditions, photoaging and skin cancers, a review. Int J Mol Sci. 2016;17(7):1026.
23. Goh CL, Chuah SY, Tien S, Thng G, Vitale MA, Delgado-Rubin A. Double-blind, placebo-controlled trial to evaluate the effectiveness of Polypodium Leucotomos extract in the treatment of melasma in asian skin: A Pilot Study. J Clin Aesthet Dermatol. 2018;11(3):14-9.
24. Choudhry SZ, Bhatia N, Ceilley R, Hougeir F, Lieberman R, Hamzavi I, et al. Role of oral Polypodium leucotomos extract in dermatologic diseases: a review of the literature. J Drugs Dermatol. 2014;13(2):148-53.
25. Rodríguez-Yanes E, Cuevas J, González S, Mallol J. Oral administration of Polypodium leucotomos delays skin tumor development and increases epidermal p53 expression and the anti-oxidant status of UV-irradiated hairless mice. Exp Dermatol. 2014;23(7):526-8.
26. Auriemma M, Di Nicola M, Gonzalez S, Piaserico S, Capo A, Amerio P. Polypodium leucotomos supplementation in the treatment of scalp actinic keratosis: could it improve the efficacy of photodynamic therapy? Dermatol Surg. 2015;41(8):898-902.
27. Aguilera P, Carrera C, Puig-Butille JA, Badenas C, Lecha M, González S, et al. Benefits of oral Polypodium Leucotomos extract in MM high-risk patients. J Eur Acad Dermatol Venereol. 2013;27(9):1095-100.
28. Pacifico A, Iacovelli P, Paro Vidolin A, Leone G. Combined treatment of NBUVB phototherapy and oral Polypodium Leucotomos extract versus NBUVB therapy alone in the treatment of patients with vitiligo. Poster #3111. Paper presented at: American Academy of Dermatology; March 2009; San Francisco, CA.
29. Reyes E, Jaén P, Heras E, Carrión F, Alvarez-Mon M, Eusebio E, et al. Systemic immunomodulatory effects of Polypodium leucotomos as an adjuvant to PUVA therapy in generalized vitiligo: a pilot study. J Dermatol Sci. 2006;41(3):213-6.
30. Middelkamp-Hup MA, Bos JD, Rius-Diaz F, Gonzalez S, Westerhof W. Treatment of vitiligo vulgaris with narrow-band UVB and oral Polypodium leucotomos extract: a randomized double-blind placebo-controlled study. J Eur Acad Dermatol Venereol. 2007;21(7):942-50.
31. Caccialanza M, Percivalle S, Piccinno R, Brambilla R. Photoprotective activity of oral polypodium leucotomos extract in 25 patients with idiopathic photodermatoses. Photodermatol Photoimmunol Photomed. 2007;23(1):46-7.
32. Caccialanza M, Recalcati S, Piccinno R. Oral polypodium leucotomos extract photoprotective activity in 57 patients with idiopathic photodermatoses. G Ital Dermatol Venereol. 2011;146(2):85-7.
33. Tanew A, Radakovic S, Gonzalez S, Venturini M, Calzavara-Pinton P. Oral administration of a hydrophilic extract of Polypodium leucotomos for the prevention of polymorphic light eruption. J Am Acad Dermatol. 2012;66(1):58-62.
34. Breithaupt AD, Jacob SE. Subacute cutaneous lupus erythematosus: a case report of Polypodium leucotomos as an adjuvant therapy. Cutis. 2012;89(4):183-4.
35. Heras ME, Ledo E, Gonzalez S. Polypodium leucotomos extract as adjuvant to PUVA therapy in the treatment of Plaque Psoriasis. Med Cutan Iber Lat Am. 1997;25:103-7.
36. Middelkamp-Hup MA, Pathak MA, Parrado C, Garcia-Caballero T, Rius-Díaz F, Fitzpatrick TB, et al. Orally administered Polypodium leucotomos extract decreases psoralen-UVA-induced phototoxicity, pigmentation, and damage of human skin. J Am Acad Dermatol. 2004;50(1):41-9.
37. Ramírez-Bosca A, Zapater P, Betlloch I, Albero F, Martínez A, Díaz-Alperi J, et al; Grupo de Anapsos en Dermatitis Atópica y centros de realización del estudio. Polypodium leucotomos extract in atopic dermatitis: a randomized, double-blind, placebo-controlled, multicenter trial. Actas Dermosifiliogr. 2012;103(7):599-607.
38. Solivellas BM, Martín TC. Polypodium leucotomos extract use to prevent and reduce the risk of infectious diseases in high performance athletes. Infect Drug Resist. 2012;5:149-53.
39. González S, Pathak MA, Cuevas J, Villarrubia VG, Fitzpatrick TB. Topical or oral administration with an extract of Polypodium leucotomos prevents acute sunburn and psoralen-induced phototoxic reactions as well as depletion of Langerhans cells in human skin. Photodermatol Photoimmunol Photomed. 1997;13(1-2):50-60.
40. Schalka S, Donato LC. Evaluation of effectiveness of a sunscreen containing Polypodium leucotomos extract in reducing the sun damage to the skin. Surg Cosmet Dermatol. 2019;11(4):310-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}