


Vivian de Carvalho Amaral1; Fernanda Aquino Cavallieri2
Submitted on: 14/10/2022
Approved on: 14/06/2023
Financial support: None
Conflict of interest: None
How to cite this article: Amaral VC. K.I.S.S. Lip Filler Technique - keeping injections simple and safe when filling lips. Surg Cosmet Dermatol. 2023;15:e20230187.
To simplify the procedure and increase lip augmentation safety, we have developed the KISS - Keep Injection Simple and Safe lip filler technique. To be simple, the method recommends only the evaluation of four anatomical parameters and the filling of five labial areas. To be safe, the injection is performed only in the supramuscular plane, using cannulas with a blunt tip, inserted in four entries: two in the upper lip and two in the lower lip. Fillers are injected in specific anatomical vectors for lips volumization, projection, contour improvement, and support of cupid’s bow and lip corners.
Keywords: Hyaluronic acid; Dermal fillers; Lip
Full lips have are with youth and beauty. Therefore, lip augmentation (LA) using hyaluronic acid (HA) is one of the most requested procedures.1 However, the need to assess multiple anatomical parameters for the aesthetic analysis of the lips, associated with the intense vascular variability of the area, makes the procedure challenging regarding lip analysis and choice of injection sites.
In the last year, we developed and used a simple model for augmenting the lip vermillion in two steps: the first is the analysis of four anatomical parameters for planning the injections, and the second is the injection itself, in five labial areas, always prioritizing the plans considered safer.
We named the model K.I.S.S. Technique, designed to deliver excellent results, keeping lip injections simple and safe.
We assessed the following lip parameters of 20 women, aged between 25 and 45 years, for LA planning:
- Height of the filter columns (FC): if longer than 1.5 cm, augmentation would not be conducted in the area;
- Height of the upper (UL) and lower (LL) lips: UL smaller than 0.8 cm and LL smaller than 0.9 cm were considered thin and were injected;
- Anterior projection of the UL in profile: it should be about 2 mm more projected concerning the LL;
- Volume ratio between UP and LL: the UL should have about 80% of the volume of the LL.
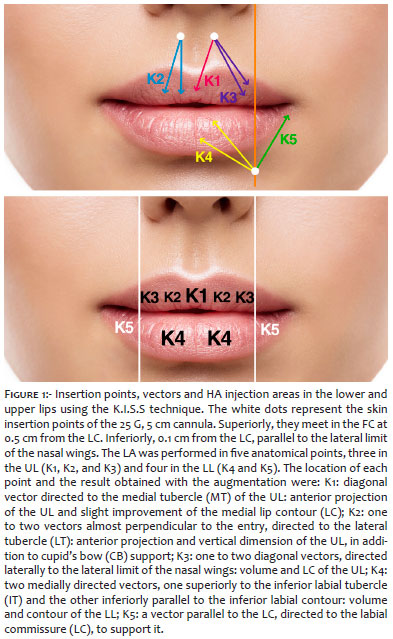
After adequate asepsis, we applied four anesthetic buttons with 1% lidocaine, 0.5 cm from the labial contour, one in each FC, superiorly, and one in each line parallel to the lateral limit of the nasal alae, inferiorly (Figure 1). Each anesthetized point corresponded to an entry where we inserted a 25 G, 5 cm cannula and injected HA in the superficial plane by retroinjection.
We performed the LA in five anatomical points, three in the UL, which we named K1, K2, and K3, and two in the LL, which we called K4 and K5 (Figures 2 and 3). The location of each point and the result obtained by its augmentation were as follows:
- K1: diagonal vector directed to the medial tubercle (MT) of the UL: anterior projection of the UL and slight improvement of the medial lip contour (LC);
- K2: one to two vectors almost perpendicular to the entry, directed to the lateral tubercle (LT): anterior projection and vertical dimension of the UL, in addition to cupid’s bow (CB) support;
- K3: one to two diagonal vectors, directed laterally to the lateral limit of the nasal wings: volume and LC of the UL;
- K4: two medially directed vectors, one superiorly to the inferior labial tubercle (IT) and the other inferiorly parallel to the inferior labial contour: volume and contour of the LL;
- K5: a vector parallel to the LC, directed to the labial commissure (LC) to support it.
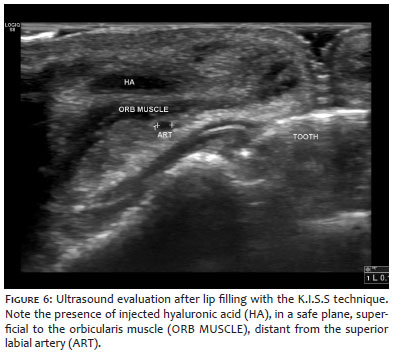
All patients were satisfied with the aesthetic result (Figures 4, 5, and 6). The major intercurrences reported were ecchymosis at the entry and edema, which resolved spontaneously within seven days. Three patients developed nodules due to local product accumulation, which resolved with a vigorous local massage.
Optimizing the aesthetic results of LA with HA requires an individualized treatment approach, with the skillful application of an appropriate injection technique, based on anatomical knowledge, for minimal risks of adverse events.1
A combination of proportion, definition, and volume determines the relative attractiveness of the lips.3 These are essential anatomical parameters that should guide the procedure to avoid unsightly results include:
- The vermilion vertical dimension of the UL must be between 8.5 mm and 9 mm, while the LL must be between 9.5 mm and 10 mm, increasing a few mm at the IT level;4
- The volume of the UL vermilion should be 75% to 80% from the LL, following the golden ratio;4, 1
- The anterior protrusion of the UL should be 1.5 mm to 2 mm greater than that of the LL;4
- The height of the FCs should ideally be between 12 mm and 15 mm.4
Injections that do not meet these criteria can make the already long FC more evident, projecting the already anterior UL, thus bringing an unsightly “duckbill” appearance, or causing excessive volumization, leading the lips to acquire a “sausage-like” shape.
Complications that are even more serious than unaesthetic outcomes include vascular impairments, which can progress to skin necrosis and blindness.5
The lips’ arterial supply presents marked anatomical variations, even when comparing the sides of the face in the same person.6 The most frequent location of the superior and inferior labial arteries was the submucosal plane (58.5%), followed by the intramuscular planes (36.2%) and subcutaneous (5.3%).7
Dissections6 and ultrasound analysis7 suggested that a superficial injection plane, about 4 mm away from the vermilion/mucosal junction, would therefore be the safest area for LA.6, 7, 8 Also, the perpendicular approach to the labial vermilion (from the cutaneous lip) could also increase safety, as the artery is located more frequently in this area.7 Deep injection between the muscular layer and the mucosa, mainly of the UL, should be avoided.9
To increase the safety of the procedure, in addition to essential anatomical knowledge, blunt-tipped microcannulas for LA can be used.10 In addition to safety, microcannulas usually produce less bruising and less pain, with faster post-fill recovery.11
We know that lip augmentation cannot be standardized. Thus, we present an individual analysis and injection model. We also know that lip vascular variability brings many risks to the procedure. Therefore, we also propose that the injection is performed through microcannulas with a blunt tip, only in the safest labial anatomical sites, even if we lose technical refinements, apparently unnoticeable to lay eyes since we could observe a high degree of satisfaction on the part of the patients.
Finally, although the technique does not include the perioral region treatment, approaching this region is often fundamental, especially in older patients, to achieve an excellent aesthetic result.
Vivian de Carvalho Amaral
ORCID: 0000-0002-5379-652X
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Fernanda Aquino Cavallieri
ORCID: 0000-0002-9465-3744
Approval of the final version of the manuscript; obtaining, analyzing and interpreting data; critical review of the manuscript.
1. Sarnoff DS, Gotkin RH. Six steps to the "perfect" lip. J Drugs Dermatol. 2012;11(9):1081-8.
2. Smith SR, Lin X, Shamban A. Small gel particle hyaluronic acid injection technique for lip augmentation. J Drugs Dermatol. 2013;12(7):764-9.
3. Hoefflin SM. The definition of facial beauty. In: Panfilov DE, ed. Aesthetic surgery of the facial mosaic. Berlin, Heidelberg: Springer; 2006:43-51.
4. Sito G, Consolini L, Trévidic P. Proposed guide to lip treatment in caucasian women using objective and measurable parameters. Aesthet Surg J. 2019;39(12):NP474-NP83.
5. Samizadeh S, Pirayesh A, Bertossi D. Anatomical variations in the course of labial arteries: a literature review. Aesthet Surg J. 2019;39(11):1225-1235. Erratum in: Aesthet Surg J. 201913;39(12):NP555.
6. Cotofana S, Alfertshofer M, Schenck TL, Bertucci V, Beleznay K, Ascher B, et al. Anatomy of the superior and inferior labial arteries revised: an ultrasound investigation and implication for lip volumization. Aesthet Surg J. 2020;40(12):1327-35.
7. Mohanty SR, Panigrahi M, Upadhyaya J. Descriptive study on vascular anatomy of the upper lip. Aesthetic Plast Surg. 2022;46(5):2248-57.
8. Trévidic P, Criollo-Lamilla G. French kiss technique: an anatomical study and description of a new method for safe lip eversion. Dermatol Surg. 2020;46(11):1410-7.
9. Tansatit T, Apinuntrum P, Phetudom T. A typical pattern of the labial arteries with implication for lip augmentation with injectable fillers. Aesthetic Plast Surg. 2014;38(6):1083-9.
10. Chopra R, Graivier M, Fabi S, Nestor M, Meuse P, Mashburn J. A Multi-center, Open-label, prospective study of cannula injection of small-particle hyaluronic acid plus lidocaine (SPHAL) for lip augmentation. J Drugs Dermatol. 2018;17(1):10-6.
11. Fulton J, Caperton C, Weinkle S, Dewandre L. Filler injections with the blunt-tip microcannula. J Drugs Dermatol. 2012;11(9):1098-103.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}